INTRODUCTION
Breast cancer is the most common non-cutaneous malignancy among women worldwide,
accounting for approximately 28% of new malignant tumor cases each year in
Brazil. In the biennium 2016-2017, the Brazilian National Cancer Institute
(Instituto Nacional do Câncer; INCA) estimated approximately 2,160 new cases in
the state of Ceará and 57,960 new cases of breast cancer for every 100,000 women
in Brazil1.
The breasts represent one of the most eloquent symbols of female sexuality,
adorning the female body, and any condition that compromises its structure
brings serious consequences to the patient’s physical and psychological
well-being.
The high incidence of breast cancer and the importance of the breasts for a good
quality of life in patients made breast reconstructions after mastectomy an
integral part of the cancer treatment plan.
In 1894, William Halsted published in the United States the technique known today
as classical radical mastectomy, which relies on total withdrawal of the breast
with an adequate margin of safety in the adjacent skin and subcutaneous tissue,
in monobloc, by removing the pectoralis major and minor muscles and the adipose
tissues in the region, which includes the axillary lymph nodes2. However, this technique greatly
compromised breast reconstructions as the skin was not preserved.
Over the years, more conservative techniques have emerged, such as the one
advocated by Patey, which preserves the pectoralis major muscle, and the Madden
technique, which preserves both the pectoralis muscles.
To progressively perform more conservative mastectomies, the skin-sparing
mastectomy was developed, which may or may not preserve the nipple-areola
complex (NAC) and emerged as a procedure that improved the reconstructed
breasts, using no less complex techniques, but less debilitating for the
reconstruction, through implants with alloplastic material. Preservation of the
breast skin envelope provides a satisfactory color tone, texture, and contour of
the reconstructed breast, either with a tissue expander, alloplastic implant,
lipografting, or deepidermized flaps2.
The use of prosthetic implants for breast reconstructions started in the early
1960s with implants filled with silicone gel. Over the years, implant technology
and surgical techniques have evolved, resulting in an improved quality of the
reconstructed breast3.
Alloplastic implants can be classified according to shape (round, natural,
anatomical, and conical), texture (smooth, textured, and coated with
polyurethane foam), and projection (high, extra-high, moderate, and low)4. The choice of implant is fundamental to
the normal and natural shape, providing more femininity to the thorax.
Breast reconstruction with an alloplastic implant presents early and late
surgical complications that are directly or indirectly related to the surgical
technique used to perform mastectomy and implantation of a synthetic
material.
OBJECTIVE
To analyze the complications found in a group of patients submitted for immediate
breast reconstructions using conical and non-conical prostheses performed in our
service from January 2016 to 2018.
METHODS
This is a cross-sectional, retrospective, observational cohort study that
analyzed the medical records of patients who were submitted for skin-sparing
total mastectomies due to breast cancer, with immediate breast reconstruction
using an extra-high conical prosthesis coated with polyurethane or a non-conical
prosthesis, performed by the Plastic Surgery and Reconstructive Microsurgery
Service at the Walter Cantídio University Hospital of the Federal University of
Ceará, in Fortaleza, CE.
Patients who had an outpatient follow-up of at least 6 months and whose
reconstruction did not require local or distant skin flaps were included. Those
who had an outpatient follow-up of <6 months or those who used local or
distant flap for breast reconstruction were excluded.
All breast implants were placed in the submuscular position, using the pectoralis
major muscle and serratus anterior muscle to create the pocket, followed by
muscular suture to connect the edges after placing the prosthesis. To finish the
procedure, the subcutaneous region was drained using a vacuum, which was removed
after a daily rate of ≤30 mL of the sero-hematic secretion was achieved.
RESULTS
The mean age of the patients was 47.1 years, ranging from 27 to 71 years.
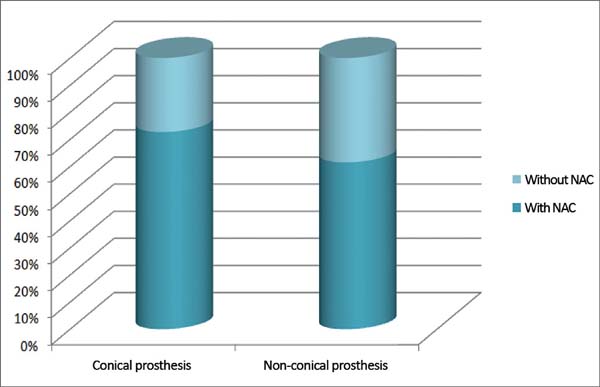
Immediate total breast reconstruction using a direct prosthesis after mastectomy
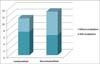
due to breast cancer was performed in 24 patients, with 13 (54.2%)
reconstructions performed with non-conical prostheses and 11 (45.8%) with
conical prostheses. The NAC was preserved in 8 (72.7%) patients with conical
prostheses and in 8 (61.5%) with non-conical prostheses; however, the NAC in 3
(27.3%) patients with conical prostheses and in 5 (38.5%) with non-conical
prostheses was not preserved (Figure 1).
Regarding the reconstructed side, 12 procedures were performed on the right
breast and 12 on the left breast.
Figure 1 - Proportion of conical and non-conical prostheses in all analyzed
patients who underwent breast reconstruction and their relation with
the nipple-areola complex (NAC) preservation.
Figure 1 - Proportion of conical and non-conical prostheses in all analyzed
patients who underwent breast reconstruction and their relation with
the nipple-areola complex (NAC) preservation.
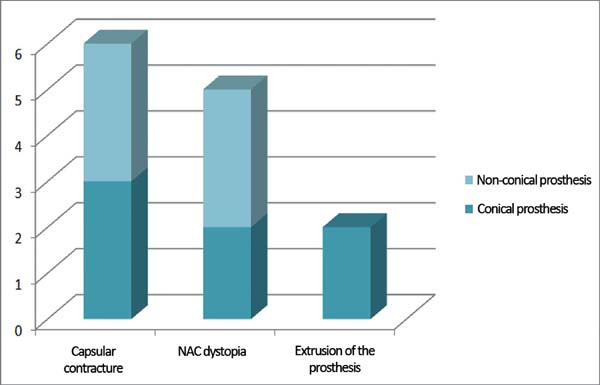
Complications occurred in 13 (54.1%) patients, with capsular contracture that
occurred in 6 (25%) patients as the most common (Figure 2). In patients with conical prostheses, 3 experienced
capsular contractures, 2 NAC dystopias (Figure 3) and 2 sore flaps with the formation of a hyperemic halo (Figure 4), similar to a pressure ulcer at
the tip of the conical prosthesis, which resulted in extrusion (Figure 5) and prosthesis removal. In
patients with non-conical prostheses, 3 capsular contractures and 3 NAC
dystopias occurred (Figure 6).
Figure 2 - Capsular contracture.
Figure 2 - Capsular contracture.
Figure 3 - Dystopia of the nipple-areola complex (NAC).
Figure 3 - Dystopia of the nipple-areola complex (NAC).
Figure 4 - Hyperemic halo at the tip of the conical prosthesis.
Figure 4 - Hyperemic halo at the tip of the conical prosthesis.
Figure 5 - Extrusion of the prosthesis.
Figure 5 - Extrusion of the prosthesis.
Figure 6 - Frequency and types of complications in all analyzed patients who
underwent immediate breast reconstruction and their relation with
the use of conical and non-conical prostheses.
Figure 6 - Frequency and types of complications in all analyzed patients who
underwent immediate breast reconstruction and their relation with
the use of conical and non-conical prostheses.
No infection or death was found in this group of patients. Regarding the
preservation of NAC, 8 (50%) patients with preserved NAC had complications,
whereas 5 (62.5%) patients with no preserved NAC had complications.
No difference in the frequency of complications was observed between the right
and left breasts, since both presented an incidence of 50% of complications.
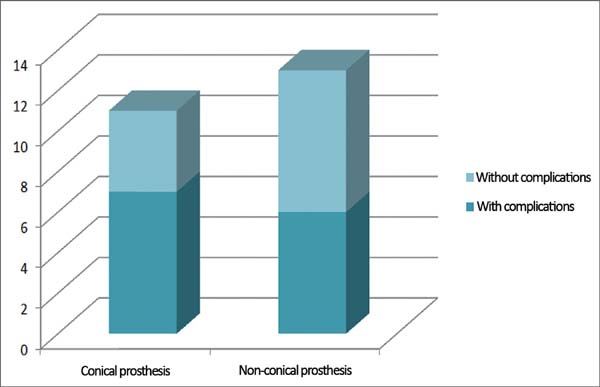
Conical prostheses presented the highest number of complications, with
complications in 7 (63.6%) patients, whereas only 6 (46.1%) patients with
non-conical prostheses had complications (Figure 7). In 6 patients submitted for radiotherapy, 2 (33.3%) had capsular
contracture as a complication, whereas among the 18 patients who did not undergo
radiotherapy, 4 (22.2%) had capsular contracture.
Figure 7 - Frequency of the use of conical and non-conical prostheses in the
immediate and total breast reconstruction cases analyzed and the
relation with the frequency of complications.
Figure 7 - Frequency of the use of conical and non-conical prostheses in the
immediate and total breast reconstruction cases analyzed and the
relation with the frequency of complications.
DISCUSSION
In the recent years, breast reconstruction for the treatment of breast cancer has
become essential for mastectomized patients due to its proven psychological and
physical benefits, because it allows faster return to social life, in addition
to an improved immunity, thus contributing to a more favorable prognosis5,6.
Choosing the format of the prosthesis directly influences the shape of the
reconstructed breast, providing a better superomedial projection in round
prostheses, a better anterior projection in conical prostheses and a more
natural appearance in anatomical prostheses for more hypotrophic breasts.
In this study, complications occurred in 54.1% of patients using the alloplastic
material, which is higher than most breast reconstruction services, with the
incidence ranging from 30% to 43%7,8.
The most common complication identified was capsular contracture, which occurred
in 6 (25%) patients, which is similar to that found in the researched
literature, ranging from 0.5% to 30%9,10.
The most serious complication identified was prosthetic extrusion that required
removal of the prosthesis that occurred in 2 patients who used the conical
prosthesis, representing 18.1% of the patients. This incidence was higher than
that of a previous study, which ranged from 1.2% to 5.3%, and higher than those
using non-conical prostheses, in which no cases of prosthetic extrusion were
observed11.
Extrusions occurring in the conical prostheses initially evolved from a sore area
(local hyperemic halo) formed in the myocutaneous flap on the tip of these
conical prostheses, with characteristics similar to pressure ulcers (Figures 4 and 5).
CONCLUSION
Immediate breast reconstructions with silicone prostheses is an excellent option
for selected patients, considering the low complexity of the procedure and short
surgical time; however, the disease severity, associated with the surgeon’s
experience in performing the mastectomy and the skin flap thickness, may weaken
the cutaneous cover of the prosthesis, which promotes extrusion.
Our study showed a higher frequency of complications in immediate breast
reconstructions with conical and non-conical prostheses when the NAC was not
preserved and when the patient is submitted for radiotherapy, which were
observed in patients using conical prostheses. This condition mainly occurs due
to the formation of a sore area at the tip of the conical prosthesis that
resulted in extrusion.
COLLABORATIONS
|
ROR
|
Analysis and/or interpretation of data; statistical analysis; funding
applications; data collection; study design; resource management;
research; methodology; and writing (preparation of the original
manuscript).
|
|
SGPP
|
Final approval of the manuscript; conceptualization; project
management; writing (review and editing); supervision; and
observation.
|
REFERENCES
1. Brasil. Ministério da Saúde. Instituto Nacional de Câncer José
Alencar Gomes da Silva (INCA). Estimativa 2016: Incidência de Câncer de Mama no
Brasil. Rio de Janeiro: INCA; 2016. [acesso 2018 Mar 12]. Disponível em:
http://santacasadermatoazulay.com.br/wp-content/uploads/2017/06/estimativa-2016-v11.pdf
2. Mélega JM. Cirurgia Plástica Fundamentos e Arte: Princípios Gerais.
2a ed. Rio de Janeiro: Guanabara Koogan; 2011.
3. Grabb WC, Smith JW. Cirurgia Plástica. 6a ed. Rio de Janeiro:
Guanabara Koogan; 2009.
4. Pitanguy I. Cirurgia Plástica: Uma visão de sua amplitude. 1a ed.
São Paulo: Atheneu; 2016.
5. Veiga DF, Veiga-Filho J, Ribeiro LM, Archangelo I Jr, Balbino PF,
Caetano LV, et al. Quality-of-life and self-esteem outcomes after oncoplastic
breast-conserving surgery. Plast Reconstr Surg.
2010;125(3):811-7.
6. Bellino S, Fenocchio M, Zizza M, Rocca G, Bogetti P, Bogetto F.
Quality of life of patients who undergo breast reconstruction after mastectomy:
effects of personality characteristics. Plast Reconstr Surg.
2011;127(1):10-7.
7. Almeida Júnior GL, Macedo JLS, Borges SZ, Souza AO, Henriques FAM,
Suschino CMH, et al. Reconstrução mamária imediata após cirurgia conservadora do
câncer de mama. Rev Soc Bras Cir Plást. 2007;22(1):10-8.
8. Bronz G, Bronz L. Breast reconstruction with skin-expander and
silicone prostheses: 15 years' experience. Aesthetic Plast Surg.
2002;26(3):215-8.
9. D'Alessandro GS, Povedano A, Santos LKIL, Santos RA, Góes JCS.
Reconstrução mamária imediata com retalho do músculo grande dorsal e retalho de
silicone. Rev Bras Cir Plást. 2015;30(2):163-71.
10. Mathes SJ, Hentz VR. Plastic surgery. 2a ed. Philadelphia: Saunders;
2006. p. 26-33.
11. Farah AB, Nahas FX, Mendes JA. Reconstrução mamária em dois estágios
com expansores de tecido e implantes de silicone. Rev Bras Cir Plást.
2015;30(2):172-81.
1. Hospital Universitário Walter Cantídio,
Universidade Federal do Ceará, Fortaleza, CE, Brazil.
Corresponding author: Rogério de Oliveira Ribeiro, Rua Odilardo
Silva, nº 81 - Laguinho - Macapá - AP - Brazil , Zip Code 68908-182. E-mail:
roimed@yahoo.com.br
Article received: August 5, 2018.
Article accepted: October 4, 2018.
Conflicts of interest: none.