



Articles - Year 2001 - Volume 16 -
Transconjunctival Lower Lid Blepharoplasty
Blefaroplasia Inferior Transconjuntival
ABSTRACT
Although transconjunctval lower lid blepharoplasty was described many years long ago, it has only been in recent years, with the advent of laser; that its indication has become almost imperative. Thanks to this revival, transconjunctival blepharoplasty has been indicated in many situations. Authors have been using it more recently in most cases where resectioning or repositioning of the eyelid pads is necessary. Also, when indicated, scalpel or laser skin resection follows immediately. In this manner; since there are no lesions to nerve and muscle structures, mainly pre-tarsal structures, most of the complications of lower lid blepharoplasty can be avoided.
Keywords: Blepharoplasty; transconjunctival; laser
RESUMO
A blefaroplastia inferior transconjuntival foi descrita há muito tempo, mas somente nos últimos anos, com o advento do laser, é que sua indicação passou a ser quase imperativa. Devido a esse ressurgimento, a blefaroplastia transconjuntival voltou a ser indicada em muitas situações. Mais recentemente os autores a têm usado na maioria dos casos em que é necessária a ressecção de bolsas palpebrais ou seu reposicionamento. Quando também está indicada a ressecção de pele, esta é feita em seguida, com bisturi ou a laser. Assim, não há lesão das estruturas nervosas e musculares, principalmente pré-tarsais, o que evita a maioria das complicações das blefaroplastias inferiores.
Palavras-chave: Blefaroplastia; transconjuntival; laser
Transconjunctival blepharoplasty was initially proposed by Bourguet(1) in 1924. Tessier(2) has been using the transconjunctival incision for congenital malformations and traumatic deformities and blepharoplasty in selected patients, since 1955. New interest in the technique arose after Zarem and Resnick's publication in 1991, in which the authors extended the use of transconjunctival access to patients with fine skin wrinkling, and older patients with apparent excess skin(3,4). Many studies have shown the technique to be superior in terms of adequate resectioning of fat compartments, avoiding eyelid retraction and dry eye symptoms and providing lasting results. One of the main advantages described in relation to the conventional technique is that transconjunctival access does not lead to denervation of the pre-tarsal portion of the orbicularis muscle(3,5,6,7).
ANATOMY
The conjunctiva is a mucous membrane that covers the eyeball and meets the lower eyelid at a lower sac or fornix. The conjunctiva reflects from the eyeball to the eyelid, and the transition area is generally marked by a transverse plexus of vessels that covers the whole fornix in a variable fashion. Reflection ends medially at the caruncle and laterally at the lateral canthus ligament. The conjunctiva completely covers the internal surface of the eyelid. Anterior to the conjunctiva of the lower eyelid are the retractor muscles that emerge as tendinous extensions of the inferior rectus muscle and extend anteriorly. The extension involves the inferior oblique muscle, enters at the lower eyelid and inserts itself primarily at the lower portion of the tarsal plate (analogous to the aponeurosis of the elevator of the upper eyelid). The tarsi of the lower eyelid are at the upper margin of the eyelid with a maximum vertical dimension of approximately 4.5 to 5 mm. Anterior to the retractor muscle of the lower eyelid is the orbital septum, that extends from the arcus marginalis of the lower orbital rim to insert in the lower tarsus. The septum acts as a barrier against the anterior prolapse of intra-orbicular strutrures (fat for example). The weakening of the structure contributes to the appearing of orbital fat that prolapses the lower eyelid. There is a potential space between the levator muscles of the lower eyelid and the septum that communicates with the eyelid pads of the lower orbit. There are three different pads. The nasal pad is separated from the medial pads by the lower oblique muscle that emerges from the lower-nasal orbit running laterally and posteriorly upwards to its insertion at the posterior eyeball. The lower oblique muscle is completely located within the orbit. Although it may be identified during the resection of the nasal pad, identification is not necessary because the muscle is situated behind the surgical field. The larger vessels that feed the orbital pads are usually located within the nasal pad. These vessels can be visualized and should be avoided, if possible, by means of careful dissection of the vascular branches. The medial pad is separated from the lateral pad by an extension of the muscles of the lower eyelid. The lateral pad generally has the smallest anterior prolapse ofthe three and may be very difficult to access. In order to access this pad more easily, an incision to the fascia layer adjacent to the Lockwood ligament should be made, since this fascia frequently incarcerates the lateral fat pad. A lateral portion of this pad, known as the Aisler bursa, may extend upwards in the direction of the lateral canthus ligament(8,9,10). The surgeon's external digital pressure in the area may be necessary to induce prolapse of the pad in the surgical field. The lower lateral connection of the septum of the orbital margin is, apparently, very weak. Anterior migration of the septum over the lower margin in the direction of the malar eminence may occur, creating a potential space for all pads, known as the Aisler recess. In the most prominent part, these pads are known as malar pads, wrongly suggesting an extra-orbital etiology. Anterior to the septum is the anterior lamella of the lower eyelid, comprising the orbital orbicularis muscle and skin. Transconjunctival access does not cover the anterior lamella. At the medial lamella are the orbital septum and eyelid pads, and at the posterior lamella, the levator muscles or capsulopalpebral fascia and conjunctiva.
As the main vascular supply of the lower eyelid is at the plane of the orbicularis muscle, laser resurfacing of the lower eyelid can be performed at the same time as the transconjuntival blepharoplast, without concern of affecting vessels. Moreover, as the orbital septum remains intact, there are few post-surgical concerns related to retraction of the lower eyelid that may occur with the transcutaneous technique.
SURGICAL TECHNIQUE
The patient is submitted to supervised pre-operative sedation by the anesthesiologist, making local anesthetic infiltration easier. Tetracaine eye drops, a topical anesthetic, are applied to the lower cul de sac, to avoid discomfort when placing the metal eye protectors that should be used during the whole laser procedure.
Patients who are submitted to blepharoplasty and laser treatment receive 4 mg of intravenous dexametasone during surgery and continue this treatment by the oral route for 2 postoperative days, in order to avoid edema.
The surgeon should sit next to the patient's head. In transconjunctival lower lid blepharoplasty, performed after upper eyelid suture, we infiltrate the anesthetic 1/2 hour before the procedure for the adrenaline to take affect -we inject 1 to 2 ml of a of 2% lidocaine solution with epinephrine at 1:100.000 added to 0.5% bupivacaine once, using a 30-gauge needle through the conjunctiva and muscles of the lower eyelid. A gentle massage of the anesthetic towards the retroseptal tissue is recommended. The upper eyelid is pulled to move the eyelashes and eyelid away from the surgical field. Afterwards, we invert the lower eyelid and digitally press the eyeball lightly until the orbital fat prolapses to the inferior cul de sac next to the conjunctiva.
We invert the upper eyelashes to avoid abrasion of the cornea when eye protectors for the laser are placed (Jaeger protector) at the lower cul de sac and over the eye to protect the eyeball. An assistant inverts the lower eyelid by turning the eyelid over the prolapsed fat. This leads to maximal protrusion of the lower orbital pad into the interior of the subconjunctival space (Fig. 1). With the CO2 laser adjusted to 6 W, in the continuous mode, with a 0.2 mm focus pointer, or comparable pulse mode, that is to say, 10 ml power, with 10 Watts, laser Ultrapulse Coherent, we make a transversal incision through the conjunctiva at the point of greatest protrusion of the pads or maximum bulging. Maximum bulging is 7 to 9 mm below the eyelid margin centrally, a distance 2 to 4 mm below the lower margin of the tarsi and, at least, 2 to 3 mm above the transverse plexus of visible subconjunctival vessels in the lower fornix (Fig. 2). During the incision, care must be taken so as not to damage the plexus. Depending on the position of the incision, access can be pre or retroseptal (11). If the parameters described above are followed, the orbital septum is kept intact and access is, therefore, retroseptal. The conjunctiva and the retractors of the lower eyelid are completely sectioned in 2 to 3 moves. Gentle pressure on the eye protector increases prolapse of the orbital fat of the nasal, medial and lateral pads (Fig. 3). The fat that emerges anteriorly to the orbital margin is folded over a matte Desmarres eyelid retractor, (in order not to reflect the laser), with a delicate mouse-tooth forceps. The fat is then sectioned using the eyelid retractor as base protector. By cutting the fat with the laser in a fairly unfocused fashion, we maximize hemostasis. Large vessels are avoided by direct visualization; an electric scalpel is used if necessary: The surgical wound is not sutured. The eye protector is removed and the lower eyelid is repositioned superiorly to check if any prolapsed pad has remained. Whenever excess residual pad is detected, we enter the incision to attempt to find and resection it. Once the bulging is adequately removed, we the eyelid is pulled up and repositioned superiorly. This restores normal anatomical relations and helps to prevent post-operative scarring ectropion.

Fig. 1 -Exposure of the conjunctival portion of the lower eyelid, viewing the vertical and horizontal vascular network.

Fig. 2 -Transconjunctival incision approximately 9 mm from the eyelash border, or at the proximal third of the conjunctival sac.

Fig. 3 -Exposure of eyelid pads after cutting the lower oblique muscle.
During this surgical stage, in most patients over 40 or with some degree of muscular flaccidity of lower eyelids, prophylactic or, frequently, therapeutic canthopexy is performed (Figs. 4 to 7)(12,13).

Fig. 4 -Drawing of the excess skin of the upper eyelid and lower eyelash incision to perform canthopexy.

Fig. 5 -Traction movement of the lower eyelid in order to measure lower eyelid flaccidity.

Fig. 6 -Traction of the lower eyelid after canthopexy suture and checking resistance.

Fig. 7 -Presence of fine wrinkles after lower transconjunctival blepharoplast and canthopexy.
In cases with deep-set eyes, or the presence of eyelid pads accompanied by inferior depression at the level of the lower orbital margin, we reposition the pads rather than remove them. The same transconjunctival access described above is used and by maneuvering the eyelid traction 90 degrees with a delicate double hook, we can observe the lower eyelid pads without cutting the orbital septum. This areolar tissue is detached up to the margin of the orbital margin, without cutting the periosteum, exposing the nasal and midface pads; these pads are resutured to the periosteum of the lower orbital margin to fill the depression at this level (Fig. 9). We call this method repositioning the lower lid pads, as described by Loeb(14) and Hamra(15). We have recently been using this method more than the simple resection of the excess pad because with the aging of facial structures, face fat tissue is progressively reduced. With this procedure we are able to keep the pads in the most adequate position.

Fig. 8 -Laser resurfacing of the lower eyelid along with total face laser.

Fig. 9 -Suture of lower lid pads around the lower orbit, medially.
When the malar pad needs to be elevated (SOOF = sub orbicular oculi fat)(15) with the elevation of the transconjunctival incision and continue the incision medium third of the face, we maintain the initial with the CO2 laser or with a regular scalpel, crossing the lateral eyelid angle or external corner laterally, and prolong it through the skin for more than 1 cm, cutting the skin, subcutaneous tissue and orbicular muscle until reaching the lateral orbital margin. We detach laterally and inferiorly a tunnel of roughly 5 to 6 cm, being careful not to damage the sensitive facial zygoin the supraperiostal plane and below the malar pad, zygomatic and infra-orbital nerve. Medially to the infra-orbital nerve, we cut the periosteum 0.5 cm below to the level of the nasal ala, respecting the infra-orbital nerve laterally. This maneuver provides us with the orbital margin and detach in the subperiostal plane an ample view of the whole eyelid flap that will be pulled superiorly and laterally, filling the depression of the medium third of the face. Non-absorbable sutures, such as prolene or nylon 5-0, are used beginasning medially towards the side, with various separate sutures.
The first sutures are between the deepest tissue medial to the periosteum, pulling and elevating the nasogenial groove with the maneuver. The most lateral suture is performed with one or two sutures joining the SOOF or malar fat to the periosteum of the lateral orbital margin at the desired height for an adequate elevation of the malar pad. Care must be taken not to pull too much, which would lead to bulging in the region. After reviewing hemostasia, we remove excess lateral skin carefully, without exaggerating, or we simply apply the laser to the surface of the eyelid skin. Then the intradermal suture of the skin is performed with nylon 6-0 and separate sutures at the level of the angle of the lateral corner of the eyelid, completely conserving local anatomy. There is no need to close the conjunctiva. If associated laser resurfacing is indicated, we do not resection the skin, since laser application to the eyelid skin will make it retract.
When the laser is not used to retract the skin, most authors indicate the possibility of immediate resection of excess skin after transconjunctival blepharoplasty or even late resection of this excess. Some authors indicate that 15% ofpatients need some skin resection, while others indicate that the resection is needed more frequently(16, 17, 18).
On the other hand, using laser to improve the final result, mainly in relation to fine wrinkles, is a powerful tool in the hands of a surgeon experienced in the technique, which is recommended whenever indicated (Figs. 10 to 15).

Figs. 10, 12 and 14 -Female, 56 year-old patient, skin phototype II of the Fitzpatrick classification, presenting Glogau Classification, type IV, wrinkles and upper and lower lid pads, with a depression at the level of the lower orbital margin.
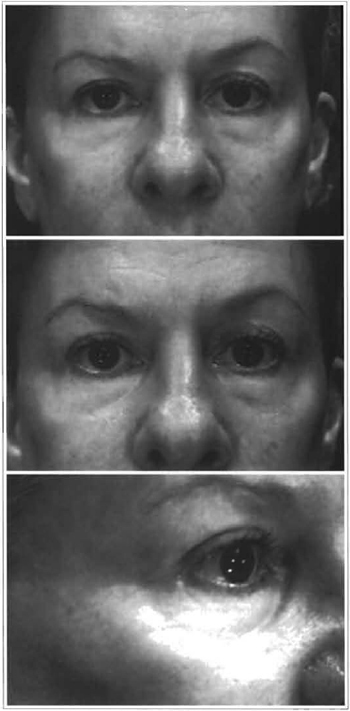
Figs. 11, 13 and 15 - 8-month post-operative follow-up after performing: upper blepharoplasty and removal of the skin and eyelid pads, transconjunctival lower lid blepharoplasty, repositioning medium and nasal pads over the lower orbital margin, rhytidoplasty and laser resurfacing of the whole face.
POST-OPERATIVE CARE
Post-operative care includes raising the head of the bed, using ice or cold pads with chamomile tea during the first 48 hours and using topical antibiotics during the day and a lubricating cream before bedtime. One should examine the patient on the first postoperative day to make sure that no retro-orbital hemorrhage, ectropion, (especially if laser was used on the skin surface) or loss of visual acuity has occurred.
COMPLICATIONS
In transconjunctival lower lid blepharoplasty, when only the eyelid pad is removed without removing skin excess, there are practically no complications. We can associate removal of excess skin to transconjunctival blepharoplasty without damaging muscular or tarsal structures and without having any complications(S). Among the complications of transconjunctival lower lid blepharoplasty that have been described are pyogenic granuloma, mainly when an attempt is made to close the incision with sutures(l9). However, whenever there is hematoma or prolonged edema, this lesion may also appear(20). Retraction of the eyelid has also been described as a complication and, although normally transitory, it lasts more than 4 weeks. Ecchymosis below the orbital margin is common and may take some days to resolve. Chemosis may occur and it is believed to be more of an allergic than surgical phenomena. The use of bupivacaine may also lead to transient diplopia due to the diffusion of the anesthetic in extrinsic muscles. Patients should be warned of this possibility (21, 22, 23, 24).
REFERENCES
1. BOURGUET J. Notre traitement chirurgical de "poches" sous les yeux sans cicatrice. Arch. Gr. Belg. Chir. 1928,31:133.
2. TESSIER P. The conjunctival approach to the orbital floor and maxilla in congenital malformation and trauma. J. Maxillofac. Surg. 1973;1:3.
3. ZAREM HA, RESNICK JI. Expanded applications for transconjunctival lower lid blepharoplasty. Plast. Reconstr. Surg. 1991;88(2):215-220.
4. TIPTON JB. Priority regarding transconjunctival blepharoplasty (letter, comment). Plast. Reconstr. Surg. 1992;89(4):765.
5. TRELLES MA, BAKER SS, TING J, et al. Carbon dioxide laser transconjunctival lower lid blepharoplasty complications. Ann. Plast. Surg. 1996;37(5):465-468.
6. ZAREM HA, RESNICK JI. Expanded applications for transconjunctival lower lid blepharoplasty. Plast. Reconstr. Surg. 1999;103(3):1041-1043.
7. ZAREM HA, RESNICK JI. Minimizing deformity in lower blepharoplasty. The transconjunctival approach. Clin. Plast. Surg. 1993;20(2):317-321.
8. PATIPA M. The evaluation and management of lower eyelid retraction following cosmetic surgery. Plast. Reconstr. Surg. 2000;106(2):438-453.
9. CARRAWAY JH. Transconjunctival blepharoplasty (letter). Plast. Reconstr. Surg. 1990;85(5):830.
10. YOUSIF NJ, SONDERMAN P, DZWIERZYNSKI WW, et al. Anatomic considerations in transconjunctival blepharoplasty. Plast. Reconstr. Surg. 1995;96(6):1271-1276.
11. ASKEN S. The preseptal and the retroseptal approaches in transconjunctival blepharoplasty. J. Dermatol. Surg. Oncol. 1992;18(12):1110-1116.
12. FLOWERS RS. Canthopexy as a routine blepharoplasty component. Clin. Plast. Surg. 1993;20(2):351-365.
13. LESSA S, SABASTIÁ R, FLORES E. A simple canthopexy. Rev. Soc. Bras. Cir. Plást. 1999;14(1):59-70.
14. LOEB R. Fat pad sliding and fat grafting for leveling lid depressions. Clin. Plast. Surg. 1981;8:757.
15. HAMRA ST. El papel de la preservación de la grasa orbitaria en cirugía estética facial - un nuevo concepto. Clin. Cir. Plast. 1996,23(1):19-29.
16. ELLENBOGEN R. Transconjunctival blepharoplasty (letter, comment). Plast. Reconstr. Surg. 1992;89(3):578.
17. JANUSZKIEWICZ JS, NAHAI F. Transconjunctival upper blepharoplasty. Plast. Reconstr. Surg. 1999;103(3):1015-1018.
18. OUSTERHOUT DK. Transconjunctival lower eyelid blepharoplasty (letter, comment). Plast. Reconstr. Surg. 1992;89(6):1176.
19. FRYER RH, REINKE KR. Pyogenic granuloma: a complication of transconjunctival incisions (letter). Plast. Reconstr. Surg. 2000;105(4):1565-1566.
20. HELTZER JM, ELLIS DS, STEWART WB, et al. Diffuse nodular eyelid lipogranuloma following sutureless transconjunctival blepharoplasty dressed with topical ointment. Ophtal. Plast. Reconstr. Surg. 1999;15(6):438-441.
21. TRELLES MA, GARCIA L. Complications in laser transconjunctival lower blepharoplasty (letter). Ann. Plast. Surg. 1997;39(1):105-106.
22. GHABRIAL R, LISMAN RD, KANE MA, et al. Diplopia following transconjunctival blepharoplasty. Plast. Reconstr. Surg. 1998;102(4):1219-1225.
23. MELE JA III, KULICK MI, LEE D. Laser blepharoplasty: Is it safe? Aesth. Plast. Surg. 1998;22(9):9-11.
24. ASKEN S. Transconjunctival lower lid blepharoplasty (letter, comment). Plast. Reconstr. Surg. 1992;89(4):764.
I - Senior Member of the Brazilian Society of Plastic Surgery and the Brazilian Society of Laser in Medicine and Surgery. Regional President for South-Brazil of the Brazilian Society of Laser in Medicine and Surgery. Visiting Professor at the Service of Plastic Surgery of the Curitiba Evangélico University Hospital.
II - Membro Titular da Sociedade Brasileira de Cirurgia Plástica e da Sociedade Brasileira de Laser em Medicina e Cirurgia. Member of the American Society for Laser in Medicine and Surgery.
III - Third Year Medical Resident in Plastic Surgery of the Plastic Surgery Service of the Curitiba Evangélico University Hospital.
IV - Medical student.
Address for correspondence:
Ruth Graf, MD
Rua Solimoes, 1184
80810-070 -Curitiba -PR Brazil
Phone: (5541) 335-7237 -Fax: (5541) 335-9394
e-mail: ruthgraf@bsi.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket