ABSTRACT
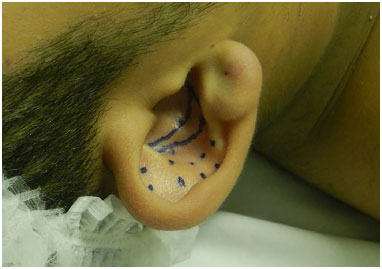
INTRODUCTION: Protruding ears are caused by poor development of the antihelix, hyperplasia of the concha, abnormal cephaloauricular angle, a large and prominent lobule, or any combination of the above.
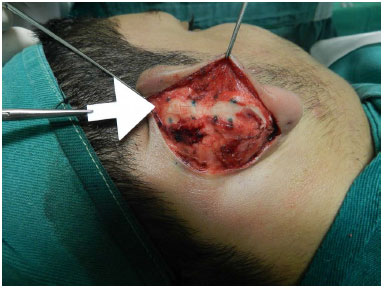
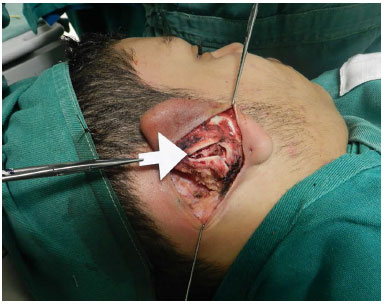
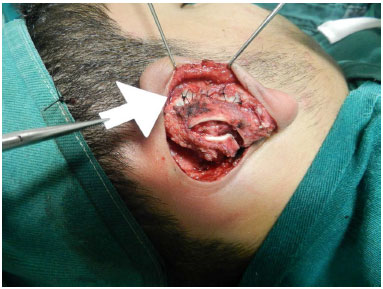
METHODS: A prospective study was performed, in which 60 patients who underwent otoplasty were followed up from January 2014 to January 2015 at the Hospital Municipal Barata Ribeiro.
RESULTS: Early complications included infection (0%), hematoma (1.6%), and skin necrosis (3.3%). Late complications included asymmetry (10%), recurrence (3.3%), extrusion of sutures (10%), granuloma formation (0%), hypertrophic scarring (0%), and keloid formation (0%). When patients were asked to rate the otoplasty, 3.3% stated that it was poor, 3.3% fair, 3.3% good, 3.3% very good, and 86.8% excellent.
CONCLUSION: The rates of early and late complications are similar to those described in the literature.
Keywords:
Reconstructive surgical procedures; Postoperative complications; External ear abnormalities; Auricle.
RESUMO
INTRODUÇÃO: Orelha em abano é caracterizada pelo pobre desenvolvimento da anti-hélice, hiperplasia da concha, ângulo céfalo-auricular anormal, lóbulo grande e proeminente ou qualquer combinação dos itens citados.
MÉTODOS: Foi realizado um estudo prospectivo, em que foram acompanhados 60 pacientes submetidos à otoplastia, no período de janeiro de 2014 a janeiro de 2015, no Hospital Municipal Barata Ribeiro.
RESULTADOS: Entre as complicações precoces, citamos infecção (0%), hematoma (1,6%) e necrose de pele (3,3%). Entre as complicações tardias: assimetria (10%), recidiva (3,3%), extrusão de pontos (10%), granuloma, cicatriz hipertrófica (0%) e queloide (0%). Quando os pacientes foram questionados quanto aos resultados obtidos com a otoplastia, 3,3% responderam que o resultado foi ruim, 3,3% regular, 3,3% bom, 3,3% ótimo e 86,8% excelente.
CONCLUSÃO: As taxas de complicações precoces e tardias são semelhantes às descritas na literatura.
Palavras-chave:
Procedimentos cirúrgicos reconstrutivos; Complicações pós-operatórias; Orelha externa/anormalidades; Pavilhão auricular.