INTRODUCTION
Loss of substance in the lower third of the leg, especially Achilles tendon
ruptures, which are common after orthopedic surgeries and are challenging for
plastic surgeons because of the high rate of complications and occurrences,1-3 usually requires complex surgical procedures for tissue
reconstruction2-4.
Several options are available for treating these injuries, and the simplest
method is always preferred1,5. The chosen
reconstruction strategy should consider the following factors: injury (location,
size), donor area, patient (clinical history), and surgery (surgeon’s
experience, hospital structure)1.
Among the options available for surgical repair, the use of the reverse sural
flap of the fasciosubcutaneous pedicle3,6,7 or adipofascial
reverse flap has been reported in the literature as a viable option since more
than 20 years7,8; however, this approach has been little
studied compared with other techniques. The main advantages of using the
proposed technique are the simple and fast execution; sufficient and reliable
vascularization; and low morbidity of the donor site, which has an excellent
rotation arc9, making this strategy useful
in several cases.
The objectives of this study were to present the results of surgical treatment of
a complex injury, involving exposure of the Achilles tendon, in the lower third
of the leg using the reverse sural flap of the fasciosubcutaneous pedicle
concomitantly with total skin grafting and to discuss the advantages of the
procedure as well as other surgical alternatives.
CASE REPORT
A.D., a 28-year-old male Caucasian patient without comorbidities, presented with
a necrotic injury (6.0 × 4.0 cm2) with Achilles tendon exposure in
the lower third of his right leg after surgical repair of Achilles tendon
rupture that had occurred during an automobile accident. On day 30 after
surgery, the patient was referred to our plastic surgery service and underwent
surgical debridement (Figure 1).
Figure 1 - Preoperative result. A: Result before debridement;
B: Result after 15 days of debridement.
Figure 1 - Preoperative result. A: Result before debridement;
B: Result after 15 days of debridement.
The complex injury was treated 15 days after debridement. With the patient in the
prone position and under spinal anesthesia, the operative site in the calf
region of the right lower limb was demarcated. The necrotic injury in the lower
third of the leg was repaired using the reverse sural flap of the
fasciosubcutaneous pedicle, which was fixed without tension, concomitantly with
total skin grafting. The skin graft was removed from the ipsilateral popliteal
region during flap preparation (Figures 2
and 3).
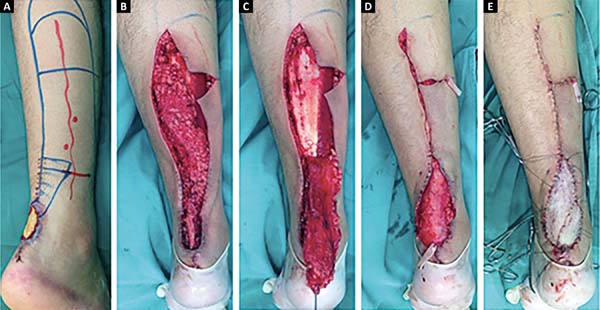
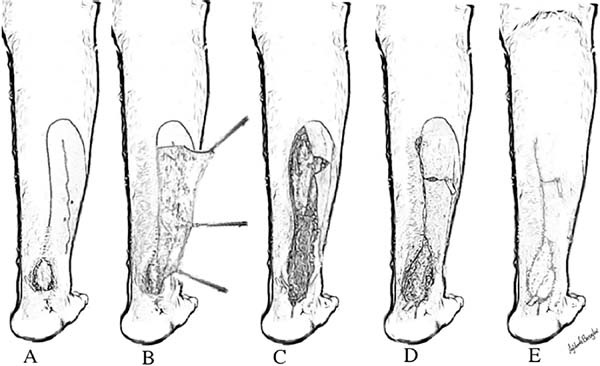
Figure 2 - Intraoperative preparation of the reverse sural flap using the
fasciosubcutaneous pedicle. A: Demarcation of the
operative site; B: Extensive cutaneous detachment;
C: Dissection of the fascia of the sural muscle and
rotation of the flap 180 degrees on the axis of the
fasciosubcutaneous pedicle, covering the exposed area;
D: Fixation of the flap in the recipient area and
use of a Penrose drain to collect the drainage; E:
Immediate postoperative result after performing total skin grafting
at the same time.
Figure 2 - Intraoperative preparation of the reverse sural flap using the
fasciosubcutaneous pedicle. A: Demarcation of the
operative site; B: Extensive cutaneous detachment;
C: Dissection of the fascia of the sural muscle and
rotation of the flap 180 degrees on the axis of the
fasciosubcutaneous pedicle, covering the exposed area;
D: Fixation of the flap in the recipient area and
use of a Penrose drain to collect the drainage; E:
Immediate postoperative result after performing total skin grafting
at the same time.
Figure 3 - Intraoperative preparation of the reverse sural flap using the
fasciosubcutaneous pedicle. A: Demarcation of the
operative site; B: Extensive cutaneous detachment;
C: Dissection of the fascia of the sural muscle and
rotation of the flap 180 degrees on the axis of the
fasciosubcutaneous pedicle, covering the exposed area;
D: Fixation of the flap in the recipient area and
use of a Penrose drain to collect the drainage; E:
Immediate postoperative result after performing total skin grafting
at the same time.
Figure 3 - Intraoperative preparation of the reverse sural flap using the
fasciosubcutaneous pedicle. A: Demarcation of the
operative site; B: Extensive cutaneous detachment;
C: Dissection of the fascia of the sural muscle and
rotation of the flap 180 degrees on the axis of the
fasciosubcutaneous pedicle, covering the exposed area;
D: Fixation of the flap in the recipient area and
use of a Penrose drain to collect the drainage; E:
Immediate postoperative result after performing total skin grafting
at the same time.
The surgical procedure lasted 90 min and was uneventful. The patient was
discharged eight hours after the procedure, without plaster immobilization and
required only occlusive dressings. The patient had no relevant motor and sensory
deficits or pain and was instructed to avoid walking with a full load for one
week. The postoperative period was uneventful, and only occlusive dressings were
required. The lesion gradually healed (Figure 4).
Figure 4 - Postoperative result. A: 60 days; B:
120 days; C: 150 days; D: 180 days
postoperatively.
Figure 4 - Postoperative result. A: 60 days; B:
120 days; C: 150 days; D: 180 days
postoperatively.
DISCUSSION
The need for more effective, easier, and reliable surgical procedures, especially
for treating injuries in the distal third of the leg, has been reported by
several studies over the years1,7.
Considering the increase in patients’ demands for better surgical outcomes,
assessment of the quality of the achieved result has been gaining prominence in
the literature and has stimulated more discussions among plastic surgeons and
patients2-4.
The reverse sural flap of the fasciosubcutaneous pedicle and the reverse
adipofascial flap receive blood supply from the cutaneous perforating branches
of the fibular and posterior tibial arteries1. These flaps preserve the sensory innervation of the saphenous,
superficial fibular, and sural nerves because only a thin region of the
subcutaneous tissue is left under the dermis to avoid injury to the subdermal
plexus of the donor region, whereas most of the subcutaneous tissue that is
easily dissected in a surgical plane guarantees the viability of the flap,
facilitating easy rotation on its axis without the need to release the pedicle
to repair the margins in a second surgical procedure, as is the case with the
fasciocutaneous flap2, maintaining low
morbidity and satisfactory results without functional sequelae1,6,8.
The reverse sural flap of the neurocutaneous pedicle, initially described by
Masquelet et al. (1994), is one of the most common options2 for treating injuries such as those reported in this case.
However, this surgical approach is criticized because of the loss of cutaneous
sensitivity and unsightly scarring of the donor area2.
Perforating flaps have also been gaining prominence in recent years. This
technique was first described by Donski & Fogdestam (1983)5 but has disadvantages, including the
considerable variability in the diameter and position of the perforating
vessels.
The use of microsurgical reconstructions, such as the free myocutaneous flap of
the latissimus dorsi, among other options that have emerged in the past few
years as surgical alternatives for treating injuries in critical areas,2,3 is usually reserved for larger injuries and requires good hospital
infrastructure and highly trained staff.
Some options commonly used for treating complex injuries of the lower limbs have
been described in a literature review published in the Brazilian Journal of
Plastic Surgery in January 201710.
However, the flap used in the present study was not mentioned in that
review.
Considering data from previous studies and this study, the use of the reverse
sural flap of the fasciosubcutaneous pedicle or reverse adipofascial flap has a
good prognosis. The use of these flaps was effective and safe, had excellent
esthetic and functional results, and did not cause relapses during the
evaluation period. Therefore, these flaps deserve more attention from plastic
surgeons because of their high clinical potential, especially compared with
other techniques used routinely.
CONCLUSION
The use of the reverse sural flap of the fasciosubcutaneous pedicle concomitantly
with total skin grafting was found to be a good option with a satisfactory
result for the surgical treatment of a complex injury due to Achilles tendon
rupture in the lower third of the leg.
COLLABORATIONS
|
DNS
|
Analysis and/or interpretation of data; statistical analyses; final
approval of the manuscript; conception and design of the study;
completion of surgeries and/or experiments; writing the manuscript
or critical review of its contents.
|
|
MR
|
Final approval of the manuscript; conception and design of the study;
completion of surgeries and/or experiments.
|
|
AABMR
|
Analysis and/or interpretation of data; statistical analyses; final
approval of the manuscript; conception and design of the study;
writing the manuscript or critical review of its contents.
|
|
ICP
|
Analysis and/or interpretation of data; statistical analyses;
conception and design of the study; writing the manuscript or
critical review of its contents.
|
REFERENCES
1. Braga-Silva J, Martins PDE, Román JA, Gehlen D. Utilização do
Retalho Adipofascial Reverso nas Perdas de Substância Cutânea do Terço Distal da
Perna e Pé. Rev Bras Cir Plást. 2005;20(3):182-6.
2. Garcia AMC. Retalho sural reverso para reconstrução distal da perna,
tornozelo, calcanhar e do pé. Rev Bras Cir Plást.
2009;24(1):96-103.
3. Weber ES, Franciosi LFN, Mueller SF, Dalponte M, Heurich NR,
Gonçalves SCS. Retalho sural para reconstrução do pé. ACM Arq Catarin Med.
2007;36(Supl. 1):1-4.
4. Belém LFMM, Lima JCSA, Ferreira FPM, Ferreira EM, Penna FV, Alves
MB. Retalho sural de fluxo reverso em ilha. Rev Soc Bras Cir Plást.
2007;22(4):195-201.
5. Donski PK, Fogdestam I. Distally based fasciocutaneous flap from the
sural region. A preliminary report. Scand J Plast Reconstr Surg.
1983;17(3):191-6. PMID: 6673085
6. Vendramin FS. Retalho sural de fluxo reverso: 10 anos de experiência
clínica e modificações. Rev Bras Cir Plást. 2012;27(2):309-15. DOI: http://dx.doi.org/10.1590/S1983-51752012000200023
7. Gumener R, Zbrodowski A, Montandon D. The reversed
fasciosubcutaneous flap in the leg. Plast Reconstr Surg. 1991;88(6):1034-41.
DOI: http://dx.doi.org/10.1097/00006534-199112000-00013
8. Franco T, Couto P, Gonçalves LFF, Franco D, Silva CC. Tratamento das
exposições ósseas e tendinosas no terço distal da perna e no pé utilizando
retalho fasciossubcutâneo reverso de panturrilha. Rev Bras Ortop.
1996;31(3):247-52.
9. Kneser U, Bach AD, Polykandriotis E, Kopp J, Horch RE. Delayed
reverse sural flap for staged reconstruction of the foot and lower leg. Plast
Reconstr Surg. 2005;116(7):1910-7. DOI: http://dx.doi.org/10.1097/01.prs.0000189204.71906.c2
10. Anlicoara R, Barbosa FAMA, Sá JZ, Braga ACCR, Sá GT. Reconstrução de
feridas complexas de membros inferiores com retalhos fasciocutâneos reversos.
Rev Bras Cir Plást. 2017;32(1):116-22.
1. Universidade Federal de Mato Grosso do Sul,
Campo Grande, MS, Brazil.
2. Sociedade Brasileira de Cirurgia Plástica, São
Paulo, SP, Brazil.
Corresponding author: Daniel Nunes e
Silva, Av. Alto Porã, nº 51 - Chácara Cachoeira, Campo Grande, MS,
Brazil. Zip Code 79040-045. E-mail:
dermatoeplastica@gmail.com
Article received: February 4, 2018.
Article accepted: June 22, 2018.
Conflicts of interest: none.