



Original Article - Year 2026 - Volume 41Issue 1
Impact of Personality Disorders on Postbariatric Plastic Surgeries: Challenges and Psychological Considerations
Impacto dos transtornos de personalidade nas cirurgias plásticas pós-bariátricas: Desafios e considerações psicológicas
Alexandre Kataoka1, ; Camila Cristina Silva Mendes2; Renato Giannini1; Fabricio Luis Pinheiro1; Renato Rocha Lage3; Marcelo Prado1; Karine Rabello Borges2; Nikole Guimarães Lello1
; Camila Cristina Silva Mendes2; Renato Giannini1; Fabricio Luis Pinheiro1; Renato Rocha Lage3; Marcelo Prado1; Karine Rabello Borges2; Nikole Guimarães Lello1
ABSTRACT
Introduction The World Health Organization (WHO) classifies obesity as a chronic noncommunicable disease. This condition affects 63% of Brazilian adults. Although patients often seek reconstructive plastic surgery after bariatric surgery, many have unrealistic expectations, leading to dissatisfaction. A psychological evaluation is essential to manage expectations and prevent the worsening or onset of psychological disorders.
Objective To identify and manage real and imaginary expectations of postbariatric patients undergoing reconstructive plastic surgery by assessing potential disorders and psychological preparedness under multidisciplinary support.
Materials and Methods: The study included 203 patients (164 women and 39 men) who underwent reconstructive plastic surgery at Hospital Ruben Berta, in São Paulo, Brazil. All subjects underwent pre- and postoperative psychological evaluations, including the application of the Revised Neuroticism, Extraversion, and Openness Five-Factor Inventory (NEO-FFI-R) and a specific questionnaire. The patients signed an informed consent form.
Results Of the 203 patients, 162 presented psychological disorders: among women (n=136), these conditions included body dysmorphic disorder (n=49), somatic symptoms (n=23), bulimia (n=17), orthorexia (n=13), mood disorder (n=13), anorexia (n=10), muscle dysmorphia (n=6), and alcohol-related disorder (n=5); among men (n=28), they included muscle dysmorphia (n=12), alcohol-related disorder (n=6), body dysmorphic disorder (n=3), mood disorder (n=3), orthorexia (n=2), and somatic symptoms (n=2).
Discussion Although most patients underwent a psychological evaluation before the bariatric surgery, the lack of follow-up favored the persistence or worsening of the disorders, compromising the effectiveness of the reconstructive surgery and generating potential doctor-patient conflicts. Continuous follow-up contributes to body-image readjustment and relapse prevention.
Conclusion The integration of psychology and a multidisciplinary team from the decision to undergo bariatric surgery through the postoperative period is essential to maximize outcomes and patient satisfaction.
Keywords: bariatric surgery; compulsive personality disorder; obesity; patient care team; plastic surgery procedures
RESUMO
Introdução A obesidade, classificada pela Organização Mundial da Saúde (OMS) como doença crônica não transmissível (DCNT), afeta 63% dos adultos brasileiros. Após cirurgia bariátrica, os pacientes frequentemente buscam cirurgia plástica reparadora; contudo, muitos mantêm expectativas irreais, o que favorece a insatisfação. A avaliação psicológica é fundamental para manejar expectativas e prevenir o agravamento ou o surgimento de transtornos psíquicos.
Objetivo Identificar e manejar expectativas reais e imaginárias de pacientes pósbariátricos em cirurgia plástica reparadora, avaliando possíveis transtornos e preparo psicológico, com apoio multidisciplinar.
Materiais e Métodos Realizamos um estudo com 203 pacientes (164 mulheres e 39 homens) submetidos a cirurgia plástica reparadora no Hospital Ruben Berta, em São Paulo. Todos passaram por avaliações psicológicas pré e pós-operatória, aplicação do instrumento Revised Neuroticism, Extraversion, and Openness Five-Factor Inventory (NEO FFI-R) e questionário específico. Foi obtido consentimento esclarecido.
Resultados Dos 203 pacientes, 162 apresentaram transtornos psíquicos: entre as mulheres (n=136), foram observados transtorno dismórfico corporal (n=49), sintomas somáticos (n=23), bulimia (n=17), ortorexia (n=13), transtorno de humor (n=13), anorexia (n=10), vigorexia (n=6) e transtorno relacionado ao álcool (n=5); e entre os homens (n=28), vigorexia (n=12), transtorno relacionado ao álcool (n=6), transtorno dismórfico corporal (n=3), transtorno de humor (n=3), ortorexia (n=2) e sintomas somáticos (n=2).
Discussão Embora a maioria dos pacientes tenha feito avaliação psicológica antes da cirurgia bariátrica, a falta de acompanhamento favoreceu a persistência ou o agravamento de transtornos, o que compromete a eficácia cirurgia da reparadora e gera possíveis conflitos médico-paciente. O acompanhamento contínuo ajuda na readequação da imagem corporal e na prevenção de recaídas.
Conclusão A integração de psicologia e equipe multidisciplinar desde a decisão pela cirurgia bariátrica até o pós-operatório é essencial para maximizar os resultados e a satisfação.
Palavras-chave: cirurgia bariátrica; cirurgia plástica; equipe de assistência ao paciente; obesidade; transtorno da personalidade compulsiva
Introduction
“The World Health Organization (WHO) classifies obesity as a highly complex Chronic Noncommunicable Disease (NCD) and is considered a challenge of the 21st century, with global repercussions. According to the Atlas of the Food and Nutri-tional Situation in Brazil, published by the Ministry of Health in 2020, a survey involving 12,776,938 adults revealed that 63% of them are overweight. Obesity is a multifactorial condition, presenting a significant risk due to its comorbid-ities and psychosocial impacts that worsen with increased weight”.1 The pursuit of a new body image often leads postbariatric patients to reconstructive plastic surgery. However, a large proportion of these patients do not fully understand what surgery can achieve and the potential results. Even after consultation and medical guidance, a significant percentage of patients perpetuate an idealized body image and, consequently, may be dissatisfied with the outcome.
In Civilization and Its Discontents, Freud defines sublima-tion as the defense mechanism that takes energy from something potentially harmful and transforms it into some-thing useful, modifying both the object and the goal.2 This unconscious modification alleviates and protects the subject from psychic suffering, such as anxiety, frustration, and mental conflict.
“Preoperative assessment and preparation are essential for postbariatric patients, especially the psychological and social aspects permeating everything from the decision-making process to the entire recovery and adaptation to the new life. This stage includes assessments, guidance, clarification of realistic treatment expectations, and in-depth interviews regarding the subject’s relationship with food, their life history, and their relationship with their own body [...]. Managing expectations and idealizations regarding bariatric surgery through self-knowledge and awareness of the complexity of this process is key to a healthy adaptation.”3
Disorders existing during the period of obesity without adequate psychological support can reappear or trigger new conditions after bariatric surgery or body contouring.
The onset of new personality disorders or the worsening of preexisting conditions can result in weight regain that may be partial or very significant.
The article “Body Dysmorphic Disorder and the influence of the media in demand for plastic surgery: the importance of proper evaluation” cites Dr. Gustavo Costa Goulart, who highlighted that the perception of the body as one’s own seems natural and intuitive; however, in reality, it is not quite so: [...] “throughout life, the vision of the body will be marked not only by images but also by definitions (signifiers) and own sensations. So, we have a body that is apprehended by its imaginary aspect (appearing), by its symbolic aspect (being), and by its real aspect (body experience not imagined or symbolized by the subject and which emerges abruptly).”4
A patient seeking reconstructive plastic surgery after bariatric surgery may be feeling vulnerable, having low self-esteem, and often experiencing a profound existential void. Thus, they end up isolating themselves from society or trying to fit in by masking their feelings of failure, using humor, or even playing the victim to get attention from their peers.
It is the psychologist’s role to identify and treat psycho-logical changes that may hinder the process, guiding the patient from bariatric surgery to reconstructive plastic sur-gery, and preparing them for the profound bodily, social, and sexual changes that may occur in their life.
Objective
The current study aimed to specify and manage the real and imagined expectations of postbariatric patients undergoing reconstructive plastic surgery procedures with support from a multidisciplinary team. The study also aimed to evaluate and identify potential disorders, risks, and the level of psychological preparedness of these patients for such surgi-cal treatments.
Materials and Methods
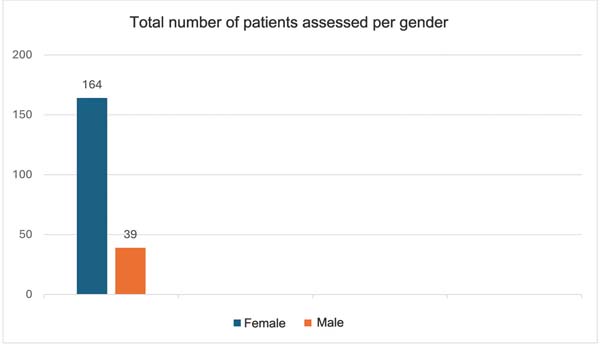
The present study comprised 203 postbariatric patients of both genders (164 women and 39 men) who underwent reconstructive plastic surgery with 4 different teams of plastic surgeons at Hospital Ruben Berta, in the city of São Paulo, Brazil (►Fig. 1)

All participants agreed to undergo unpaid consultations and preand postoperative testing for reconstructive plastic surgery with the same psychologist, as well as personality testing, including the Revised Neuroticism, Extraversion, and Openness Five-Factor Inventory (NEO) Five-Factor Inventory (NEO FFI-R) and a preoperative psychological assessment questionnaire for postbariatric plastic surgery. All patients signed an informed consent form for psychological treat-ment, ensuring compliance with the ethical criteria and requirements of the research.
Personality inventory application
All patients who had their initial consultation with a plastic surgeon and a psychologist received via email the NEO FFI-R, which is a widely-used tool to assess personality traits based on the Big-Five personality model, which addresses five main dimensions: neuroticism, extraversion, openness, agreeable-ness, and conscientiousness. The NEO-FFI-R is a reviewed, reduced version of the Revised NEO Personality Inventory (NEO PI-R), consisting of 60 items that objectively measure these 5 dimensions. In clinical and organizational settings, this inventory provides a precise assessment of personality traits, and it is useful in research and psychological practice.5 We asked patients to complete a personality inventory and questionnaires based on how they perceive themselves and how they think they normally behave in any given situation.
Results
We analyzed the results of the NEO-FFI-R and questionnaires to identify consistencies in each subject’s characteristics, assuming that human attributes are stable, steady features that, combined, form a personality.5
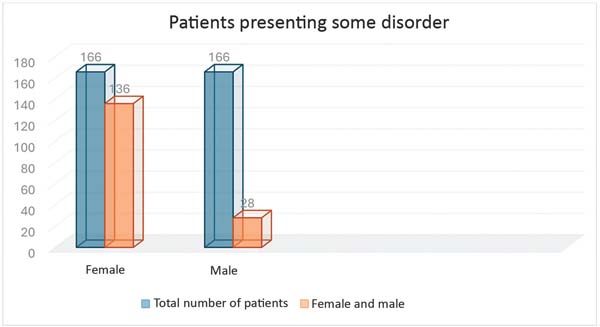
Of the 203 patients monitored, 162 (136 women and 28 men) presented some mental disorder. None of the identified disorders led to the suspension of postbariatric plastic surgery (►Fig. 2).

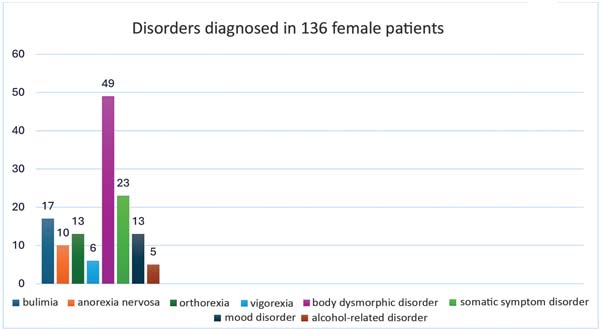
Among the 136 women with some mental condition, we identified body dysmorphic disorder (n ¼ 49 patients), so-matic symptom disorder (n ¼ 23 patients), bulimia nervosa (n ¼ 17 patients), orthorexia (n ¼ 13 patients), mood disor-der (n ¼ 13 patients), anorexia nervosa (n ¼ 10 patients), muscle dysmorphia (n ¼ 6 patients), and alcohol-related disorder (n ¼ 5 patients) (►Fig. 3).

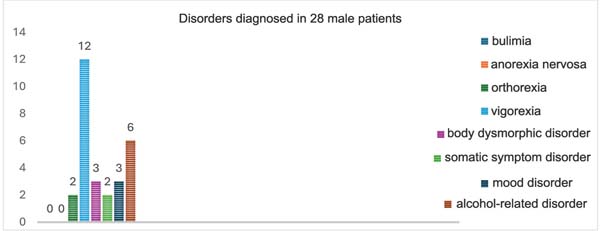
Regarding the 28 male patients with some mental condi-tion, we identified muscle dysmorphia (n ¼ 12 patients), alcohol-related disorder (n ¼ 6 patients), body dysmorphic disorder (n ¼ 3 patients), mood disorder (n ¼ 3 patients), orthorexia (n ¼ 2 patients), and somatic symptom disorder (n ¼ 2 patients). No male patients presented with bulimia nervosa or anorexia nervosa (►Fig. 4).

Discussion
The current study evaluated the preand postoperative motivations and expectations of patients, their psychological state, and the existence of any psychological disorders that would contraindicate reconstructive plastic surgery after bariatric surgery. Our analysis encompassed personality disorders, anxiety disorders, obsessive-compulsive disorders (OCDs), somatic symptoms, and, in particular, eating disor-ders, which we believe to be the most common in postbari-atric patients.
We observed that most patients underwent preoperative psychological evaluation for bariatric surgery, but with no follow-up. This discontinuity leads many patients to seek reconstructive plastic surgery with the same preexisting disorders, or even with worsening of their psychopathologi-cal condition. This situation undermines the procedure’s effectiveness and can negatively impact the doctor-patient relationship, possibly leading to legal action.
Our results indicate that ongoing psychological support is crucial for postbariatric patients; however, it did not occur in most cases herein analyzed. This support is essen-tial for body-image readjustment, development of a new identity after weight loss, and management of the signifi-cant changes that will occur in the patient’s life, regardless of the presence of preexisting psychological disorders. Such need reinforces the importance of a humanized multidisci-plinary team with psychological support throughout the entire surgical process, from the preoperative period to body remodeling.
Continuous, collaborative interaction with the psycholo-gist can enhance the patient’s well-being. This relationship provides a broader, more effective approach, which encom-passes surgical outcomes and physical, psychological, and emotional aspects. Providing psychological support before and after surgery helps manage patients’ anxieties and expectations, leading to a healthier, more balanced recovery. The involvement of a psychologist in this journey promotes an integrated intervention, enhancing the physical benefits of surgery and contributing to the patient’s emotional sta-bility and mental health. This integrated intervention enhan-ces satisfaction for the patients and the surgical team, fostering collaboration among the several healthcare pro-fessionals involved in the treatment.
Detailed description of the identified disorders
Some mental disorders presented by our patients are within the OCD spectrum, including body dysmorphic disorder and muscle dysmorphic disorder (vigorexia).
According to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR),6 OCD features are obsessions, compulsions, or both. Obses-sions are recurrent and persistent thoughts, impulses, or images perceived as intrusive and unwanted. Compulsions are repetitive behaviors or mental acts that the subject feels compelled to perform in response to an obsession or accord-ing to rules requiring rigid enforcement. In the following paragraphs, we will detail the mental disorders observed among the patients herein analyzed with their respective International Classification of Diseases, Tenth Revision (ICD-10),7 codes.
Body dysmorphic disorder (F45.22)
Subjects with body dysmorphic disorder (formerly known as dysmorphophobia) exhibit excessive preoccupation with one or more perceived defects in their physical appearance, considering themselves ugly, unattractive, abnormal, or de-formed. However, these flaws are not observable by others or appear mild. Body image distortion is central to the disorder, causing patients to perceive themselves in a way that does not correspond to reality.
Muscle dysmorphic disorder (vigorexia; F45.2/F42)
This psychological condition features an obsession with not having sufficiently-developed muscles, even when the sub-ject already presents regular or well-defined musculature. It is related to body-image distortion, similar to other disorders such as anorexia, but with a focus on gaining muscle mass.
Patients with muscle dysmorphia exhibit behaviors such as obsession with exercise, excessive concern with diet for muscle gain, distorted body image, and use of substances, including anabolic steroids, to accelerate muscle gain, which entails severe health (cardiac, hepatic, and hormonal) risks.
Eating disorders
Eating disorders are persistent disruptions in eating habits or behaviors. This dysfunction affects food intake or absorption, significantly compromising the physical health and psycho-social well-being of the affected subjects.
Bulimia nervosa (F50.2)
Subjects with bulimia nervosa have recurrent episodes of binge eating, that is, the intake of large amounts of food, accompanied by a feeling of loss of control. Feeling guilty, the patient uses inappropriate compensatory behaviors to avoid weight gain, such as self-induced vomiting. These patients are usually ashamed of their eating problems and try to hide their symptoms. Therefore, binge eating often occurs in secret, and the episode continues until the subject feels uncomfortably full or in pain.
Anorexia nervosa (F50.0)
Anorexia nervosa is an intense fear of gaining weight or becoming fat, even in underweight subjects. This preoccupa-tion remains despite weight loss; in fact, it may increase as weight decreases. In addition to food restriction, some patients with anorexia nervosa may exhibit excessive levels of physical activity, exacerbating their weight loss. An in-crease in physical activity usually precedes the onset of the disorder, and, throughout its course, high activity levels accelerate weight loss. During treatment, controlling exces-sive activity can be challenging, hindering weight recovery.
Orthorexia nervosa (not yet recognized as a formal mentaldisorderintheICD-10)
Orthorexia is a pathological obsession with a diet considered “healthy” and “pure.” This rigidity leads to food restriction and can result in nutritional deficiencies and weight loss. Although not officially recognized as a specific eating disor-der by the DSM-5 nor the ICD-10, it is widely discussed in clinical settings. Orthorexia can have severe consequences, such as malnutrition, excessive weight loss, and impairments in social and emotional life.
Its characteristics include excessive focus on food quality, with rigorous evaluation of ingredients and manufacturing processes, restriction of food groups, feelings of moral superiority, and social isolation, as the subject avoids eating out because they do not trust the standards of the food offered.
Somatic symptom disorder (F45.1)
Somatic symptom disorder refers to the presence of one or more physical symptoms that cause significant distress or impairment in the subject’s daily life, even without an adequate medical explanation. The emotional or psycholog-ical response to the physical discomfort is disproportionate, and the patient tends to worry excessively about these symptoms, which worsens their quality of life.
Mood disorders (F30-F39)
This group of psychological conditions involves significant and persistent changes in mood, affecting how a subject feels, thinks, and acts. The manifestations can range from episodes of deep depression to periods of intense euphoria, as in the case of bipolar disorder.
The main characteristics include persistent mood swings (extreme sadness, exaggerated euphoria, or irritability), changes in sleep and appetite patterns, loss of interest in daily activities, low energy, fatigue, thoughts of worthless-ness, guilt, or suicide (the last three in cases of depression), impulsivity, grandiose feelings, or risky behavior (in cases of mania/hypomania).
Alcohol-related disorders (F10.220)
Moderate or severe alcohol-use disorder refers to a prob-lematic pattern of consumption that results in significant impairment. A key aspect is excessive consumption, in which the subject repeatedly ingests large amounts of alcohol, frequently exceeding the limits considered safe. Furthermore, there is impaired control, manifesting as difficulty in reducing or stopping consumption, even after attempts to do so. Alcohol tolerance may also increase, leading to the need for larger amounts to obtain the same effects. Withdrawal symptoms are another striking feature, with tremors, sweating, anxiety, and irritability being fre-quent after reducing or stopping alcohol use. Alcohol con-sumption also has negative consequences, impacting health issues, interpersonal relationships, work or school perfor-mance, and potentially involving the subject in dangerous activities. Additionally, the use frequently occurs in situa-tions that pose a risk to health or safety, such as when driving under the influence of alcohol. Finally, persistent use is evident, as the subject continues to consume alcohol even after recognizing physical or psychological problems related to this substance.
Conclusion
Adopting a multidisciplinary approach from the initial deci-sion to undergo bariatric surgery through the postoperative period of bariatric and reconstructive plastic surgeries is key to the success of the treatment. The inclusion of regular psychological consultations in this process is essential to help the patient adapt to the physical and emotional changes resulting from the surgeries, promoting not only an im-proved quality of life but also more effective integration between the clinical and surgical teams.
This holistic approach maximizes therapeutic and surgi-cal outcomes, it has a positive impact on the patient’s overall well-being, it benefits all professionals involved, and it ensures more comprehensive, humane treatment, and pa-tient satisfaction with the results.
REFERENCES
1. Martins AC, Nicodemo D, Suzuki VY, Sales SS, Albuquerque LM. Avaliação psicológica em cirurgia plástica pós-bariátrica: uma revisão de escopo. Rev Bras Cir Plást 2024;39(03):e0948. Doi: 10.5935/2177-1235.2024RBCP0948-PT
2. Dias FC. O conceito de dessublimação repressiva em Herbert Marcuse. [tese (Mestrado em Filosofia)]. Porto Alegre: Instituto de Filosofia e Ciências Humanas, Universidade Federal do Rio Grande do Sul; 2023
3. Almeida IM, Nespoli NS. Para além da bariátrica: revisão de literatura sobre as possíveis consequências psíquicas da cirurgia. Rev Psicol Saúde 2021;13(04):139-152. Doi: 10.20435/pssa.v13i4.1328
4. Kataoka A, Lage RR, Mendes CCS, Soares NG. O Transtorno Dismór-fico Corporal e a influência da mídia na procura por cirurgia plástica: a importância da avaliação adequada. Rev Bras Cir Plást 2023;38(01):e0645. Doi: 10.5935/2177-1235.2023RBCP0645-PT
5. Plataforma Vetor. Ferramentas de avaliação psicológica [Internet]. São Paulo: Vetor Editora; c2024 [citado em 2024 set 7]. Disponível em: https://www.vetoreditora.com.br
6. American Psychiatric Association. Manual Diagnóstico e Estatís-tico de Transtornos Mentais: DSM-5-TR. 5ª ed., texto revisado. Porto Alegre: Artmed; 2023
7. World Health Organization (WHO). ICD-10: International Statis-tical Classification of Diseases and Related Health Problems: Tenth Revision. 2nd ed. Genebra: World Health Organization; 2004. Disponível em: https://iris.who.int/handle/10665/42980
1. Plastic Surgery Department, Hospital Ruben Berta, São Paulo, SP Brazil
2. Psychology Department, Hospital Ruben Berta, São Paulo, SP, Brazil
3. Plastic Surgery Department, Hospital da Baleia, Belo Horizonte, MG, Brazil
Address for correspondence Alexandre Kataoka, Avenida Antártico, 381, Cj. 108, Jardim do Mar, São Bernardo do Campo, SP, 09726-150, Brazil (e-mail: drkataoka@hotmail.com drkataoka@hotmail.com).
Article received: September 08, 2024.
Article accepted: August 26, 2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket