ABSTRACT
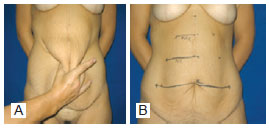
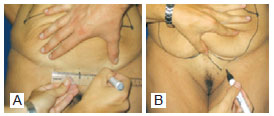
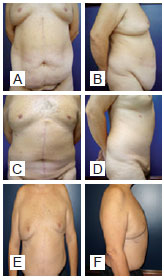
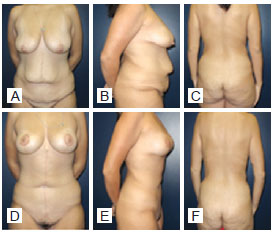
BACKGROUND: Morbid obesity is a worldwide endemic disease. Its growing incidence makes it a public health problem. Bariatric surgery is an alternative weight loss method with the objective of controlling obesity-associated diseases and improving quality of life. The surgical treatment of the deformities resulting from significant weight loss is a new challenge for plastic surgeons. This paper presents a new technique for abdominoplasty in formerly obese patients with a midline abdominal scar resulting from gastroplasty.
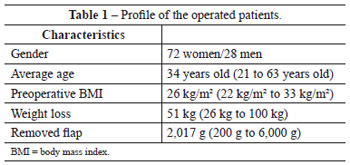
METHODS: A total of 28 men and 72 women who underwent abdominoplasty after gastroplasty by the "fish" technique described in this study were analyzed.
RESULTS: The results obtained with the technique presented were satisfactory, resulting in a new body contour and a low complication rate.
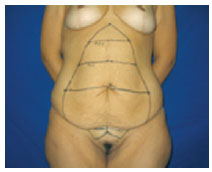
CONCLUSIONS: Abdominoplasty with markings forming a fish shape is successful for the removal of excess abdominal skin in patients who underwent bariatric surgery.
Keywords: Surgery, plastic/methods. Abdomen/surgery. Gastroplasty. Bariatric surgery.