INTRODUCTION
Pachydermoperiostosis or Touraine-Solente-Golé syndrome is a rare inherited disease,
predominant in males characterized by thickening of the skin (pachydermia), acropachy,
periostosis of long bones, which may be associated with hyperhidrosis and seborrheic
dermatitis1. Facial deformity is one of the main complaints of these patients, and surgical treatment
is the best strategy for its correction. There are several surgical options, among
which are conventional facelift techniques and local skin resections2.
Facelift techniques emerged in the early 20th century3. The first steps in the treatment of facial wrinkles were attributed to Charles Conrad
Miller, due to his publication on the eradication of wrinkles, in which he proposed
the subcutaneous section of the facial muscles4. Dissatisfied with the results of small skin extractions in front of the ear and
on the edge of the scalp, Eugene Von Hollander, in 19015, was the first surgeon to perform a facelift using a long vertical incision in front
of the ear and sideways to the neck3,4.
Later, Lexer at in 19316 suggested that the skin flaps be dissected in a subcutaneous plane. He was the first
surgeon to perform an elevation of the frontal region7.
At the end of World War I, the high demand for repair surgeries was the basis for
facelift. For instance, in 1926, Hunt8 described the coronal incision with resection of the scalp. Five years later, in
1931, Joseph9 reported using a capillary incision for the same purpose10. In 1960, Pagman et al.11 described frontal facelifts by a coronal incision in the hairline or the capillary
insertion10.
From the 70’ onwards, greater emphasis is placed on technical refinements such as
reduced scars, muscle manipulation, and musculoaponeurotic systems4. Skoog reported, in 197412, the elevation of the platysma of the neck and the lower third of the face without
skin detachment4,7. This more profound dissection method, together with the description of the superficial
aponeurotic muscular system (SAMS) by Mitz and Peyronie, in 197613, paved the way for modern facelift techniques3,10.
Pierce et al. em 194714 recognized the relationship between the corrugator muscles and vertical expression
lines in the glabella area and advocated addressing these muscles through a supraciliary
incision4. Castanhares, in 196415, proposed the resection of a cutaneous spindle by incision on the eyebrow to elevate
the lateral portion10.
Many early frontal lifts involved resection of the skin on the forehead or scalp without
weakening the strength of the frontal muscle. Regnault, in 197216, marked the frontal muscle; Skoog, in 197412 and Vinas et al., in 197617, defended the resection of the frontal strips to weaken the muscle10.
As in all scientific activities, the evolutionary process is continuous. Techniques
and tactics continue to emerge, showing the importance of rhytidoplasties for the
scene of plastic surgery4.
The case report, the object of this paper, has its peculiarity in the fact that it
is a patient with syndromic facies, which presents a strong cutaneous manifestation,
especially in the distal third in the frontal region, making it impossible to correct
the defect using the usual facial lifting techniques, where the frontal flap is performed
cranially. Therefore, it was necessary to make an atypical incision to help this European
patient, who had emigrated to Brazil exclusively in an attempt to find treatment for
his problem. Reverse frontal cosmetic surgery was the idealized surgical technique
for the case. It is an innovative technique without prior publication in the literature.
CASE REPORT
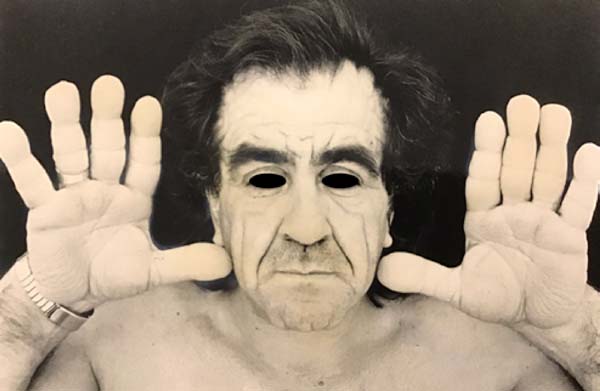
56-year-old Italian patient diagnosed with pachydermoperiostosis with thickening of
the dermis and epidermis (pachydermia), acropachy, and periostosis (Figure 1). The cutaneous manifestation was more pronounced in the frontal region of the face
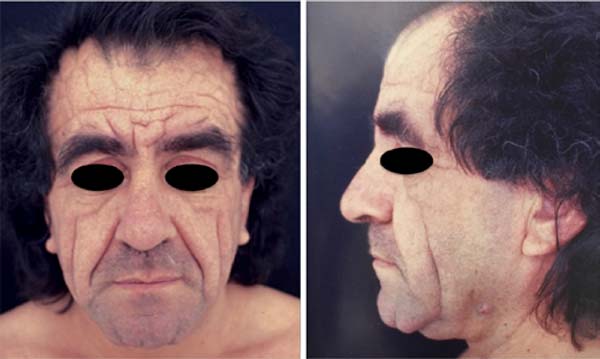
with the presence of inelastic and redundant skin and with the formation of deep grooves,
which generated aesthetic discomfort for the patient (Figure 2). Due to the characteristics of the skin and the distance from the coronal incision
to the site to be treated, traction in the cranial direction would be ineffective.
Therefore, an atypical facelift incision, called reverse frontal, was conceived, where
the front flap is pulled in the caudal direction.
Figure 1 - Patient with pachydermia, acropathy and swelling of fingers.
Figure 1 - Patient with pachydermia, acropathy and swelling of fingers.
Figure 2 - Left: Preoperative frontal view; Right: Preoperative view from profile.
Figure 2 - Left: Preoperative frontal view; Right: Preoperative view from profile.
METHODS
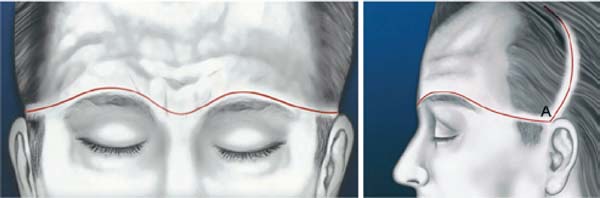
The incision begins at the root of the helix at point A, outlines the eyebrow in a
sinuous line half a centimeter from the implantation of the eyebrow hairs, rises to
the glabella region, curves towards the root of the nose, and it is found with identical
dimensions on the other side (Figure 3). From point A, a curved line rises leaning towards the medial direction, at a distance
of 2 cm, to allow a secure nutritional basis for the entire flap. The intention is
to reduce the distance between the area to be pulled and the area of the incision,
to obtain greater traction, thus allowing correction of the appearance of the face.
After the incision, a cranial subgaleal detachment of the forehead was performed,
and the frontal and interciliary muscles were treated. Flap traction is performed
in the caudal (reverse) direction with subsequent marking and resection of the cutaneous
excess in the frontal region, symmetrically, resulting in a supraciliary scar (Figures 4 and 5).
Figure 3 - Trace from the root of the helix (point A) around the eyebrows, curving towards the
root of the nose, finding identical dimensions on the other side. From point A, a
curved line leans towards the medial direction, at a distance from each other, which
allows a secure nutrition base for the entire flap.
Figure 3 - Trace from the root of the helix (point A) around the eyebrows, curving towards the
root of the nose, finding identical dimensions on the other side. From point A, a
curved line leans towards the medial direction, at a distance from each other, which
allows a secure nutrition base for the entire flap.
Figure 4 - Photo of the technique being performed intraoperatively. Resection of excess tissue
in the frontotemporal region.
Figure 4 - Photo of the technique being performed intraoperatively. Resection of excess tissue
in the frontotemporal region.
Figure 5 - Photo of the technique being performed intraoperatively. Caudal flap traction.
Figure 5 - Photo of the technique being performed intraoperatively. Caudal flap traction.
The middle and lower thirds of the face were treated through a pre-intracapillary,
retroauricular, pre-auricular and pre-tragal MACE incision, reaching point A, with
subsequent broad flap detachment, SAMS plication and medial platysma approach. Skin
spindle resection was performed in the nasogenian grooves, which, being pronounced,
required local traction following the same concept used in the upper third. A skin
excision was performed on the submentum to treat excess skin in the mentonian region.
RESULTS
The caudal traction of the flap, made using a supraciliary incision, made it possible
to correct the defect in the frontal region without altering the capillary implantation
line or producing excessive eyebrow rise. The treatment of the middle and lower thirds
of the face, added to the resection of the skin spindle in the nasogenian groove and
submentum, also allowed the rejuvenation of the face in a broad aspect and the smoothing
of the grooves (Figures 6 and 7).
Figure 6 - Front view of the pre and postoperative period.
Figure 6 - Front view of the pre and postoperative period.
Figure 7 - Pre and postoperative profile view.
Figure 7 - Pre and postoperative profile view.
However, preoperative counseling is essential so that the patient becomes aware that
the scars will become more apparent, but are necessary to obtain a more effective
result.
DISCUSSION
There is still no consensus for the treatment of frontal and nasoglabelar wrinkles,
and the best surgical option for patients diagnosed with pachydermoperiostosis has
not been established. Endoscopic lifting is one of the most used techniques because
it has reduced surgical time and less apparent scarring. However, it presents as a
disadvantage the difficulty in positioning the eyebrow and the persistence of redundant
skin, since, with this technique, only the soft tissues are elevated, without performing
skin resections4,18.
Transpalpebral approaches are another alternative for the treatment of the frontal
region, but they are indicated only for small degrees of ptosis of the eyebrow and
have frequent recurrence. More recently, the use of botulinum toxin, hyaluronic acid,
support threads, and surgical techniques, such as gliding brow lifting, have been
described as less invasive options for the treatment of the frontal region19,20,21,22. These techniques are also indicated for cases with less skin excess since the tissues
are not resected.
In the case presented, the redundancy of the skin was more pronounced in the frontal
region, mainly in the caudal third, near the eyebrow. Therefore, correction would
not be possible using the existing coronal rhytidoplasty techniques, since the skin
tissue had an inelastic characteristic. Traction of the flap in the cranial direction
would be ineffective in this case due to the distance between the incision and the
area to be corrected.
In the literature, there are descriptions of the treatment of the frontal region with
the traditional coronal incision. However, this method has the disadvantage of the
need to subject the patient to multiple surgical procedures to correct excess skin
in the supraciliary region2,23.
Therefore, the author of this article developed the reverse frontal lift technique,
which allows treating excess skin in the caudal third of the forehead, while attenuating
frontal and nasoglabellar wrinkles. The same concept of local traction applies to
the nasogenial sulcus region, which will not be corrected only with SAMS traction
and overlying skin. The burden of local resections is the most apparent scarring,
however, accepted by this patient without resistance.
CONCLUSION
Despite the wide range of facelift techniques, surgeons are not free to face challenging
cases that must be addressed through atypical incisions. The reverse frontal elevation
technique was created for a specific case of pachydermoperiostosis. When well indicated
for application in rare cases, this technique can be used to achieve good results.
Despite the increased exposure to the scar, with a layered suture and carefully coaptized
skin, it is possible to achieve a satisfactory result.
COLLABORATIONS
|
RP
|
Final manuscript approval, Project Administration, Realization of operations and/or
trials, Writing - Original Draft Preparation
|
|
GHP
|
Analysis and/or data interpretation, Final manuscript approval, Supervision
|
REFERENCES
1. Supradeeptha C, Shandilya SM, Reddy KV, Satyaprasad J. Pachydermoperiostosis - a case
report of complete form and literature review. J Clin Orthop Trauma. 2014 Mar;5(1):27-32.
2. Taichao D, Fuling L, Hengguang Z. Comprehensive surgical strategies for the management
of pachydermoperiostosis. Facial Plast Surg. 2018 Jun;34(3):330-4.
3. Barrett DM, Casanueva FJ, Wang TD. Evolution of the rhytidectomy. World J Otorhinolaryngol
Head Neck Surg. 2016;2(1):38-44.
4. Pontes R. O universo da ritidoplastia. Rio de Janeiro: Revinter; 2011.
5. Hollander E. In: Plastische(Kosmetische) Operation: KritischeDarstellungihresgegenwartigen,
Stands. Berlin: Urban and Schwarzenberg; 1932:1e17.
6. Lexer E. Leipzig: JA Barth; 1931.
7. Kaplan JL. Skin only facelift. Medscape Drugs Dis. 2014.
8. Hunt HL. Plastic surgery of the head, face, and neck. Philadelphia: Lea & Febiger;
1926.
9. Joseph J. NasenplastiK und sonstige gesichtsplastik: nebst einem Anhang über mammaplastik.
Ant Labitzsch Leipzig 1931:507-509
10. Liang MD. Temporal approach to corrugator laser ablation. In: Ramirez OM, Rollin DK,
eds. Endoscopic plastic surgery. New York: Springer-Verlag; 1996. p. 28-35.
11. Pangman WJ 2nd, Wallace RM. Cosmetic surgery of the face and neck. Plast Reconstr
Surg. 1961;27:544-50.
12. Skoog T. Plastic Surgery: New Methods and Refinements. Philadelphia: W.B. Saunders;
1974.
13. Mitz V, Peyronie M. The superficial musculo-aponeurotic system (SMAS) in the parotid
and cheek area. Plast Reconstr Surg. 1976;58:80e88.
14. Pierce GW, Klabunde EH, Bergeron VL. Useful procedures in plastic surgery. Plast Reconstr
Surg (1946). 1947;2(4):358-361.
15. Castañares S. Forehead wrinkles, glabellar frown and ptosis of the eyebrows. Plast
Reconstr Surg.1964;34:406-13.
16. Regnault P. Complete face and forehead lifting, with double traction on "crow's-feet".
Plast Reconstr Surg. 1972;49(2):123-129.
17. Vinas JC, Caviglia C, Cortinas JL. Forehead rhytidoplasty and brow lifting. Plast
Reconstr Surg. 1976;57(4):445-454.
18. Chi JJ. Periorbital surgery forehead, brow, and midface. Facial Plast Surg Clin North
Am. 2016 May;24(1):107-17.
19. Fattahi T. Open brow lift surgery for facial rejuvenation. Atlas Oral Maxillofacial
Surg Clin North Am. 2016 Sep;24(2):161-4.
20. Moradi A, Watson J. Current concepts in filler injection. Facial Plast Surg Clin North
Am. 2015 Nov;23(4):489-94.
21. Pedroza F, Anjos GF, Bedoya, Rivera M. Update on brow and forehead lifting. Curr Opin
Otolaryngol Head Neck Surg. 2006 Aug;14(4):283-8.
22. Viterbo F, Auersvald A. Glinding brow lifting. Plast Reconstr Surg Glob Open. 2017
Sep;5(9 Suppl):186-7.
23. Lima JSF, Costa SM, Chiari Júnior A, Bezerra MM, Polizzi LQR, Polizzi RJ. Surgical
treatment of primary pachydermoperiostosis: report of two cases. Rev Bras Cir Plást.
2014;29(1):165-8.
1. Serviço de Cirurgia Plástica Professor Ronaldo Pontes, Cirurgia Plástica, Niterói,
RJ, Brazil.
Corresponding author: Ronaldo Pontes, Av. Sete de Setembro, 301, Santa Rosa, Niterói, RJ, Brazil. Zipe Code: 24230-251.
E-mail: servicopgronaldopontes@gmail.com
Article received: February 19, 2019.
Article accepted: February 29, 2020.
Conflicts of interest: none.