



Original Article - Year 2001 - Volume 16 -
Umbilical Restoration in Abdominoplasty: A Simple Rectangular Technique
Restauração Umbilical na Abdominoplastia: Uma Simples Técnica Retangular
ABSTRACT
The authors present a simple technique for umbilicus restoration in abdominal dermolipectomy. The procedure consists of a rectangular incision in the skin of the abdomen, slightly curved at the superior and inferior poles, after freeing the umbilicus with a circular incision in the abdominal tissue. The technique gives the umbilicus a natural, circular shape, obtaining a satisfactory result. Different drawings and pictures are shown to explain the skin procedure.
Keywords: Umbilicus; reconstruction; restoration; dermolipectomy; flap
RESUMO
Os autores apresentam uma técnica simples para a restauração do umbigo na dermolipectomia abdominal. Este procedimento está representado por uma incisão cutânea retangular, ligeiramente curvilínea nos pólos superior e inferior, feita na pele do abdome, após uma incisão circular no tecido abdominal liberando o umbigo. Esta técnica deixa o umbigo com uma forma natural, circular, apresentando um resultado satisfatório. Diferentes desenhos e figuras propõem-se a explicar o procedimento cutâneo.
Palavras-chave: Umbigo; reconstrução; restauração; dermolipectomia; retalho
The umbilicus has been described as a 1.5 to 2 cm diameter depressed scar, surrounded by a natural skin fold, anatomically situated at the level ofthe superior iliac crests (1,2). Many surgical procedures for reconstructing the umbilicus during dermolipectomy have been described.
Some authors have proposed using a different array of skin incisions to improve the shape of the umbilicus and disguise the periumbilical scar(l,3,4,5). Others defend using a conchal cartilage composite graft as the donating area to recreate the shape of the umbilicus(6).
Most of the existing procedures propose a circular skin incision of the umbilical cone to free it from its original position. The biological development of a circular scar eventually leads to retraction of the circular incision, and therefore to stenosis of the neo-umbilicus.
The authors propose a simple procedure that allows restoring the umbilical anatomy and hiding the scar that is buried around the umbilicus, leaving only its inferior margin visible.
SURGICAL TECHNIQUE
The first half of umbilicus restoration comprises a skin incision, to free the umbilicus from its original position. After marking the incision area, we position the index finger in the umbilical cavity and cut around the mark, freeing the umbilicus cone in a circular fashion (Fig. 1), measuring 1.5 cm in diameter.

Fig. 1 -After drawing a circle, the incision is performed around the index finger positioned in the umbilicus cavity to free the circular cone.
After removing the excess abdominal skin, the next phase is to reposition the neo-umbilicus. A fixation point with mononylon 3-0, 5 mm under the margin of the umbilicus is employed to put it at the aponeurosis of the linea alba. This suture allows the fixation of the umbilicus. A second suture inserts it at the xiphoumbilical line (Fig. 2).

Fig. 2 -We use mononylon 3-0, 5 mm fixation suture, under the umbilicus margin, at 6:00 and 12:00 o'clock.
After the guide sutures are placed to approximate the abdominal flap and the pubic area, we decide upon the position of the umbilicus on the abdominal skin. The position is marked 0.5 cm under the projected position of the umbilicus on the abdominal skin. This positioning reduces skin tension on the pubic incision.
A rectangle, slightly curved at the superior and inferior poles is drawn on the abdominal skin in the neoumbilical position (Figs. 3a & 3b). The A-B line should not exceed 2 cm, and the A-A' line should not exceed 0.5 cm. Subcutaneous fat is removed with a pair of scissors after the skin incision is made around the neo-umbilical position.
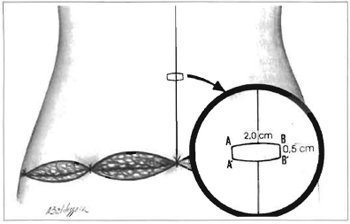
Fig. 3a -Drawing of the slightly curved rectangular marking at the superior and inferior poles over the abdominal wall skin.
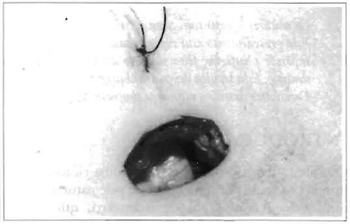
Fig. 3b -View of the umbilical cone after the rectangular incision through the abdominal wall.
POSTOPERAIVE PERIOD
A vaseline-saturated gauze dressing is kept over the entire umbilical area during the immediate postoperaive period. We tell the patient to change the dressing, using a mild topical corticoid and gauze to fill the umbilicus after bathing after the seventh day. After three weeks, we place a small sphere that is kept in place for 3 months to maintain the shape and compress the scar until it flattens.
COMPLICATIONS
In our series from February 1999 to February 2001, there were four complications, that were treated with dressings, and three hypertrophic scars treated with triamcinolone spray.
CONCLUSION
The umbilicus is a neonatal scar that remains invisible because it is hidden in the back of the cavity, and it is essential to the abdominal contour. It helps define the median abdominal sulcus, contributing to the proportionate curve of the inferior abdomen(7). Many techniques have been proposed to reposition the umbilicus(l,3,4). In the present study we present another easy way to perform the technique. This was used in 110 surgeries, from February 1999 to February 2001, all of which maintained the anatomical shape of the umbilicus and, due to its importance as a sexual focus(8), maintained its integrity in this respect (Figs.4-6).
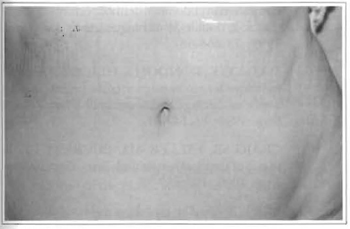
Fig. 4 -One year and 6 month postoperaive period, demonstrating the natural aspect of the umbilicus, with a practically unnoticeable scar.
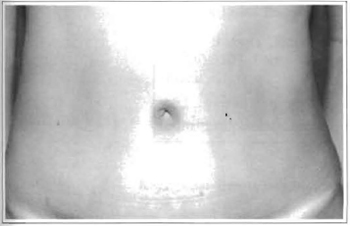
Fig. 5 -One year postoperaive period, with a hidden scar buried around the umbilicus.

Fig. 6 -Six-month postoperaive period showing a preserved anatomical shape.
REFERENCES
1. BAROUDI R. Umbilicoplasty. Clin. Plast. Surg. 1975; 2:431-48.
2. DUBOU R, OUSTERHOUT DK. Placement of the umbilicus in an abdominoplasty. Plast. Reconstr. Surg. 1978; 61 :291-3.
3. MASSIHA H, MONTEGUT W, PHILLIPS R. A method of reconstructing a natural looking umbilicus in abdominoplasty. Ann. Plast. Surg.1997; 38:228-31.
4. ITOH Y, ARAI K. Umbilical reconstruction usinga coneshaped flap. Ann. Plast. Surg. 1992; 28:335-8.
5. CANNISTRA G, PECORRELLI E. Umbilical restoration in abdominal dermolipectomy: a simple double-Y, double-M teclmique. Aesth. Plast. Surg. 1999; 23:364-66.
6. MATSUO K, KONDOH S, HIROSE T A simple teclmique for reconstruction ofthe umbilicus usinga conchal cartilage composite graft. Plast. Reconstr.Surg. 1990; 86:149-51.
7. CRAIG SB, FALLER MS, PUCKETT CL. Insearch of the ideal female umbilicus. Plast. Reconstr.Surg. 2000; 105:389-92.
8. BROWN ES. The umbilicus as sexual focus. Int.I Psychoanal. 1997; 78:577-8.
I - Candidate to the Brazilian Society of Plastic Surgery.
II - Full member of the Brazilian Society of Plastic Surgery, Head of the Plastic and Hand Surgery Service of Rio de Janeiro Santa Casa da Misericordia Hospital.
Address for correspondence:
Luis Lopez Tallaj, MD
R. Santa Luzia 206-11a Enf.
20020-020 -Rio de Janeiro -RJ Brazil
Phone: (55 21) 220-1778
e-mail: lopeztallaj@email.com
Study performed at the Plastic and Hand Surgery Service of Rio de Janeiro Santa Casa da Misericordia Hospital.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket