ABSTRACT
INTRODUCTION: Pain control is essential in any surgical event. Liposuction is, in general, accompanied by complaints of post-operative pain, which raises the discussion about the best way to prevent and treat it. Accordingly, studies indicate that the analgesia should begin before any painful stimulus is triggered in order to reduce or prevent the pain preemptively. The approach of the various pain pathways, with a combination of different classes of drugs or utilization of spinal block or epidural/general anesthesia can also contribute to pain management.
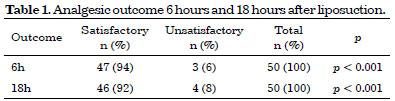
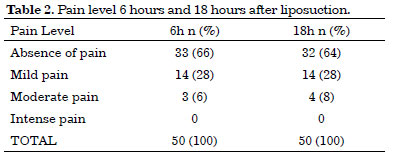
METHODS: A descriptive, prospective, interventional cohort type study was conducted with patients undergoing plastic surgery involving liposuction. The standard anesthetic procedure consisted of an association between general and spinal anesthesia. The assessment of pain, carried out 6 and 18 hours after the end of the surgery, used unidimensional scales. The absence of pain or the presence of mild pain was considered a satisfactory result.
RESULTS: Fifty female patients were evaluated, with an average of 35 years of age. No intense pain was found at any time during the study. Satisfactory results accounted for 94% and 92% of the patients in the assessment at 6 and 18 hours post-surgery, respectively (p < 0.001).
CONCLUSIONS: Intravenous anesthesia combined with spinal anesthesia, in body contouring surgery, was able to satisfactorily control pain in the immediate postoperative period in most cases (>90%). In this study, liposuction was revealed to be a type of surgery with manageable pain.
Keywords:
Analgesia; Lipectomy; General anesthesia; Spinal anesthesia; Pain, postoperative.
RESUMO
INTRODUÇÃO: O controle da dor é essencial em qualquer evento cirúrgico. A lipoaspiração cursa, em geral, com queixas de dor pós-operatória, o que levanta a discussão acerca da melhor maneira de preveni-la e tratá-la. Dessa forma, estudos indicam que a analgesia deveria começar antes que qualquer estímulo doloroso seja deflagrado a fim de reduzir ou prevenir a dor preemptivamente. A abordagem nas diversas vias álgicas, com combinação de diferentes classes de fármacos ou associação dos bloqueios raquimedular ou epidural com anestesia geral, também pode contribuir para o manejo da dor.
MÉTODOS: Estudo descritivo, prospectivo, intervencionista, tipo Coorte, com pacientes submetidas à cirurgia plástica envolvendo lipoaspiração. O procedimento anestésico padrão consistiu na associação de anestesia geral e subaracnóidea. O escalonamento da dor, realizado 6 e 18 horas após o término da cirurgia, utilizou escalas unidimensionais. A ausência de dor ou a presença de dor leve foram consideradas como resultado satisfatório.
RESULTADOS: Foram avaliadas 50 pacientes do sexo feminino, com média de 35 anos de idade. Não foi encontrada dor severa em qualquer momento do estudo. Os resultados satisfatórios representaram 94% e 92% das pacientes na avaliação das 6 e 18 horas do pós-operatório, respectivamente (p < 0,001).
CONCLUSÕES: A anestesia geral venosa combinada com raquianestesia, em cirurgia de contorno corporal, foi capaz de controlar satisfatoriamente a dor no pós-operatório imediato na maioria dos casos (>90%). A lipoaspiração mostrou ser cirurgia de dor controlável nesta casuística.
Palavras-chave:
Analgesia; Lipectomia; Anestesia geral; Raquianestesia; Dor pós-operatória.