INTRODUCTION
Rhinoplasty remains one of the most common aesthetic procedures1. More recently, technological advances in
injectable products based on hyaluronic acid (HA) and refinements of application
techniques have allowed HA to reach the gold standard as a volumizing agent2. Nasal reshaping with HA is a fast and
simple procedure that does not involve distancing recovery activities while
providing results comparable to conventional rhinoplasty3. The most common applications have been the correction of
deformities of the tip, back, and columella4.
Indications for nasal filling include patients who want to “test” the result of
rhinoplasty, patients undergoing rhinoplasty who do not wish to further surgery
to review a residual deformity, patients who are not candidates for surgery, and
patients waiting for the appropriate time interval before undergoing a secondary
rhinoplasty5,6. The nose is the subunit of the face most
at risk for fillings after glabella. As the number of patients submitted to
fillings increases, so does the number of associated adverse effects.
OBJECTIVES
According to the authors ‘ experience, this study aims to demonstrate a safe
technique, highlighting the anatomical knowledge and problems involved in nasal
reshaping in a standard case report.
METHODS
The main techniques used for Nasal reshaping are bolus and retroinjection. For
safety, we strongly suggest that this procedure be preferably performed with
cannulas. We do not use needles to inject into the nose. Injections should be
performed deep in the musculoaponeurotic layers and suprapericondral and
supraperiostal layers to avoid injury or cannulation of the vessels (which are
subdermal in this region) providing natural results and with greater safety.
In secondary rhinoplasty, extreme caution should be taken. Unpredictable blood
vessel repositioning and a more tenuous blood supply in the operated nose may
increase the risk of ischemia, necrosis, and vascular embolism after filler
injection. Anatomical planes may have been violated or healed. The dermis may be
adhered to deep planes; besides, natural anastomoses between contralateral
vessels may no longer be present.
The amount of HA injected per patient is variable. On average, the total
quantities range from 0.6 to 2ml. The desired modifications are elevation of the
nasal tip, increased nasolabial angle, and correction of nasal dorsum
irregularity with nasal root repositioning. These modifications will be
described below:
- The first step is to photograph the patient. Frontal, lateral, and
caudocranial incidences are essential. Images should be standardized
to help evaluate results;
- The nose is one of the areas most colonized by bacteria. Extra care
in the antisepsis is mandatory for the safety of this procedure;
- Intraoral access is used to block the infraorbital nerve with 2%
lidocaine without epinephrine. This time, tiny additional anesthetic
buds using lidocaine with epinephrine are injected into the nasal
tip and nasolabial angle. Anesthetics with epinephrine help reduce
the risk of peri-cannula bleeding. Remember that there will be a
halo of pallor due to the vasoconstrictor;
- The cannulas should be long enough to reach from the tip to the
nasal root. In general, 50mm in length is a good measure. Our
preference is for the 22G 50mm cannulas;
- In a single step, with the entry point at the nasolabial angle (the
paramedian intake is better than the median, so the syringe does not
touch the chin), we start increasing the columella-labial angle. The
cannula is advanced along the subcutaneous plane to the nasal spine.
Then, the HA is injected slowly, carefully observing the filling of
the columella-labial angle (Figure 1 - step 1);
Figure 1 - Sequential order of the fill. Edited figure: (Warren
RJ, Neligan P. Plastic surgery: aesthetics. 3rd ed.
Amsterdam: Elsevier; 2015. v. 2.).
Figure 1 - Sequential order of the fill. Edited figure: (Warren
RJ, Neligan P. Plastic surgery: aesthetics. 3rd ed.
Amsterdam: Elsevier; 2015. v. 2.).
Once the nasolabial angle is corrected, the cannula is previously oriented to
strengthen and rectify the columella. This maneuver straightens, lengthens, and
supports the columella. This should produce a more anterior tip projection with
less cranial rotation. When stretching the columella, the nose should appear
more isosceles and the nostril more tear-shaped when viewed from the basal angle
(Figure 1 - step 2);
• In a single step, with the entry point still at the
nasolabial angle, the third stage begins with the tip’s projection.
A single bolus is sufficient for this purpose
(Figure 1 - step3(;
• The last step is to correct the back. Injections before and
after the comic can disguise it. Subsequent injection projects the
root. The final point is to create a new root at the approximate
level of the supratarsal fold, to create an angulation of
approximately 135 degrees of the nasal dorsum with the forehead, and
to create a new nasal profile, more aesthetically pleasing (Figure 1 - steps 4 and 5);
- Cohesive gels can be easily molded and remodeled to sculpt the
nose, such as “modeling mass” immediately after injection.
Additional syringes may be required at this stage;
- In all areas, always apply deep injections;
- In our technique, we start with the columella enhancement, then the
tip, and finish with the back;
- The right hand is used for smooth, measurable, and directional fill
injection. The left hand is used to guide placement, shaping, and
avoid inadvertent spreading of the injected load. This is
particularly important when injecting the dorsum since the lack of
accuracy of the injected filler creates a noticeable asymmetry;
- Slow and constant correction provides the safest way to achieve the
best results;
- Compression of the nasal and dorsal upper part of the angular
arteries is also recommended. It should always be injected more than
2 to 3 mm above the alar groove to avoid the lateral nasal
artery7;
- Stop injection immediately if there are ischemic changes in the
skin of the nose;
- Other additional fixes are always possible at a later date;
- Avoid large volumes of superficial injections as this can cause
external vascular compression, which can cause ischemia and necrosis
of the skin. This is especially important at the tip and nasal
base;
- Closely monitor the nose after the procedure for signs of ischemia,
particularly in those patients with a history of the previous
rhinoplasty, as their vascular supply may be distorted and
compromised;
- Avoid unnecessary external compression of the nose after injection,
such as wearing glasses, for at least a few days;
- A small dressing is added at the entry points at the end of the
procedure to avoid ha reflux and the consequent increased risk of
fistulization.
RESULTS
One of the authors developed this technique (Fernandes RL) in 2013, and since
then, it has been performed in approximately 60 patients. Results range from
good to very good in almost all patients. The duration of the effect of
correction of the dorsal gibbon is significant, with an average between 12 and
18 months. The duration of the tip lift is shorter, usually half that time. Pain
is considered mild to moderate using this technique. The most common side
effects are fistula (or HA vesicle) at the cannula’s entry points and persistent
erythema of the nose. No serious adverse events were observed using this
technique.
MCB, 28 years old, 1.2 ml HA (Teosyal Ultra Deep® - Teoxane Laboratory -
Genéve) with 22G cannula - 50mm (Figures 2,3 and 4).
Figure 2 - Results of the nasal reshaping procedure. A,
C and E pre-application.
B, D and F
post-application.
Figure 2 - Results of the nasal reshaping procedure. A,
C and E pre-application.
B, D and F
post-application.
Figure 3 - Pre-application HA. HA: Hyaluronic Acid.
Figure 3 - Pre-application HA. HA: Hyaluronic Acid.
Figure 4 - 3 weeks after the procedure.
Figure 4 - 3 weeks after the procedure.
DISCUSSION
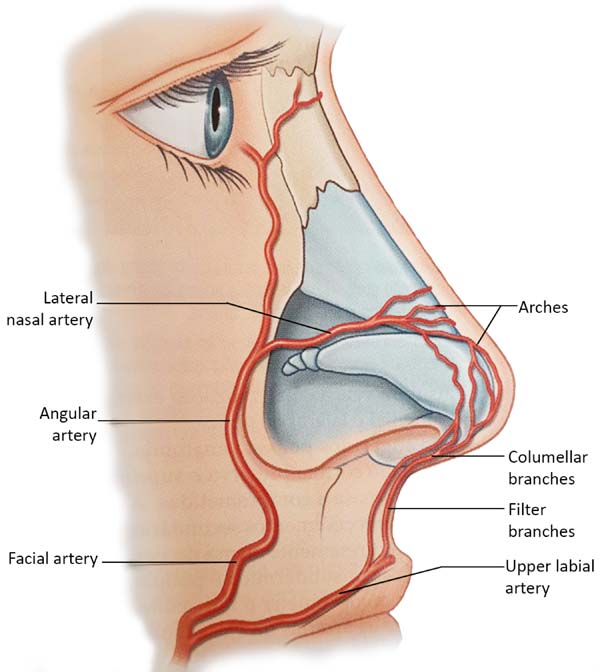
Anatomy
The extensive collateral blood supply of the nose makes this procedure
relatively safe. Both a branch of the internal carotid artery, the
supratroclear, and a branch of the external carotid artery, the facial
artery, give rise to branches that cross the midline. These form a vascular
network that runs through the back. Along the way, inferior to the nose, the
facial artery originates the upper labial artery, which also originates the
filter’s arteries, providing the ascending columellar arteries’ main
contribution. Several arches arise from both the supratroclear arteries and
the facial arteries (Figure 5); the
lateral nasal artery is one of the main sources of blood supply to the
nose.
Figure 5 - Arterial irrigation of the nose (Warren RJ, Neligan P.
Plastic surgery: aesthetics. 3rd ed. Amsterdam: Elsevier; 2015.
v. 2.).
Figure 5 - Arterial irrigation of the nose (Warren RJ, Neligan P.
Plastic surgery: aesthetics. 3rd ed. Amsterdam: Elsevier; 2015.
v. 2.).
Tansatit et al., in 20168, studied 50
cadaver noses and showed that the dorsal artery of the nose is not a
constant artery. It is present as a pair of arteries in 34%. The typical
pattern of the nose’s dorsal artery is a large and long artery that descends
through the back or side of the nose and is anastomosed with the lateral
nasal artery on one side or both. The lateral nasal artery (LNA) is a
constant branch of the alar groove’s facial artery. It represents an
anastomosis between the facial artery (FA) and ophthalmic artery (OA) in the
paracentral zone of the middle third of the face. In 28% of the cadavers, a
single and sizeable dorsal artery was presented8. The study used 57 adult hemifaces to allow precise
observation of the branches of the facial artery. Four patterns were
identified based on the detailed course and origin of the angular artery
(AA) concerning the surrounding structures. In type I, the persistent
pattern in which the AA traverses the LNA branch point toward the medial
corner area. In type II, the deviation pattern, the AA originates from FA
near the corner of the mouth and then heads towards the infraorbital area,
finally rotating medially along with the nasal areas nasojugal corner. This
pattern was the predominant type, and AA emerged along with the lower margin
of the eye’s orbicularis. In type III (alternative pattern), AA originates
from OA and runs down along the nose’s side. Finally, in type IV (latent
pattern), AF ends up as ALN without producing an AA branch. In summary, AA
originated from FA in 50.9% of the specimens dissected with persistent (type
I) and deviation (type II) patterns 8.
Venous drainage of the nose consists mainly of vessels anastomosed with the
facial vein, either through veins that travel from the back and lateral
nasal wall or through vessels that accompany the filter and upper labial
vessels8. The vascularization of
the nose is superficially located below the dermis.
Fillers
Fillers are volumizing biomaterials that are injected into dermal and/or
subcutaneous tissues for various reconstructive and cosmetic purposes,
especially on the face9. The use of
injectable fillers has skyrocketed in the last 25 years. The American
Society of Plastic Surgeons reports an increase from 650,000 filling
procedures in 2000 to 2.3 million in 20144. Hyaluronic acid (HA) injections comprise most of these
procedures (80%), followed by calcium hydroxyapatite (CaHA) (10%),
polylactic acid (5%), and autologous fat (3%)9.
From the 1990s to today, HA fillers have evolved technologically. They have
improved durability, versatility (gels with distinct rheological
characteristics and different tissue expansion capabilities), and safety.
These changes allowed HA to become a good volumizing agent10.
There is no identical or similar HA filler if we compare different brands.
The rheological characteristics of each product are unique. They differ
among the most diverse products, mainly depending on the following features:
being single-phase or biphasic, the molecular weight of its HA chains, the
technology and its degree of crosslinking, and the concentration of HA.
The main rheological parameters are viscosity, cohesiveness, and elasticity.
Viscosity is the spreading capacity of the gel. The more viscous, the
smaller the tissue spread. Surface applications require less viscous gels to
make results more natural without irregularities.
Cohesiveness is the resistance capacity of the gel to shear. The more
cohesive, the more united its structure remains when subjected to external
pressure. We give preference to the more cohesive HAs when we want to get
better-defined forms.
Elasticity is the ability to resist deformation when subjected to external
pressure. Deep planes are looser and require more elastic HAs for better
tissue expansion.
Of course, there is no ideal filler, but we recommend high viscosity,
cohesive, and elasticity HA if we want to perform a non-surgical rhinoplasty
effectively and safely. They are known as volumizers and are indicated for
subdermal application.
Adverse effects
The potential adverse events associated with filling are injection site
reaction, inappropriate injection (hypercorrection, nodulation, asymmetry),
product sensitivity, infection, and necrosis.
Although most complications are transient, some irreversible ones can cause
severe functional and aesthetic deficits1. Complications, fortunately, are not typical and range from
hematomas, edemas, and late granulomatous reactions to more severe skin
necrosis11,12. Necrosis of the nose’s tip’s skin
is particularly worrisome in the procedure, as it inevitably leads to
permanent disfigurement. However, the nasal dorsum correction without
considering the tip’s correction does not produce a comprehensive aesthetic
improvement.
Inadvertent injection of intravascular filler would lead to irreversible
necrosis of the skin. If an artery compression causes ischemia, it can
eventually be reversed by dissolving the filling of AH13,14. Due to this reason, in case of use of needles, we recommend the
filling injection only after the aspiration test, and we recommend that you
observe closely immediately after rhinoplasty with HA and be ready to inject
hyaluronidase.
Intermittent swelling followed by the development of palpable and/or painful
nodular papulocystic lesions, from weeks to months after the injection, can
progress to aseptic abscesses, the most common evolution being drainage
through a fistula. These reactions usually occur after patients have their
second or third injection. The histopathological analysis may show
non-granulomatous inflammatory infiltrate (chronic suppurative inflammatory
process with eosinophilia) or granulomatous reactions.
The mechanisms underlying the activation of the immune system and leading to
chronic granuloma formation are still unclear. Various agents, including
biomaterials, can trigger granulomatous reactions. These late reactions
related to HA fillers are immunological in nature, but an infectious origin
cannot be ruled out. It is important to differentiate two possible bacterial
presence sources: 1 - bacteria are directly inoculated in the filling
material or reach the filler from distant locations; 2 - systemic or remote
infection can provoke inflammatory immunomediator reactions harmful to
fillers in the absence of bacterial colonies in the filler. Clinically, a
nodule of consistency and late-onset may suggest a granulomatous response.
However, granuloma is a pathological diagnosis. True granuloma appears late
(especially after 6 to 24 months) at all injected sites at approximately the
same time; they grow quite fast.
The initial adverse effects described above tend to disappear within one or
two weeks spontaneously with symptomatic treatment. In cases of severe or
persistent swelling requiring corticosteroid use, betamethasone
(0.05mg/kg/day) is preferable due to its higher mineralocorticoid action
(antiedema) compared to the others.
Persistent hypercorrection can be treated early by incision and drainage. A
blade is inserted directed to the nodule, and an expression is
performed.
Hypersensitivity reactions usually regress without sequelae with the triple
therapeutic regimen: hyaluronidase injection (once a week while the reaction
persists) + antibiotics (macrolides such as clarithromycin or lymphomycins
such as clindamycin) for 14 to 21 days + oral prednisolone (0.5mg/kg/day,
while the reaction persists).
Due to frequent recurrence, corticosteroid treatment can last a long time.
All precautions related to corticosteroid side effects should be taken:
chest X-ray, bone densitometry, serum lipid dosage, blood pressure, and
blood glucose monitoring should be considered. For treatment for more than
three months, ophthalmological evaluation and supplementation of calcium
carbonate (1.5g per day) and sodium alendronate (70mg per week) is
recommended.
True granuloma usually reacts well to intralesional steroid injections
(triamcinolone acetonide), despite or associated with oral corticosteroid
ingestion.
The concomitance of HA reactions and other infectious conditions nearby is
quite common. Investigation of periodontal disease and chronic sinusitis
should be encouraged, especially in suggestive signs and symptoms.
The possibility of intravascular injection blindness is described in the
literature, but cases with HA showed better results than other fillers due
to hyaluronidase use, according to a meta-analysis study15. Another meta-analysis analyzed the
cases described and found that most were unilateral cases with acute visual
symptoms and signs, with a better prognosis in patients with partial loss of
vision and cases of anterior artery branch obstruction, with a worse
prognosis of complete blindness and obstructions in the central retinal
artery or ophthalmic artery16. In
arterial embolization cases, the immediate application of hyaluronidase and
the emergency evaluation of a specialist in angiology and vascular surgery
(possibly also an ophthalmologist qualified for retrobulbar injection) is
the best way to minimize sequelae.
CONCLUSION
We are in the midst of a new era of rhinoplasty, in which surgery is not the only
means to treat heart defects17.
Non-surgical options seem more feasible than they would be before the advent of
the new synthetic fillers18. In the
literature, however, there are few prospective studies focused on the efficacy,
safety, and longevity of HA fillers to support their usefulness as a
non-surgical alternative to rhinoplasty. Several rhinoplasty surgeons have used
fillers in the nose for many years, recognizing that HA can accurately smooth
irregularities and asymmetries in the nose after aesthetic rhinoplasty. Indeed,
the ability to smooth irregularities and asymmetries in the nose with an
injectable material still has great appeal because imperfections after
rhinoplasty are common.
The main advantage of using fillers in the nose is correcting a deformity without
the financial cost, anesthetic risk, or downtime usually associated with
surgical intervention. Disadvantages include potential damage to the nasal skin
envelope, the need for serial treatments to maintain correction, and a decrease
in the surgeon’s impulse to achieve the perfect intraoperative outcome5. Fear of occlusion or vascular compression
is undoubtedly the most threatening. However, we believe that by following the
simple steps of safety and having refined anatomical knowledge, fillers can be a
good tool for a safe and comprehensive improvement of modeling rhinoplasty.
REFERENCES
1. Robati RM, Moeineddin F, Almasi-Nasrabadi M. The risk of skin
necrosis following hyaluronic acid filler injection in patients with a history
of cosmetic rhinoplasty. Aesthet Surg J. 2018 Jan;38(8):883-8.
2. Fernandes RL. Hyaluronic acid filler for the malar area. In: Issa
MCA, Tamura B, eds. Botulinum toxins, fillers and related substances. Cham:
Springer International Publishing; 2019. p. 271-80.
3. Youn SH, Seo KK. Filler rhinoplasty evaluated by anthropometric
analysis. Am Soc Dermatol Surg. 2016 Ago;42(9):1071-81.
4. Thomas WW, Bucky L, Friedman O. Injectables in the nose. Facial
Plast Surg Clin North Am. 2016 Ago;24(3):379-89.
5. Humphrey CD, Arkins JP, Dayan SH. Soft tissue fillers in the nose.
Aesthet Surg J. 2009;29(6):477-84.
6. Kurkjian TJ, Ahmad J, Rohrich RD. Soft-tissue fillers in
rhinoplasty. Plast Reconstr Surg. 2014 Fev;133(2):121-6.
7. Scheuer JF, Sieber DA, Pezeshk RA, Gassman AA, Campbell CF, Rohrich
RJ. Facial danger zones: techniques to maximize safety during soft-tissue filler
injections. Plast Reconstr Surg. 2017 Mai;139(5):1103-8.
8. Tansatit T, Apinuntrum P, Phetudom T. Facing the worst risk:
confronting the dorsal nasal artery, implication for non-surgical procedures of
nasal augmentation. Aesthetic Plast Surg. 2017 Fev;41(1):191-8.
9. Wang LL, Friedman O. Update on injectables in the nose. Curr Opin
Otolaryngol Head Neck Surg. 2017 Ago;25(4):307-13.
10. Williams LCBA, Kidwai S, Mehta K, Kamel G, Tepper O, Rosenberg J.
Nonsurgical rhinoplasty: a systematic review of technique, outcomes, and
complications. Plast Reconstr Surg. 2020 Jul;146(1):41-51. DOI:
https://doi.org/10.1097/PRS.0000000000006892
11. Johnson ON, Kontis TC. Nonsurgical rhinoplasty. Facial Plast Surg.
2016;32(5):500-6. DOI: https://doi.org/10.1055/s-0036-1586209
12. Alam M, Dover JS. Management of complications and sequelae with
temporary injectable fillers. Plast Reconstr Surg. 2007 Nov;120(6 Suppl
1):98S-105S.
13. Daher JC, Silva SV, Campos AC, Dias RCS, Damasio AA, Costa RSC.
Complicações vasculares dos preenchimentos faciais com ácido hialurônico:
confecção de protocolo de prevenção e tratamento. Rev Bras Cir Plást.
2020;35(1):2-7.
14. Moon HJ. Use of fillers in rhinoplasty. Clin Plast Surg. 2016
Jan;43(1):307-17.
15. Chatrath V, Banerjee PS, Goodman GJ, Rahman E. Soft-tissue
filler-associated blindness: a systematic review of case reports and case
series. Plast Reconstr Surg Glob Open. 2019 Abr;7(4):e2173.
16. Kapoor KM, Kapoor P, Heydenrych I, Bertossi D. Vision loss
associated with hyaluronic acid fillers: a systematic review of literature.
Aesthetic Plast Surg. 2020 Dez;44(3):929-44. DOI:
https://doi.org/10.1007/s00266-019-01562-8
17. Ramos RM, Bolivar HE, Piccinini PS, Sucupira E. Rinomodelação ou
rinoplastia não-cirúrgica: uma abordagem segura e reprodutível. Rev Bras Cir
Plást. 2019;34(4):576-81.
18. Jasin ME. Nonsurgical rhinoplasty using dermal fillers. Facial Plast
Surg Clin North Am. 2013 Mai;21(2):241-52.
1. Institute of Plastic Surgery Santa Cruz,
São Paulo, SP, Brazil.
Corresponding author: André Campoli Frisina, Rua Bento de
Andrade, 216, Jardim Paulista, São Paulo, SP, Brazil. Zip Code: 04503-000.
E-mail: andrefrisina@yahoo.com.br
Article received: April 18, 2020.
Article accepted: April 18, 2020.
Conflicts of interest: none