



Articles - Year 1998 - Volume 13 -
Vitamina A Ácida, Vitamina E e Vitamina C Injetáveis no Tratamento de Necroses de Pele
Vitamina A Ácida, Vitamina E e Vitamina C Injetáveis no Tratamento de Necroses de Pele
ABSTRACT
Experimental studies veckoning vitamin A acid (all tmns retinoic acid 0.1 %) with the antioxidant action of vitamin E (tocophero1 acetate 0.2%) and vitamin C (coated ascorbic acid 0.2%) diluted 1:4 to vitamin A 0.02%, vitamin E 0.05% and vitamin C 0.05%, with efficacy in the vascular neoformation induction and in the cellular membrane stabilization, has been clinically used by us for the improvement of the skin and the skin necrosis regression after routine plastic sugeries. Patients after rhytidectomy, breast reduction and abdominoplasty with localized skin flap necrosis were submitted to daily intradermic injections for a period of 15 days, had their skin healed by these vitamin effects.
Keywords:
RESUMO
Este trabalho baseou-se em estudos realizados em laboratórios contando com a capacidade de neoformação vascular induzida pelo ACE pool isto é, vitamina A ácida "all trans retinoic acid 0,1%", com a ação antioxidante das vitaminas E "Acetato de tocoferol 0,2%" e C "ácido ascórbico revestido 0,2%" e com a capacidade das mesmas na estabilização das membranas celulares. As vitaminas foram diluídas 1:4 com vitamina A 0,002%, vitamina E 0,05% e vitamina G 0,05%. O uso de ACE pool na forma injetável intradérmica superficial por 15 dias demonstrou regerssão do quadro de necrose cutânea pós cirurgia plástica (ritidoplastia; mamoplastia redutora e abdominoplastia).
Palavras-chave:
Very often skin necrosis by traumatism and after routine plastic surgeries are reponed in the literature and in scientific meetings. In the same patient, the skin react diversely even after safe surgical manipulation, from region to region, in different or the same decade of their lives by unknown biochemical behavior and stimulation.
Several examples illustrate these occurrences. In the same scar line there are keloids segments alternated with unconspicuos scars. In the rhytidectomy there are scars with aesthetic variations in the same patient, in which hypertrophic reactions, keloids, scar broadness, skin flap necrosis, etc. are present.
The skin texture, undermined extension, local suture tension, smokers, age and even the surgeons qualification are some of the countless factors, used to explain these secondary unpleasant problems, where some are predictable and others unexpected. Isolated or in combined situations, not extended to extensive, deep or superficial skin necrosis are always a problem for the doctors and for the patients, based on the emotional involvements and unaesthetic effects. Laboratory researches proved the capacity of vascular neo-formation induced by vitamin A (a11 trans retinoic acid 0.1 %), with the anti-oxidant action of the vitamin E (tocopherol acetate 0.2%) and vitamin C ( coated ascorbic acid 0.2%) "ACE pool" diluted 1:4 to vitamin A 0.02%, vitamin E 0.05%, vitamin C 0.05%, and their ability of stabilizing the skin necrosis when inrradermically injected.
Based on preliminary studies with ACE pool, we have been using this product for increasing of the collagen and the c1astic fibers of the skin face for aesthetic purposes especial1y 24 hours after rhytidectomy, and in extension in cases of abdominoplasty and breast reduction, up to 15 days post-operarive period, with the scope to obtain better scars aspects and the reduction of eventual mild skin necrosis.
VITAMIN A
It was already described that vitamin A (retinoic acid) has the ability of intra-nucleous activation in the retinoic cycle, resulting in a better cellular function with the incre.1se of collagen and elastic tibers production.
Its anti-oxidant action and immune regulation effets, may be used in difterent pathologies (2,6,11,12,15,17,18,20,21).
Vitamin A relationship to the hyperkeratotic syndrome was first c1inically diagnosed by STTUTGEN(20) in 1962. RW Johnson Pharmaceutical Research Institute, supported Sttutgen's experiments with retin A for ortho diagnosis(15). KLIGMAN(11), in 1969, was the first to clinically associate vitamin A with the problem of acne. He began vitamin A treatment for skin alterations, mainly in the photo aged skin.
Recently ELLIS(5), in 1990, demonstred the positive effect of Tretinoin based cream (all trans retinoic acid 0.1 % = 1000 mm/ml) in the treatment of the photo aged skin. He observed the reduction of the epidermic corneal byer and the increase of granular layer, an advanced number of mitosis in the keratocyres, the presence of glicosaminoglicans, a growth of the anchoring fibers in the intersection of the dermal layers and a higher thickness of the epidermis.
This first evaluation was done 4 months after the treatment and repeated 22 months later.
The final result showed a significant decrease of the thin facial wrinkles, creases, as well as the improvement of the skin texture and the skin e1aticity. No side effects were observed, confirmed by KLIGMAN(12), LASNITZKI(13) and WILSON(22).
According to JADILLIER(9), the retinoic acid is more efficient than retinol because it doesn't need glycolization in order to generate glycosaminoglicans which are responsible for the presence of fibronectines.
The fibronectines are reduced in the photo aged skin and with an uncontrolled growth in the malignant transformations. Based on these effects, vitamin A may possibly inhibit the skin carcinogenesis.
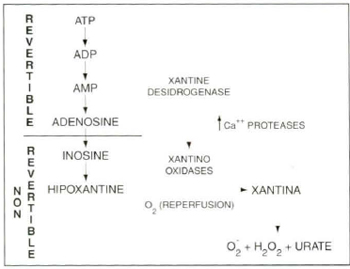
Fig. 1 - Ischemia by re-perfusion.

Fig. 1b - Haber-Weiss reaction.
Immune Regulator Effect of the Vitamin A Acid.
According to PENN er col.(17) supplementary vitamins A, C and E, increase the functions of the immunologic cellular mediator, with significant absolute number increase of lymphocyte T, followed by an increase of Ivmphocyte T4 (Helper), and the stabilization of Ivmphocyte T8 in reply to the phytohemaglutinine, which is a chemical mediator increased with the presence of vitamins A, C and E.
Many articles reports that vitamin A maintain the intra-cellular communication with each other. They also described that the prostaglandines E2 synthesized by the epidermis in the presence of all trans retinoic acid induces blood stimulation increasing the leukocyte response. These reactions improve the skin defensive mechanisme against virus, bacteria, parasites and non malignant or malignant tumoral processes. CONNOR(3).
Retinoic acid also stimulates the production of interleucin. Its presence in the integument actives the network of the Merckel cells and the free extremities neurons placed in the dermic-epidermic junction. These reactions are recognized as important elements in the release of prostaglandines D2, serotonin, leukotriens ( chemical mediators) which stimulate vasodilatation with the subsequent increase of vascular permeability. Based on these, some possible chemical reactions can be described:
a) The platelets when adhered to the sub-endothelium become activated by their contact with trombine and the collagen tissue.
New platelets when connected with these activated platelets also become active, releasing platelet activating factor .
b) The trombine and the collagen have different receptors regarding the platelets. Biochemical reactions among them, determine the appearance of platelets granules secretion.
One of these reactions release prostaglandine IP3 which is the second most important platelet activator. IP3 prostaglandine plays the role of calcium ionophore increasing its concentration, and subsequently activates A2 like phospholipases enzymes, which by reactions release arachidonic acid.
c) Tromboxane A2, a potent vasoconstrictor and platelet aggregator is a subproduct of the arachidonic acid. Therefore it is necessary its inhibition, and stimulation of the cyclo-oxigenase enzyme in order to obtain a small quantity of tromboxanc A3; which is physiologically inactivated and reduces platelets aggregation while maintaining vasodilatation.
d) The production of prostaglandin I2 ( a potent vasodilator and anti-platelet aggregator) in the endothelium is not significant inhibited and the physiologic activity of a new prostaglandin I3 is added to prostaglandin I2. The resulting effect is a homeostatic equilibrium tending to an increased vasodilatation condition, with lower platelet aggregation. ABB(1).
e) Leukotriens are also sub products of arachidonic acid. Leukotriens B4 (L T B4) are present in diseases like rheumatoid arthritis and psoriasis. In the presence of lipoxigenase enzyme, the Arachidonic acid generates leukotriens B5 (L T B 5 ) with reduced effect over inflanmatory and chemiostatic processes, improving the skin local conditions.
The prolonged use of retinoic acid even in non-toxic concentration will inhibit the T-killer lymphocyte.


Fig. 2a . Three of the skin flaps are mobilized in the dorsal aspects of the rats.
Each flap presents 5 cm length and 1 cm in the base. The flaps vertex are placed cranially.

Fig. 2b - The skin flaps after undermined are placed in their normal position. At the vertex "a" Gillis isolated type of stitch with 5-0 mono filament nylon is placed and an isolated stitch in each flap side complete the suture.

Fig. 2c - All the triangular flaps present 16% of necrosis of their distal portion, 24 hours after their mobilization.

Fig. 2d - At the 8th postoperative day, the flap "A" treated with ACE Pool shows significant necrosis regression, while the flap "B" presents a necrotic scar.

Fig. 2c - Microscopic aspect of the flap C (control) 24 hours after its mobilization, showing dermo epidermic necrosis with acute inflammatory reaction, with the presence of capillary network dilation, high neurrophil concentration around the vessels, necrotic phanerous and neotrophils surrounding the hair axis.

Fig. 2f - Microscopic aspects of the non treated flap (B) after 7 postoperatory days, showing the dissociation of the corneal stratus done by ncutrophils and red cells, epidermic necrotic focus, neutrophils exudate below the dermal level derno epidermic necrosis focus of tissue regeneration and inflammatory reactions.

Fig. 2g - Microscopic aspects of the treated flap (A) after 7 days postoperarive, showing a thick corneal stratum with regenerate epidermis, the dermis with presence of cutaneous annex, ectasia of capillary network with few surrounding neutrophils, fibroblast proliferation and histioid cells inside the fibrin network.
VITAMIN C
Vitamin C (ascorbic acid) Is essential for the collagen synthesis, OLZEWER(14). It is required in the hydroxybtion of proline in the collagen, STRYER(19). The ascorbat removes the ferric ion from the enzyme which was inactive during the proline hydroxylation, becoming a specific anti-oxidant. The synthesis of collagen without the ascorbat will produce abnormal fibers and will contribute to the appearence of skin lesions and vascular fragility.
CLINICAL APPROACHES
Patients
Based on the experimental studies in rats and on the literature, 21 patients were treated with ACE pool injections in specific necrotic areas after routine plastic surgeries; 4 underwent rhytidectomy, 10 breast reduction (3 bilateral and 7 unilateral skin localized necrosis) and 7 abdominoplasties. Figs. 3,4 & 5.

Fig. 3a - A 51 year-old white woman after a routine rhytidectomy,shows a retro-auricular skin necrosis behind the ear 24, hours after the surgery.

Fig. 3b Same patient 14 days after daily injection of face pool. complete skin regeneration is observed without evidence of scarring.

Fig. 4a - A 33 year-old woman, after breast reduction through vertical incision procedure, shows vascular dcficiency ar the areola-nipple complex 24 hours after surgery.

Fig. 4b - Same patient 14 days after daily injection of ACE pool. A complete regeneration of the areola-nipple complex is observed, without suture dehiscence or scar deformity.
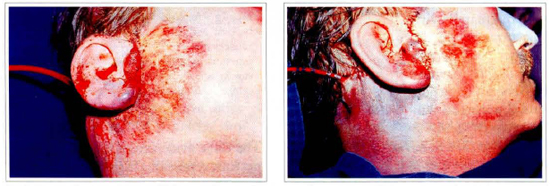
Figs. 5a & 5b - A 50 year-old man 24 hours after rhytidccromy, shows a huge hematoma with skin vascular deficiency.

Fig. 5c - 4 days after daily injection of ACE pool.

Fig. 5d - 15 days after daily injection of ACE pool.
The patient's ages averaged from 17 to 65 years old. Each necrotic area received daily 1 to 3 cc of ACE pool intradermically (diluted), injcted daily for 15 days. The injections were performed with insulin type of needles adapted to 1 to 3 cc disposable syringe. The place of the injections were 5 mm behind the necrotic area at intradermic superficial level and towards the necrotic zone. The amount of infiltration reached the local epidermic saturation and the necrotic extension. The infiltrations were punctiform and 5 mm distant from each other.
DISCUSSION AND CONCLUSIONS
The clinic evidences of the healing processes and the necrotic remissions high level in rats and in the clinic patients allow the following conclusions:
1. The vitamin E in the ACE pool intradermic skin injection seems to be responsible for the cellular membrane stabilization based on the reduction level of phospholipolization in the membrane structures.
2. In combined reactions vitamin A determines the intranucleous activation and stimulates the collagen fibers formation
3. The vitamin C determines thc collagen tissue stabilization induced bv the proli-hidroxilation.
4. The association of these vitamins, also determine the vitamin E potencialization that inhibit the cellular lipidic peroxidation.
5. The tissues treated with ACE pool presented a time reduction in the healing processes when compared to similar healing involvements in a non treated area.
6. Localized necrosis remission were evident in almost all treated cases. The final cicatrization macroscopic aspect were of a high acceptable aesthetic quality compared to scars after secondary intention healings.
7. In conclusion injectable ACE pool is a specific method for limited necrotic areas that determine a high percentage of necrosis remission with a better acceptable scar in a shorter period of time, compared to traditional methods.
REFERENCES
l. ABB J et al: Effect of Retinoic acid on the Spontaneous and Interferon-induced activity of Human NaUiral Killer Cells. Int. J. Cancer. 1982;30:307.
2. CHANDHARY L et al: Metabolism of All Trans (113H) Retinil acetate in young rats test. Ann. Nutr. Metab. 1986;30: 1.
3. CONNOR HJ et al: Inhibition of UVB Carcinogenesis by Retinoic Acid. Cancer Research. 1983-43:272.
4. DIPLOCK AT, RICE-EVANS CA, Burdon RH. Is there a Significant Role for Lipid Perxidation in the Causation of Malignancy and for Antioxidants in Cancer Prevention. Cancer Res. 1994;54: 1952.
5. ELLIS CN, WEISS JS et al. Sustained Improvement with Prolongued Topica1 Tretinoin (Rerinoic Acid) for Photoaged Skin. Journal of the American Acad. Dermat. 1990;23: 1.
6. ESCRIBANO J, GRUBB A, MENDEZ E. Indentification of Retinol as one the Proteic HC Chromophores. Bich. and. Bioph. Research Communications. 1988;155:1424.
7. FITZPATRICK T. Dermatology in General Medicine. MacGrow Hill, Boston. 1993; l:247.
8. HEFFNER JE, REPINE JE. Pulmonary Strategies of Antioxidante Defence. Am. Rev. Respr. Dis. 1989;140:531.
9. JARDILLIER JC, RALLET A. Metabolisme de la Vitamine A et dês Retinoides. Bull. Cancer. 1986;73: 180.
10. KARLSON P. Bioquimica. Guanabara Koogan, Rio de Janeiro. 1970;1:470.
11. KLlGMAN AM, FULTON JE, PLEWIG G. Topical Acid Vitamin A in Acne Vulgaris Arch. Dermatol. 1969;99:469.
12. KLlGMAN. AM et al. Topical Tretinion for Photo Aged Skin. Journal of the American Acad. Dermat. 1986; 15:836.
13. LASNITZKI I. The Effect of Exess Vitamin A on Mitosis in Chick Heart Fibroblast in Vitro. Esp. Cell. Res. 1955;8:121.
14. OLSZEWER E. Radicais Livres em Medicina. Fundo Editorial BYK, São Paulo. 1992;122.
15. ORTHO RW Johnson Pharmaceutical Rcsearch Institute.
16. PALAN PR, GOLDBERG GL et al. Lipid-soluble Antioxidants: Beta-carotene and Alpha Tocopherol Levels in Breast and Ginecologic Cancer Gynecol. Oncol. 1994;55:72.
17. PENN ND. The Effect of Diaret Suplementation With Vitamin A and E on Cell-mediated Immune FUnctionin Elderly Long Stay Patients. A Randomized Controlled Trial. Age and Aging. 1991;20:169.
18. PERSSONELLE J et al. Restauração do Tegumento Cutaneo com uso de All Trans Retinoic Acid Injetável "Nova forma de Tratamento". Rev. Bras. Med., 1993;50:986.
19. STRYER L: Bioquimica Koogan. Rio de Janeiro. 1988;848.
20. STTUTGEN G: Zur Loklbehandiung. von Keratosen Mit Vitamin A. Saur.: Dermat. 1962; 124:65.
21. TONG PS: Trans Retinoic Acid Enhances the Growht Response of Epidermis Keratinocytes to Epidermis Growth factor Beta. J. Invest. Dermatol. 1990;94:126.
22. Wilson EL, Reech E. Plasminogen Activator in Check Fibroblast: Induction of Synthesis by Retinoic Acid: Synergism With Viral Transformation and Pherbol Ester. Cell. 1978;15:385.
ACKNOWLEDGMENTS
- To Tommus Química e Farmacêutica Ltda.
- To Salomão Zoppi - Serviço de Anátomo-Patologia for their keen lab analysis.
- To G. Pozzan - Serviço de Anátomo-Patologia da Santa Casa de São Paulo.
- To Prof. Ricardo Baroudi, MD - for his scientific encouragement.
I - Clinical Director of the Plastic Surgery Ward, Saint Paul's Hospital - Sao Paulo, Brazil.
II - Head of the course of specialization in plastic surgery of University Santa Cecilia dos Bandeiranres, Santos, Brazil.
III - Assistant Physician Plastic Surgery Ward, Saint Paul's Hospital São Paulo, Brazil.
Address for Correspondence:
Jussara G. Perssonelle, MD
Av. Moema 170-111
04077-020 - Sao Paulo - SP - Brazil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket