ISSN Online: 2177-1235 | ISSN Print: 1983-5175
Retrospective analysis of the approach to nasal fractures at Unicamp Clinical Hospital
Estudo retrospectivo da abordagem das fraturas nasais no Hospital de Clínicas da Unicamp
Original Article -
Year2011 -
Volume26 -
Issue
4
Bruna Borghese1; Davi Reis Calderoni2; Luis Augusto Passeri3
ABSTRACT
INTRODUCTION: Nasal fractures are common injuries, frequently considered to be minor. Nevertheless, they may cause significant damage, from both a functional and aesthetic perspective.
METHODS: Medical records of 144 patients admitted for nasal fracture treatment between February 2002 and October 2008 to the Plastic Surgery Area of the Unicamp Clinical Hospital were analyzed.
RESULTS: Patients were predominantly male (75.7%), with a male to female ratio of 3.1:1. The most number of cases was observed in 21 to 30 year olds, and the majority of fractures (31.8%) were caused by physical aggression. Closed reductions were performed on all patients under local and topical anesthesia after an average of 8 days. Among the studied patients, 31 experienced residual deformity.
CONCLUSIONS: Patients typically affected by nasal fractures are young male adults. Closed reduction surgical treatment yields acceptable results, with correct injury evaluation and treatment timing.
Keywords:
Nose/surgery. Nasal bone/injuries. Facial injuries.
RESUMO
INTRODUÇÃO: As fraturas nasais são lesões de grande incidência, frequentemente consideradas de menor importância. No entanto, podem trazer prejuízos importantes do ponto de vista tanto funcional como estético.
MÉTODO: Foram analisados prontuários médicos de 144 pacientes submetidos a tratamento de fratura nasal na Área de Cirurgia Plástica do Hospital de Clínicas da Unicamp, no período de fevereiro de 2002 a outubro de 2008.
RESULTADOS: Observou-se predomínio de pacientes do gênero masculino (75,7%), com proporção entre gêneros masculino e feminino de 3,1:1. A faixa etária mais acometida foi aquela entre 21 anos e 30 anos de idade. A maioria das fraturas (31,8%) foi causada por agressão física. Todos os pacientes foram tratados por meio de redução fechada, sob anestesia local e tópica, após um período médio de 8 dias. Entre os pacientes analisados, 13 evoluíram com deformidade residual.
CONCLUSÕES: O paciente tipicamente afetado pelas fraturas nasais é o indivíduo adulto jovem e do gênero masculino. O tratamento cirúrgico por meio de redução fechada promove resultados aceitáveis, se respeitados os princípios de avaliação correta da lesão e do momento de indicação do tratamento.
Palavras-chave:
Nariz/cirurgia. Osso nasal/lesões. Traumatismos faciais.
INTRODUCTION
Nasal fractures are the most common facial fracture and the third most common fracture in the human body1-4. This is due to the fact that less force is required to cause a nasal fracture than other facial fractures, and the nose is in a prominent position on the face2,4. Despite their frequency of occurrence, few studies about nasal fractures are available, especially studies conducted in Brazil.
Although considered to be less complex injuries, nasal fractures have significant implications, both from aesthetic and functional perspectives. This fact may be appreciated by residual nasal deformity rates, found in some studies to be 50%1,2. Some of the factors that contribute to undesirable aesthetic and functional results include edema, a prolonged period of time between the trauma and surgical treatment, the presence of an undetected previous nasal deformity, and undiagnosed septal injury/deformity2. Bone fractures are commonly followed by cartilaginous and septal injuries, since these structures are closely connected4.
From a functional perspective, it is known that obstructive symptoms are frequently observed. However, emphasis has been placed on the objective evaluation of these symptoms only recently. After evaluating nasal cavity patency by measuring the average cross-sectional area by acoustic rhinometry, a reduction from 15% to 36% after nasal fractures was detected. This reduction represented improvement after appropriate fracture treatment, with consequent functional relief5.
Currently, there is also debate over the most appropriate surgical timing and technique. It is believed that the decision should be based on variables such as injury complexity, the presence of other facial fractures, the patient's adherence to treatment, and the presence of septal injury4. There are three fundamental aspects that should be considered during treatment planning: (a) the amount of time between trauma and reduction, (b) the type of anesthesia (local vs. general), and (c) the surgical technique (opened vs. closed) 6,7. Except for drainage of a septal hematoma, which should be immediate, fractures may be treated between 10 and 14 days after the trauma1-3. The most common treatment for nasal fractures is closed reduction surgery with local anesthesia, and the result is frequently considered satisfactory by both physicians and patients3.
METHODS
This study retrospectively analyzed data from 144 patients with nasal fractures who were admitted for surgical treatment to the Plastic Surgery Area of the Clinical Hospital of the Universidade Estadual de Campinas (Unicamp) between February 2002 and October 2008. A review of medical records yielded demographic information related to medical visits, surgical procedures, and post-operative follow-ups.
Surgical Procedure
All patients in the study were admitted for closed reduction surgical treatment of their nasal fractures. Local anesthesia consisted of a 2% lidocaine with adrenaline solution at a concentration of 1:200.000. Infraorbital nerve blocks were followed by paranasal infiltration. Anesthesia was complemented by intranasal topical instillation of a 10% lidocaine spray.
Asch or Walsham forceps were used to perform the fracture reduction. An intranasal buffer was indicated in patients who presented instability of the fractured segments. After the procedure, a plaster dressing was applied over the nasal dorsum, tied with a micropore tape and worn for 7 days.
Statistical Analysis
Statistical analysis was performed using the BioEstat 5.0 program. The adopted statistical significance level was P < 0.05.
RESULTS
The medical records of 144 patients who underwent closed reduction surgery with local anesthesia were analyzed.
Patients were predominantly male, representing 75.7% of the total. The ratio between male and female patients was 3.1:1 (p < 0.0001). With respect to ethnicity, 79% of patients were Caucasian (Figure 1). Patient ages ranged from 2 to 78 years, with an average age of 26.3 years and a median age of 23 years. Most injuries occurred among 21 to 30 year olds (36.8%), followed closely by 11 to 20 year olds (35.4%) (Figure 2).

Figure 1 - Distribution of patients by race.

Figure 2 - Distribution by age.
With respect to the trauma mechanism, most fractures resulted from physical aggression (31.8%), followed by sports accidents (21.6%) and automobile accidents (13.6%) (Figure 3). From a clinical perspective, deviation of the nasal pyramid (crooked nose), presence of ecchymosis/hematoma, and local pain were most prevalent (Figure 4).

Figure 3 - Distribution of fractures according to trauma mechanism (n = 88).
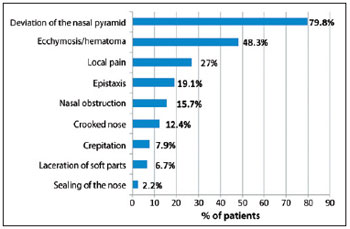
Figure 4 - Clinical problems (n = 89).
Injuries associated with nasal trauma occurred in 18 (12.5%) patients. In 77.8% of these patients, injuries also resulted in the fracture of other skull bones, including the orbital wall (9 patients), jaw (4 patients), and zygomatic bone (1 patient).
In all cases, patients were treated surgically using the technique previously described. The average period between trauma and surgical treatment was 8 days, with a median of 7 days and an interval ranging from 1 to 26 days.
Among the studied patients, 56 had records of proper post-operative follow-up, which allowed complications to be identified and evaluated. Complications were present in 20 patients, with 13 (23.2%) cases of residual deformity and 5 (8.9%) cases of persistent nasal obstruction. Local infection and anosmia occurred in 1 patient each. Rhinoplasty was performed on 6 patients to correct persistent deformity. The average period between trauma and surgical reduction for patients presenting complications was 10 days, and there was no statistically significant difference in relation to the period observed in cases without complications.
DISCUSSION
Nasal bone fractures, commonly seen in clinical practice1-4, are frequently considered minor injuries. Nevertheless, they present significant potential for aesthetic and functional complications1-3.
From a demographic perspective, patients in this study were predominantly male, with a male-female ratio of 3.1:1 (P < 0.0001), and an average age of 26.3 years. This data coincides with a majority of previous studies, including studies specifically about nasal trauma7-10 and traumas affecting other areas of the face11-14. Data presented in this study corroborate the fact that nasal trauma and general facial trauma are common injuries among young male individuals who are economically independent. The most frequent fracture mechanism was physical aggression, followed by sports accidents. Thus, the etiological pattern of the nasal fractures also coincides with previous reports, with low energy impacts such as physical aggression9,15 and falls7,8,10 being most frequent.
Disregarding patients with non-defined trauma etiology reported in Figure 3 as "Unknown" and "Others," low energy traumas correspond to 61.4% of the nasal fractures. This reflects the anatomical characteristics of the nasal bones, which, due to their reduced thickness, require less force to be fractured. Also, considering that the population studied consists of patients admitted for surgical fracture treatment, it calls for even more attention to be paid to the significant predominance of low energy mechanisms resulting in fractures. At the outset, these patients were considered to have had more serious injuries, which drove the need for surgical reduction. Thus, nasal deviation occurred in about 80% of the cases.
In terms of clinical presentation, the alteration pattern was similar to the one previously reported by other authors7,8, with nasal deviation occurring most frequently. This is mainly due to the fact that the studied population consisted predominantly of patients admitted for surgical treatment of deformities resulting from nasal fractures.
In 110 cases, it was possible to obtain information on the occurrence of injuries associated with the nasal fractures. Among patients for whom there was available information, 18 (16.4%) presented some associated injury, with injuries in the cephalic segment being most common. Previous studies demonstrated disparate incidences of associated trauma, ranging from 4.2%7 to 27%8, which were always head injuries consisting mainly of other facial fractures. However, it is noteworthy that 55.6% of patients with associated injuries presented with polytraumatism affecting other body segments.
This inversion of the trauma mechanism pattern is also present among patients with associated traumas. Considering the study population as a whole, automobile accidents caused 28.4% of the injuries. Nevertheless, in the subgroup of patients with other injuries in addition to nasal fracture, this percentage increased to 55.5%, making automobile accidents the most common cause. This association refers, once again, to the need to obtain an accurate story with respect to trauma etiology; such information should raise suspicions and substantiate further clinical evaluation and investigation (e.g., by imaging) in order to determine other areas that may be affected.
Controversy also exists about several aspects of nasal fracture treatment, such as the timing of reduction surgery, the approach (open or closed), and the type of anesthesia to be used. In this study, all patients were treated with closed surgical reduction of the fractures under local anesthesia. The treatment was carried out after an average of 8 days.
Despite the existence of small variations, the literature predominantly recommends postponing surgical nasal fracture reduction treatment until local edema is reduced, except in cases where a patient is evaluated immediately after the trauma and edema has not completely developed. Recent reviews are unanimous regarding the necessity of waiting until a comprehensive evaluation of the nasal deformity is possible1,2,4,6,16. Based on these studies, reduction should be ideally performed, on average, within 2 weeks after the trauma; in general, this occurs within 5 to 10 days. This procedure allows for proper mobilization of the fractured segments, and reduces the need for additional interventions to correct residual deformities3.
With respect to the type of anesthesia to be used, in this study local anesthesia was chosen, using lidocaine with infraorbital nerve block and infiltration around the nose, complemented by intranasal topical anesthesia with lidocaine spray. There is debate in the literature over the type of anesthesia to be used. Some authors defend the use of general anesthesia2,10,17, arguing that it allows for intranasal examination and surgical manipulation without patient reaction and provides more comfort. However, a majority of studies demonstrate that nasal fracture reduction is feasible using local anesthesia, with high rates of patient satisfaction7,15. Our results also support the adequacy of local anesthesia combined with topical anesthesia, which provides the benefit of being able to perform the procedure at an outpatient clinic without having to hospitalize individuals. Recent broad reviews of the literature examining this issue concluded that nasal fracture manipulation under local anesthesia yields acceptable results in terms of patient comfort and aesthetic and functional results18.
Closed reduction is the most frequently used nasal fracture treatment during the acute phase, being generally well accepted in terms of results2,3,7,8,10,19. However, the treatment success rate reported in the literature is variable, with residual deformities occurring in 2-50% of cases2,3,10,15,17,19. This high variability is due to factors such as patient type, evaluation method, and treatment planning. Detailed internal nasal evaluation, with the main goal of detecting septum alterations, is considered essential, greatly influencing the result, since inappropriate treatment of the septum frequently damages the final nose shape1,2.
In this study, all patients underwent closed reduction surgery. Among the 56 patients for whom there was adequate information, there were 13 (23%) cases of residual deformity based on later evaluation of the nose shape in the records. This number corresponds to previous observations. It is noteworthy that proper patient follow-up can be difficult, a fact observed in other studies regarding facial trauma5,20. However, it is highly probable that the patients who did not follow the correct procedure did not experience significant residual deformities. Thus, the actual incidence of residual deformities would tend to be lower than the observed one.
CONCLUSIONS
Nasal fractures are associated with young male individuals and situations involving physical aggression. Although they tend to occur in isolation, that is, without associated injuries, attention should be paid to cases of polytraumatization, where the diagnosis of nasal fractures could be neglected.
Treatment via closed reduction with local anesthesia is feasible and yields proper results. Therefore, factors like proper evaluation of the extent of the fracture and correct treatment timing should be respected.
REFERENCES
1. Ziccardi VB, Braidy H. Management of nasal fractures. Oral Maxillofac Surg Clin North Am. 2009;21(2):203-8.
2. Rohrich RJ, Adams WP Jr. Nasal fracture management: minimizing secondary nasal deformities. Plast Reconstr Surg. 2000;106(2):266-73.
3. Fattahi T, Steinberg B, Fernandes R, Mohan M, Reitter E. Repair of nasal complex fractures and the need for secondary septo-rhinoplasty. J Oral Maxillofac Surg. 2006;64(12):1785-9.
4. Rubinstein B, Strong EB. Management of nasal fractures. Arch Fam Med. 2000;9(8):738-42.
5. Chun KW, Han SK, Kim SB, Kim WK. Influence of nasal bone fracture and its reduction on the airway. Ann Plast Surg. 2009;63(1):63-6.
6. Mondin V, Rinaldo A, Ferlito A. Management of nasal bone fractures. Am J Otolaryngol. 2005;26(3):181-5.
7. Ridder GJ, Boedeker CC, Fradis M, Schipper J. Technique and timing for closed reduction of isolated nasal fractures: a retrospective study. Ear Nose Throat J. 2002;81(1):49-54.
8. Hwang K, You SH, Kim SG, Lee SI. Analysis of nasal bone fractures; a six-year study of 503 patients. J Craniofac Surg. 2006;17(2):261-4.
9. Fornazieri MA, Yamaguti HY, Moreira JH, Navarro PL, Heshiki RE, Takemoto LE. Fratura de ossos nasais: uma análise epidemiológica. Arq Int Otorrinolaringol. 2008;12(4):498-501.
10. Ashoor AJ, Alkhars FA. Nasal bone fracture. Saudi Med J. 2000;21(5):471-4.
11. Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(1):28-34.
12. Gomes PP, Passeri LA, Barbosa JR. A 5-year retrospective study of zygomatico-orbital complex and zygomatic arch fractures in Sao Paulo State, Brazil. J Oral Maxillofac Surg. 2006;64(1):63-7.
13. Motta MM. Análise epidemiológica das fraturas faciais em um hospital secundário. Rev Bras Cir Plást. 2009;24(2):162-9.
14. Calderoni DR, Guidi MC, Kharmandayan P, Nunes PH. Seven-year institutional experience in the surgical treatment of orbito-zygomatic fractures. J Craniomaxillofac Surg. 2011;39(8):593-9.
15. Atighechi S, Baradaranfar MH, Akbari SA. Reduction of nasal bone fractures: a comparative study of general, local, and topical anesthesia techniques. J Craniofac Surg. 2009;20(2):382-4.
16. Higuera S, Lee EI, Cole P, Hollier LH Jr, Stal S. Nasal trauma and the deviated nose. Plast Reconstr Surg. 2007;120(7 Suppl 2):64S-75S.
17. Dickson MG, Sharpe DT. A prospective study of nasal fractures. J Laringol Otol. 1986;100(5):543-51.
18. Powell O, Doshi D. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 4: Should nasal fractures be manipulated under local anaesthesia? Emerg Med J. 2008;25(8):525-7.
19. Illum P. Long-term results after treatment of nasal fractures. J Laryngol Otol. 1986;100(3):273-7.
20. Carr RM, Mathog RH. Early and delayed repair of orbitozygomatic complex fractures. J Oral Maxillofac Surg. 1997;55(3):253-8.
1. Resident Physician of General Surgery of the Clinical Hospital of Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil.
2. Plastic surgeon, resident physician of the Plastic Surgery Area of the Clinical Hospital of Unicamp, Campinas, SP, Brazil.
3. Titular professor of Oral and Maxillofacial Surgery of the Plastic Surgery Area of Faculdade de Ciências Médicas da Unicamp, Campinas, SP, Brazil.
Correspondence to:
Luis Augusto Passeri
Cidade Universitária Zeferino Vaz
Campinas, SP, Brazil - CEP 13083-887
E-mail: passeri@fcm.unicamp.br
Paper submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Paper received: October 26, 2011
Paper accepted: December 8, 2011
Study conducted at the Clinical Hospital of the Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil.
 All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license


