Clinical Entities
Lipodystrophy without sagging skin.
Skin flaccidity located in the axillary region without
lipodystrophy.
Localized skin flaccidity from the axillary region to the middle
third of the arm without lipodystrophy.
Localized skin flaccidity from the axillary region to the distal
third of the arm without lipodystrophy.
Lipodystrophy with sagging skin located in the axillary
region.
Lipodystrophy with localized skin flaccidity from the axillary
region to the middle third of the arm.
Lipodystrophy with localized skin flaccidity from the axillary
region to the distal third of the arm.
Considering each of the seven types of deformities described above, seven
corresponding surgical treatments can be established.
Type L arm - Liposuction
Type C1 arm - Axillary incision only
Type C2 arm - Axillary incision going to the middle third of the
arm
Type C3 arm - Axillary incision going to the medial
epicondyle
Type LC1 arm - Liposuction + Axillary only incision
Type LC2 arm - Liposuction + Axillary incision going to the
middle third of the arm
Type LC3 arm - Liposuction + Axillary incision going to the
medial epicondyle
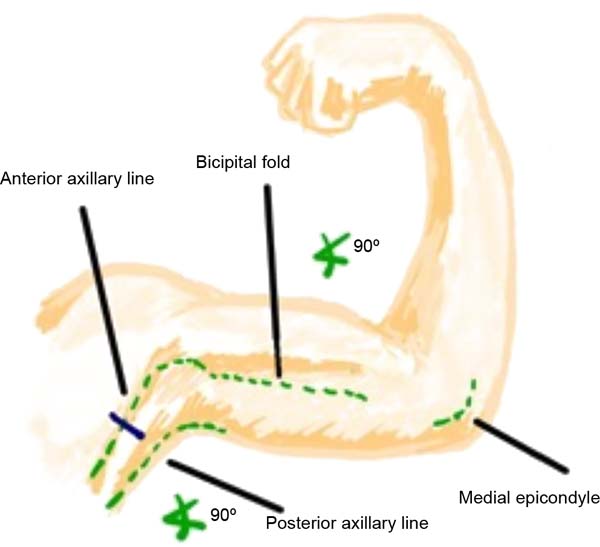
Skin demarcation for surgery should be performed with the patient in the
supine position, arm abducted at 90º, and forearm flexed at 90°
concerning the upper arm (Figure 1). The main anatomical points are identified: anterior and
posterior axillary folds, medial epicondyle, and medial bicipital
sulcus. Then, the marking begins based on the type of deformity the
patient presents according to the classification proposed here.
Figure 1 - Ideal arm position for skin demarcation.
Figure 1 - Ideal arm position for skin demarcation.
Cutaneous demarcation showing the spindle drawing determined by bidigital
clamping. Parallel lines guide cutaneous ears’ free closure (Figure 2).
Figure 2 - Markup example.
Figure 2 - Markup example.
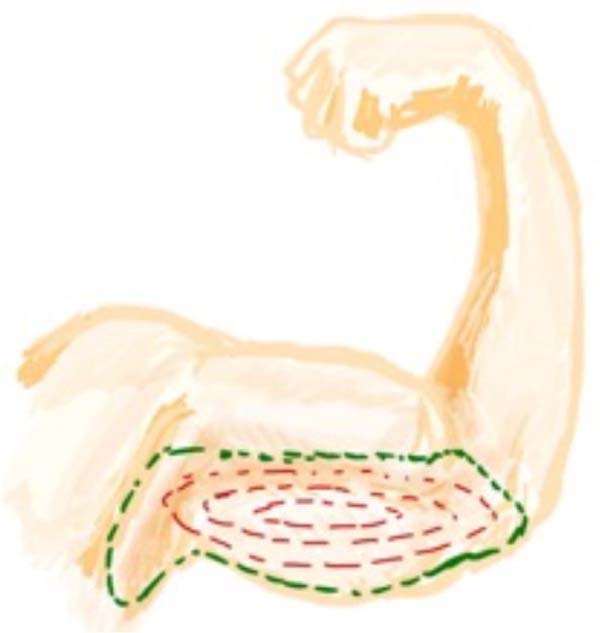
Type L arm: On physical examination, we found that in type L arm, there
is only lipodystrophy without flaccidity or excess skin. In this type of
arm, only liposuction is indicated. Cutaneous demarcation should be
performed only at the site to be liposuctioned using a classic
topographic technique, and in surgery, due care should be taken with
noble structures located deep in this region (Figure 3).
Figure 3 - Type L arm, only lipodystrophy is seen, without excess
skin.
Figure 3 - Type L arm, only lipodystrophy is seen, without excess
skin.
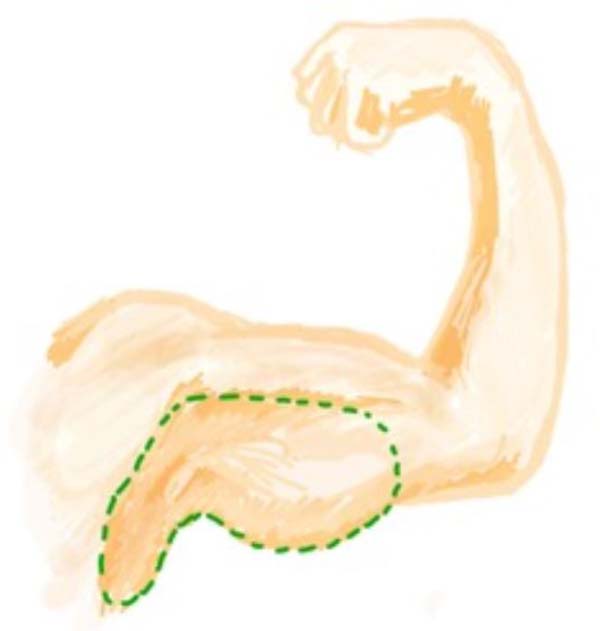
Type C1 arm: In this arm type, we see excess skin only close to the
armpit, without fat accumulation. The middle and distal thirds of the
arm are unchanged. In the type C1 arm, surgery to remove excess skin is
indicated only in the proximal region of the arm; therefore, the
demarcation of the incision must be made from the axillary fossa,
reaching the medial third of the arm at most, in a line that is located
1cm cranial to the bicipital sulcus (Figure 4).
Figure 4 - Type C1 arm presents only excess proximal skin without
lipodystrophy.
Figure 4 - Type C1 arm presents only excess proximal skin without
lipodystrophy.
Type C2 arm: This arm has excess skin extending from the armpit to the
middle third of the arm, without lipodystrophy. In type C2, surgery is
indicated to remove excess skin from the armpit extending to the middle
third of the arm, demarcating a line located 1 cm cranially to the
bicipital sulcus (Figure 5).
Figure 5 - Type C2 arm: excess skin from the armpit to the middle
third of the arm.
Figure 5 - Type C2 arm: excess skin from the armpit to the middle
third of the arm.
Type C3 arm: In this type of arm, a large excess of skin goes from the
armpit to the medial epicondyle without lipodystrophy; therefore, there
is no indication for liposuction. The incision is made in a line 1 cm
cranial to the bicipital sulcus, from the axillary crease to the end of
the deformity. The lower line is delimited by skin clamping encompassing
excess skin. As a result, a spindle is obtained from the crease of the
elbow, next to the medial epicondyle, extending to the axillary cavum
(Figure 6).
Figure 6 - Type C3 arm, excess skin from the axilla to the medial
epicondyle, without lipodystrophy.
Figure 6 - Type C3 arm, excess skin from the axilla to the medial
epicondyle, without lipodystrophy.
The following types are a combination of the types already described:
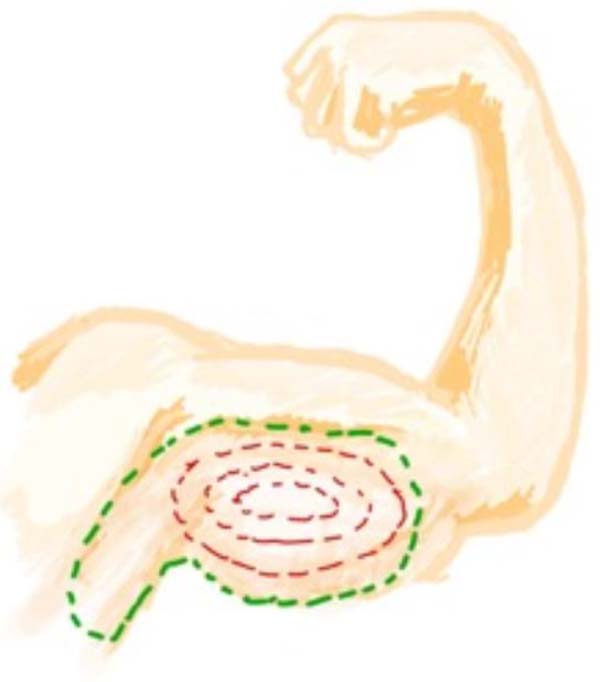
LC1: type C1 arm, with excess skin from the armpit to the proximal third
of the arm associated with lipodystrophy of the arm in any region.
Therefore, in this type of arm, surgery to remove excess skin is
indicated only in the proximal region of the arm, which goes from the
axillary cave to a maximum of the medial third of the arm, in a line
that is located 1cm cranial to the bicipital sulcus, associated with the
liposuction (Figure 7).
Figure 7 - Type LC1 arm, with excess proximal skin associated with
lipodystrophy.
Figure 7 - Type LC1 arm, with excess proximal skin associated with
lipodystrophy.
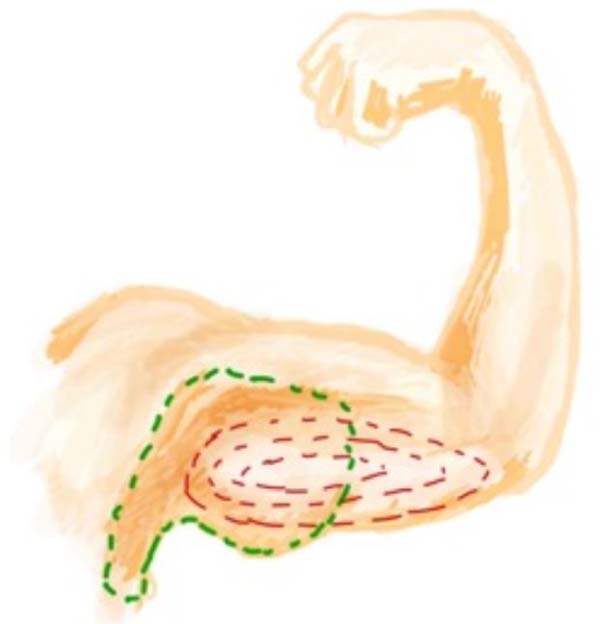
LC2: Arm with excess skin from the armpit to the middle third of the arm
associated with lipodystrophy. Skin resection is indicated from the
axillary pit to the middle third of the arm, respecting the limit of up
to 1 cm from the bicipital sulcus. Lipodystrophy is treated with
liposuction (Figure 8).
Figure 8 - Type LC2 arm: excess skin up to the middle third of the
arm associated with lipodystrophy.
Figure 8 - Type LC2 arm: excess skin up to the middle third of the
arm associated with lipodystrophy.
LC3: Indicates the arm with flaccidity and excess skin and associated
lipodystrophy. The resection will be taken up to the medial epicondyle.
Lipodystrophy will be treated with liposuction (Figure 9).
Figure 9 - Type LC3 arm with flaccidity: lipodystrophy up to the
distal region of the arm.
Figure 9 - Type LC3 arm with flaccidity: lipodystrophy up to the
distal region of the arm.