



Original Article - Year 2024 - Volume 39 -
Topographic anatomy of the masseteric nerve applied to masseteric-facial transfer
Anatomia topográfica do nervo massetérico aplicada à transferência massetérico-facial
Joaquín Calisto1,* ; Camila Rocha1; Augusto Garrido1; Camilo Prego Mujica2; Oscar Jacobo2
; Camila Rocha1; Augusto Garrido1; Camilo Prego Mujica2; Oscar Jacobo2
ABSTRACT
Introduction: The masseteric nerve is used as a nerve transfer in facial reanimation
surgery. Therefore, an anatomotopographic study of the approach of this
nerve applied to facial reinnervation surgery was performed. The objective
was to describe the anatomy of the masseteric nerve as a reference during
facial reanimation surgery.
Method: Data were analyzed in 15 masseteric regions belonging to adult cadavers fixed
in formaldehyde.
Results: In 12 cases, the nerve was positioned in relation to the posterior third of
the zygomatic arch. It emerged from the mandibular notch at an average
distance of 14.7 mm anterior to the condylar process and 8.8 mm from the
lower border of the zygomatic arch. The relationships with the masseteric
vessels were variable.
Conclusion: Anatomical knowledge of the nerve is essential for its approach.
Keywords: Anatomy; Facial paralysis; Facial nerve; Nerve regeneration; Nerve transfer; Face
RESUMO
Introdução: O nervo massetérico é utilizado como transferência nervosa na cirurgia de reanimação facial. Por conseguinte, foi realizado um estudo anatomotopográfico da abordagem deste nervo aplicado à cirurgia de reinervação facial. O objetivo foi descrever a anatomia do nervo massetérico como referência durante a cirurgia de reanimação facial.
Método: Os dados foram analisados em 15 regiões massetéricas pertencentes a cadáveres adultos fixados em formaldeído.
Resultados: Em 12 casos o nervo posicionava-se em relação ao terço posterior do arco zigomático. Emergiu da incisura mandibular a uma distância média de 14,7mm prévio ao processo condilar, e 8,8mm da borda inferior da arcada zigomática. As relações com os vasos massetéricos foram variáveis.
Conclusão: O conhecimento anatômico do nervo é indispensável para a sua abordagem.
Palavras-chave: Anatomia; Paralisia facial; Nervo facial; Regeneração nervosa; Transferência de nervo; Face.
INTRODUCTION
Facial paralysis is a condition caused by the involvement of the facial nerve at any point along its path. Facial movement can be restored using several techniques. The masseteric nerve is used as a nerve transfer in facial reanimation surgery to treat facial paralysis, with good functional and aesthetic results1, especially when the transfer is performed to reinnervate the buccal muscles.
Consequently, oral continence and facial expression are permitted, thus improving the quality of life of patients. Masseteric nerve transfer can be total or partial, the latter as a “babysitting” procedure, with the purpose of maintaining muscle viability during the axonal regeneration process of transfacial facial nerve grafts2. The contralateral facial nerve used as a transfacial graft requires a period of 9 to 12 months for the axons to migrate through the graft, causing the facial muscles to be paralyzed during this time to atrophy. Using the masseteric nerve as a partial nerve transfer maintains the viability of the transfacial graft.
The innervation of the masseter muscle depends on the mandibular branch of the fifth cranial nerve (trigeminal nerve). The mandibular nerve leaves the middle cranial fossa through the foramen ovale to the infratemporal region, where it divides into an anterior trunk and a posterior trunk. The temporomandibular nerve originates from the anterior trunk, from which the masseteric nerve arises. The masseteric nerve emerges towards the masseteric region, passing through the mandibular notch, below the zygomatic arch, reaching the deep surface of the masseter muscle3,4.
The use of the masseteric nerve as nerve transfer produces a minimal masticatory motor deficit in the masseter muscle since this muscle has proximal branches of the descending branch of the masseteric nerve. These allow the masseter muscle to maintain its masticatory function when the dominant branch is used for nerve transfer, in the same way as the synergy between the masseter muscle and the temporal muscle during mastication4.
Therefore, identification of the masseteric nerve is essential for performing this technique, for which an anatomotopographic study of the approach to this nerve was carried out and applied to facial reinnervation surgery.
OBJECTIVE
Study the topographic anatomy of the masseteric nerve approach, specifying the variations in its relationships with neighboring structures, as well as its path and termination, to obtain a rapid approach and dissection of the masseteric nerve.
METHOD
Fifteen masseteric regions were dissected from adult cadavers fixed in formaldehyde. Dissection material was used to approach the anatomical parts, as well as photographic equipment, a digital caliper to take measurements, and the use of Microsoft Windows Excel software for data collection and processing (Figure 1).


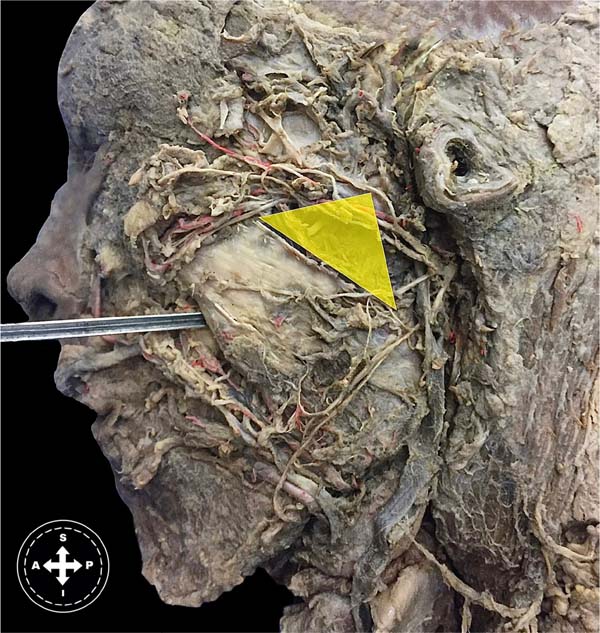
A preauricular approach similar to the in-plane facelift approach under the superficial musculoaponeurotic system (SMAS) was performed (Figure 2). The incision was made in the skin over the subzygomatic triangle between the zygomatic arch, the mandibular condyle, and the posterior border of the superficial fascicle of the masseter muscle (Figure 3). The masseteric pedicle was dissected from the inferior border of the zygomatic arch to its entry between the middle and deep fascicles of the masseter muscle (Figure 4). The masseteric nerve and masseteric vessels were identified. In addition, the length of the zygomatic arch was measured and the point of emergence of the masseter nerve in relation to it was identified, dividing it into three thirds (anterior, middle, and posterior) (Chart 1).
| Corpse side | Zygomatic arch length (mm) |
Relationship with 1/3 of the zygomatic arch | Distance from the lower edge of the arcade - point of emergence at the zygomatic notch (mm) | Condyle distance - emergence at the zygomatic
notch (mm) |
Length (mm) | Width at terminal sector (mm) | Relationship with masseteric A. and V. | |
|---|---|---|---|---|---|---|---|---|
| 1 | Left | 34.76 | Posterior | 2.34 | 4.63 | 25.74 | 1.17 | Superficial |
| 2 | Left | 39.53 | Posterior | 10.19 | 11.44 | 20.83 | 1.14 | Deep |
| 3 | Left | 44 | Posterior | 9 | 15.05 | 21.1 | 0.9 | Deep |
| 4 | Right | 51.4 | Posterior | 10.4 | 12.33 | 12.8 | 1.5 | Superficial |
| 5 | Right | 41.96 | Average | 12.41 | 27.91 | 19.7 | 0.58 | Superficial |
| 6 | Right | 42.06 | Anterior | 7.89 | 35.43 | 16.34 | 1.12 | Deep |
| 7 | Left | 33.36 | Posterior | 6.43 | 14.7 | 33.21 | 2.12 | Deep |
| 8 | Right | 53.26 | Average | 16.86 | 21.41 | 21.47 | 3.36 | Deep |
| 9 | Left | 25.83 | Posterior | 8.78 | 16.75 | 13.41 | 1.1 | Superficial |
| 10 | Left | 37.34 | Posterior | 6.1 | 11.94 | 14.04 | 1.75 | Superficial |
| 11 | Right | 49.54 | Posterior | 14.7 | 14.22 | 8.5 | 1.51 | Superficial |
| 12 | Right | 28.93 | Posterior | 11.15 | 8.34 | 11.7 | 1.59 | Superficial |
| 13 | Left | 31.55 | Posterior | 5.31 | 15.64 | 11.52 | 0.9 | Superficial |
| 14 | Left | 42.26 | Posterior | 9.62 | 5.11 | 23.31 | 2.38 | Deep |
| 15 | Right | 50.45 | Posterior | 1.9 | 5.4 | 18.6 | 1.9 | Deep |




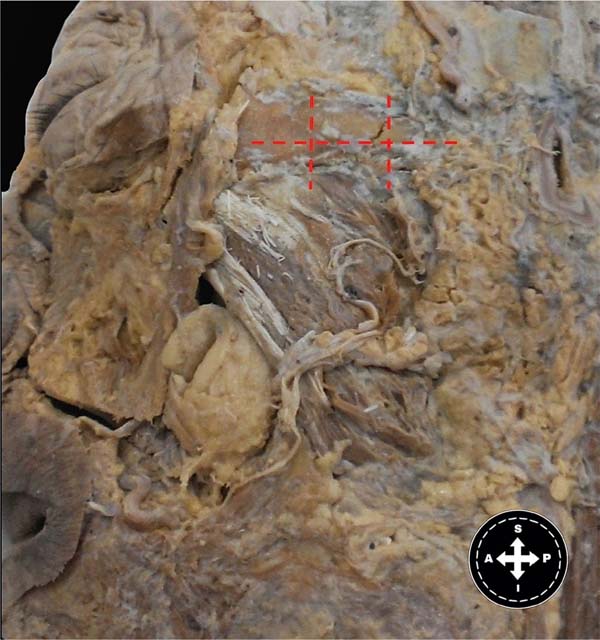

The relationship between the masseteric nerve and the masseteric vessels was also verified. The distance of the masseteric nerve course was measured from its emergence under the zygomatic arch to its termination. Then, the distance between the mandibular condyle and the point of emergence of the masseteric nerve under the zygomatic arch was measured. Finally, the distance between the origin of the masseteric nerve and the lower border of the zygomatic arch was measured (Figure 4).
RESULTS
The length of the zygomatic arch varied between 53.3 mm and 25.8 mm, with an average length of 40.4 mm and a median of 42.0 mm.
The emergence of the masseteric nerve was below the posterior third of the zygomatic arch in 80% of cases, below the middle third in 13%, and below the anterior third in 7%.
The distance between the inferior border of the zygomatic arch and the emergence of the masseteric nerve below it ranged from 16.9 mm to 1.9 mm, with a mean of 8.9 mm and a median of 9.0 mm. The distance between the mandibular condyle and the emergence point of the masseteric nerve below the zygomatic arch ranged from 35.4 mm to 4.6 mm, with a mean of 14.7 mm and a median of 14.2 mm.
In 53% of cases, the masseteric nerve was found superficial to the masseteric vessels, while in 47%, it was found deep to the masseteric vessels.
The length of the masseteric nerve path from its origin under the zygomatic arch to its termination varied from 33.2 mm to 8.5 mm, with an average of 18.2 mm and a median of 18.6 mm.
The width of the nerve at its termination varied from 3.4 mm to 0.6 mm, with an average of 1.5 mm and a median of 1.5 mm.
DISCUSSION
To topography the masseteric nerve, two palpable anatomical references on the surface were used: the mandibular condyle and the lower border of the zygomatic arch. These present little variability, and their anatomy is not distorted during the surgical procedure. Collar et al.1 propose the subzygomatic triangle for the topography of the masseteric nerve. This triangle is delimited by the zygomatic arch, a vertical line that passes through the mandibular condyle and the frontal branch of the facial nerve and is a questionable region for dissection of the masseteric nerve due to the presence of a structure with variable anatomy such as the frontal branch of the facial nerve.
Using the mandibular condyle, the lower border of the zygomatic arch, and the posterior border of the masseter muscle, a triangle with more precise limits can be determined to topograph the masseteric nerve, reinforcing a more accurate tool for facial reanimation surgery with nerve transfer of said nerve.
CONCLUSION
Reliable anatomical relationships have been determined for the identification of the masseteric nerve during masseteric-facial transfer surgery. It can be identified in an area between the zygomatic arch, masseter muscle, and mandibular condyle.
REFERENCES
1. Collar RM, Bryne PJ, Boahene KDO. The subzygomatic triangle: rapid, minimally invasive identification of the masseteric nerve for facial reanimation. Plast Reconstr Surg. 2013 Jul;132(1):183-8. DOI: 10.1097/PRS.0b013e318290f6dc
2. Rodriguez ED, Neligan PC. Plastic surgery: Volume 3: Craniofacial, head and neck surgery and pediatric plastic surgery. 4th ed. Philadelphia; Elsevier; 2017.
3. Kaya B, Apayadin N, Loukas M, Tubbs RS. The topographic anatomy of the masseteric nerve: A cadaveric study with an emphasis on the effective zone of botulinum toxin A injections in masseter. J Plast Reconstr Aesthet Surg. 2014;67(12):1663-8. DOI: 10.1016/j.bjps.2014.07.043
4. Cotrufo S, Hart A, Payne AP, Sjogren A, Lorenzo A, Morley S. Topographic anatomy of the nerve to masseter: an anatomical and clinical study. J Plast Reconstr Aesthet Surg. 2011;64(11):1424-9. DOI: 10.1016/j.bjps.2011.05.026
1. Facultad de Medicina Universidad de la
Republica, Departamento de Anatomía, Montevideo, Montevideo,
Uruguai
2. Facultad de Medicina Universidad de la
República, Cátedra de Cirugía Plástica Reparadora y Estética Hospital de
Clínicas, Montevideo, Montevideo, Uruguai
Joaquín Calisto Tacuarembó 1429/315, Montevideu, Uruguai, E-mail: joaquin.calisto@gmail.com
Artigo submetido: 06/08/2023.
Artigo aceito: 26/07/2024.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket