



Ideas and Innovation - Year 2023 - Volume 38 -
Brachioplasty in ex-obese patients: proposed classification
Braquioplastia no paciente ex-obeso: proposta de classificação
Rodrigo Pinto Gimenez1 ; Erick Samuel Santos de Mello1*; Raphaela Silveira Amaral1; Tatiani Cerioni Toth1
; Erick Samuel Santos de Mello1*; Raphaela Silveira Amaral1; Tatiani Cerioni Toth1
ABSTRACT
Introduction: Surgical treatment of morbid obesity has resulted in a greater demand for repairing procedures for sequelae caused by weight loss. Brachioplasty treats excess skin and localized lipodystrophy in the arm and armpit regions. Procedures for brachial deformity correction are incomplete and result in unsatisfactory scars. Therefore, we propose an objective classification that suggests surgical treatment intending to obtain an adequate brachial contour. The aim is to propose a classification to assess lipodystrophy and skin flaccidity in the arms and armpits in ex-obese patients and suggest adequate surgical treatment.
Method: Literature review and classification proposal that suggests a surgical treatment option based on the preoperative physical examination. This classification is objective and comprehensive, facilitating standardization among plastic surgeons.
Results: The LC classification is divided into 7 types. Type L - lipodystrophy without sagging; Type C1 - proximal flaccidity without lipodystrophy; Type C2 - sagging up to the middle third without lipodystrophy; Type C3 - flaccidity up to the distal third without lipodystrophy; Type LC1 - sagging in the proximal third with associated lipodystrophy; Type LC2 - sagging up to the middle third with lipodystrophy; Type LC3 - sagging up to the distal third with lipodystrophy. Based on the classification, those labeled "L" benefit from liposuction, while those labeled "C" suggest surgical dermolipectomy.
Conclusion: The classification aligns preexisting deformities with the respective surgical modality for correction in each case; therefore, an objective and practical classification facilitates communication and guides the best treatment, providing the patient with an adequate brachial contour.
Keywords: Reconstructive surgical procedures; Arm; Weight loss; Lipodystrophy; Lipectomy; Classification
RESUMO
Introdução: O tratamento cirúrgico da obesidade mórbida implicou na maior demanda por
procedimentos reparadores das sequelas causadas pela perda ponderal.
Braquioplastia trata o excesso de pele e lipodistrofia localizada nas
regiões dos braços e axilas. Os procedimentos para correção de deformidade
braquial são incompletos e resultam em cicatrizes insatisfatórias. Sendo
assim, propomos uma classificação objetiva que sugere tratamento cirúrgico
com vistas à obtenção de um contorno braquial adequado. O objetivo é propor
classificação para avaliar lipodistrofia e flacidez cutânea na região dos
braços e axilas no paciente ex-obeso e sugerir tratamento cirúrgico
adequado.
Método: Revisão da literatura e proposta de classificação que sugere opção de
tratamento cirúrgico a partir do exame físico pré-operatório. Tal
classificação é objetiva e abrangente, facilitando a padronização entre os
cirurgiões plásticos.
Resultados: A classificação LC se divide em 7 tipos. Tipo L - lipodistrofia sem flacidez;
Tipo C1 - flacidez proximal sem lipodistrofia; Tipo C2 - flacidez até terço
médio sem lipodistrofia; Tipo C3 - flacidez até terço distal sem
lipodistrofia; Tipo LC1 - flacidez em terço proximal com lipodistrofia
associada; Tipo LC2 - flacidez até terço médio com lipodistrofia; Tipo LC3 -
flacidez até terço distal com lipodistrofia. Baseado na classificação, as
denominadas "L" se beneficiam de lipoaspiração enquanto as denominadas "C"
sugerem dermolipectomia cirúrgica.
Conclusão: A classificação alinha deformidades preexistentes com a respectiva modalidade
cirúrgica para correção de cada caso, portanto, a existência de uma
classificação objetiva e prática facilita a comunicação e orienta o melhor
tratamento, proporcionando ao paciente um contorno braquial adequado.
Palavras-chave: Procedimentos cirúrgicos reconstrutivos; Braço; Perda de peso; Lipodistrofia; Lipectomia; Classificação
INTRODUCTION
The considerable increase in bariatric surgeries for the surgical treatment of morbid obesity has resulted in a greater demand for repairing procedures for sequelae caused by massive weight loss, such as abdominoplasty, mastopexy, and brachioplasty1-5. Brachioplasty treats excess skin and localized lipodystrophy in the arms and armpits to obtain an attractive brachial contour, graceful and discreet scarring, and fewer possible complications, such as dehiscence, infection and seroma, hypertrophic scarring, and contractures cicatricials3,4.
As most procedures for correcting post-weight loss brachial deformities are still incomplete and result in unsatisfactory scars4,6, there is a need to improve the surgical technique7 and standardize surgical procedures7-11. We created an intuitive classification that allows for better communication between surgeons, enabling the uniformity and standardization of assessing ex-obese patients with deformities in the arm and armpit region related to massive weight loss. Through this, we suggest the appropriate surgical treatment for each case to restore an adequate brachial contour. Prof. Ricardo Baroudi successfully adopted this standardization - Santa Casa de Campinas.
OBJECTIVE
Suggest a practical and useful classification for brachial deformities after severe weight loss, aiming to facilitate understanding and communication between plastic surgeons and jointly suggest possible specific management for each subtype.
MATERIAL AND METHOD
We performed a literature review, proposed an objective and practical classification encompassing all cases of brachial deformity found in our daily practice, and suggested the surgical treatment modality that could be applied to each subtype.
Currently, in the existing classifications, we find limitations, such as difficulty classifying and differentiating regions with lipodystrophy and/or skin laxity and using fixed values to determine ptosis, disregarding the patient’s body dimensions.
Considering that such classifications are unsatisfactory for standardizing an adequate surgical approach, we propose a classification that uses parameters easily assessed on physical examination and intuitively guides a treatment approach. Didactically, we divided such deformities into seven clinical entities, ranging from the simplest deformity with small lipodystrophy to the presence of cutaneous flaccidity along the entire length of the arm with the presence of lipodystrophy.
RESULTS
The proposed classification is based on evaluating the presence of lipodystrophy and cutaneous flaccidity in the region of the arms and armpits during the patient’s physical examination. After evaluating these parameters, it is possible to suggest appropriate surgical treatment for each case.
LC Classification
Clinical Entities
Lipodystrophy without sagging skin.
Skin flaccidity located in the axillary region without lipodystrophy.
Localized skin flaccidity from the axillary region to the middle third of the arm without lipodystrophy.
Localized skin flaccidity from the axillary region to the distal third of the arm without lipodystrophy.
Lipodystrophy with sagging skin located in the axillary region.
Lipodystrophy with localized skin flaccidity from the axillary region to the middle third of the arm.
Lipodystrophy with localized skin flaccidity from the axillary region to the distal third of the arm.
Considering each of the seven types of deformities described above, seven corresponding surgical treatments can be established.
Type L arm - Liposuction
Type C1 arm - Axillary incision only
Type C2 arm - Axillary incision going to the middle third of the arm
Type C3 arm - Axillary incision going to the medial epicondyle
Type LC1 arm - Liposuction + Axillary only incision
Type LC2 arm - Liposuction + Axillary incision going to the middle third of the arm
Type LC3 arm - Liposuction + Axillary incision going to the medial epicondyle
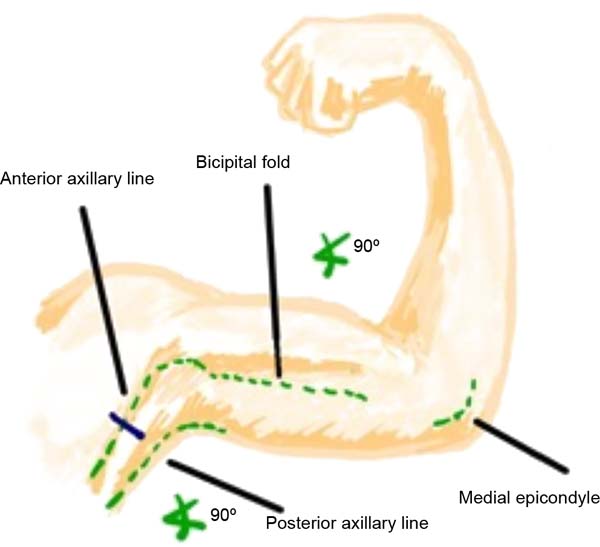
Skin demarcation for surgery should be performed with the patient in the supine position, arm abducted at 90º, and forearm flexed at 90° concerning the upper arm (Figure 1). The main anatomical points are identified: anterior and posterior axillary folds, medial epicondyle, and medial bicipital sulcus. Then, the marking begins based on the type of deformity the patient presents according to the classification proposed here.

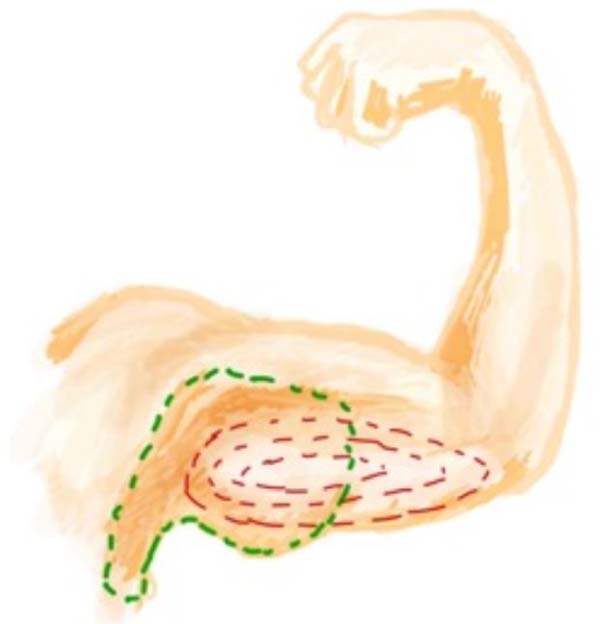
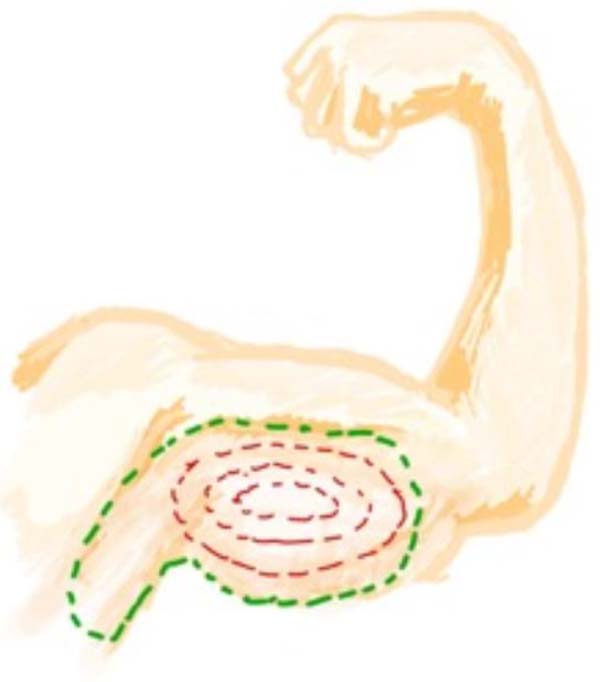
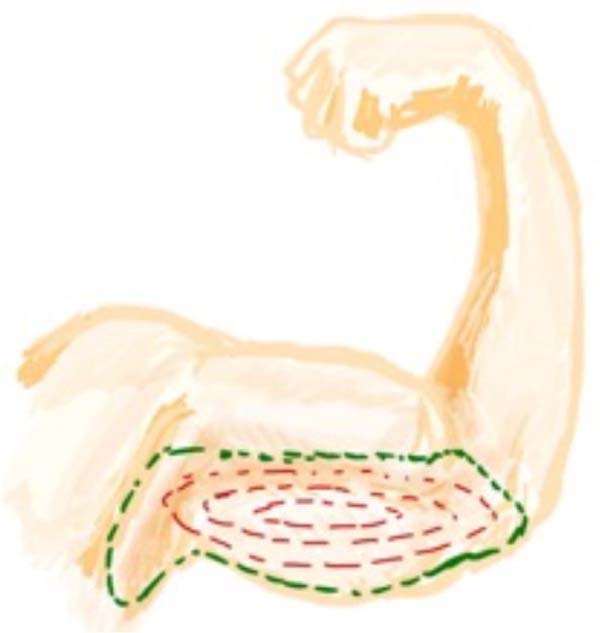
Cutaneous demarcation showing the spindle drawing determined by bidigital clamping. Parallel lines guide cutaneous ears’ free closure (Figure 2).


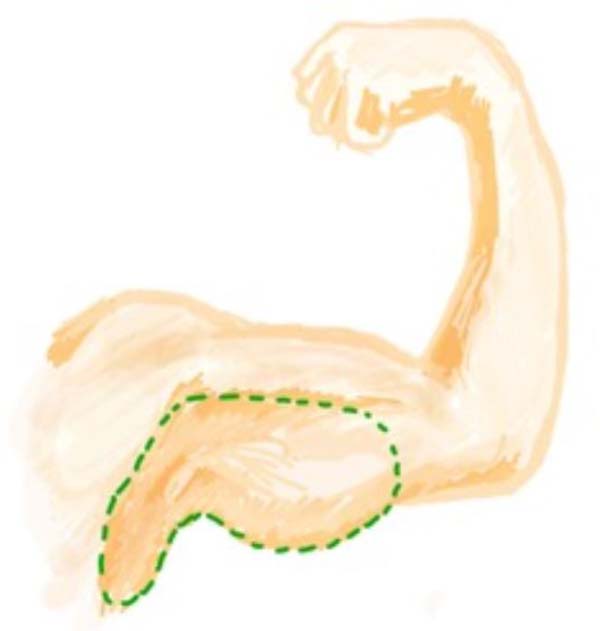
Type L arm: On physical examination, we found that in type L arm, there is only lipodystrophy without flaccidity or excess skin. In this type of arm, only liposuction is indicated. Cutaneous demarcation should be performed only at the site to be liposuctioned using a classic topographic technique, and in surgery, due care should be taken with noble structures located deep in this region (Figure 3).


Type C1 arm: In this arm type, we see excess skin only close to the armpit, without fat accumulation. The middle and distal thirds of the arm are unchanged. In the type C1 arm, surgery to remove excess skin is indicated only in the proximal region of the arm; therefore, the demarcation of the incision must be made from the axillary fossa, reaching the medial third of the arm at most, in a line that is located 1cm cranial to the bicipital sulcus (Figure 4).


Type C2 arm: This arm has excess skin extending from the armpit to the middle third of the arm, without lipodystrophy. In type C2, surgery is indicated to remove excess skin from the armpit extending to the middle third of the arm, demarcating a line located 1 cm cranially to the bicipital sulcus (Figure 5).

Type C3 arm: In this type of arm, a large excess of skin goes from the armpit to the medial epicondyle without lipodystrophy; therefore, there is no indication for liposuction. The incision is made in a line 1 cm cranial to the bicipital sulcus, from the axillary crease to the end of the deformity. The lower line is delimited by skin clamping encompassing excess skin. As a result, a spindle is obtained from the crease of the elbow, next to the medial epicondyle, extending to the axillary cavum (Figure 6).


The following types are a combination of the types already described:
LC1: type C1 arm, with excess skin from the armpit to the proximal third of the arm associated with lipodystrophy of the arm in any region. Therefore, in this type of arm, surgery to remove excess skin is indicated only in the proximal region of the arm, which goes from the axillary cave to a maximum of the medial third of the arm, in a line that is located 1cm cranial to the bicipital sulcus, associated with the liposuction (Figure 7).

LC2: Arm with excess skin from the armpit to the middle third of the arm associated with lipodystrophy. Skin resection is indicated from the axillary pit to the middle third of the arm, respecting the limit of up to 1 cm from the bicipital sulcus. Lipodystrophy is treated with liposuction (Figure 8).

LC3: Indicates the arm with flaccidity and excess skin and associated lipodystrophy. The resection will be taken up to the medial epicondyle. Lipodystrophy will be treated with liposuction (Figure 9).

DISCUSSION
The advent and popularity of liposuction expanded the range of options for improving body contour6,9,12, including concerning brachioplasty6. The proposed classification infers the modality of surgical treatment from the preoperative clinical evaluation, and this is objective, comprehensive, and practical for all cases of brachial deformity in ex-obese patients1,2,12. The classification proposal is the master plan for the knowledge of the types of existing deformities with the suggestion of surgical treatment necessary to correct each case. This classification highlights the main points to be observed in the surgical treatment of brachial deformity after severe weight loss, such as the need or not for liposuction,
The degree of deformity can be variable, and good surgical results should always take into account skin flaccidity and accumulation of subcutaneous tissue2,7.
Among the existing scales, we have Temouriam and Malekzadeh, Appelt, Pitsbourgh, and El Khatip; the latter is the most used. All scales use skin laxity and lipodystrophy as parameters, but the previous classifications do not consider the particularities of the patient’s body.
El Khatip uses fixed numbers as points of reference; these points are unlikely to be universally applicable. Our classification uses non-fixed measures; therefore, we believe it can be applied to all post-bariatric patients with some degree of lipodystrophy and/or skin flaccidity in the arms and armpits. Due to its practicality and objectivity allows easy interpretation by the plastic surgeon and reliable registration in medical records, articles, and literature, facilitating communication between professionals. Finally, our scale proposes a suggestion for surgical treatment to provide the patient with a harmonious arm contour and discreet scars (Table 1).
| El Khatip scale11 | ||
|---|---|---|
| Group | Skin and Fat | Treatment |
| I | Minimal fat (less than 300ml) without ptosis | Circumferential liposuction |
| IIa | Moderate fat and ptosis less than 5cm | Multi-stage liposuction |
| IIb | Severe fat with ptosis 5-10cm | Liposuction +/- skin excision axillary |
| III | Generalized obesity and skin laxity | Liposuction + brachioplasty with reduced scar |
| IV | Minimal fat deposits with grade 3 ptosis | Brachioplasty |
| LC scale | ||
| Arm Type | Skin and Fat | Treatment |
| L | Lipodystrophy without sagging | Liposuction |
| C1 | Axillary skin sagging Lipodystrophy | Axillary-only incision |
| C2 | Skin sagging in the axillary region up to the middle third of the arm without lipodystrophy | Axillary incision going to the middle third of the arm |
| C3 | Skin laxity up to the distal third without lipodystrophy | Axillary incision to the medial epicondyle |
| LC1 | Lipodystrophy with sagging skin in axillary region | Liposuction + incision only axillary |
| LC2 | Lipodystrophy with sagging skin up to the middle third of the arm | Liposuction + excision up to the middle third of the arm |
| LC3 | Lipodystrophy with skin flaccidity from the axillary region to the distal third of the Arm | Liposuction + axillary incision to the medial epicondyle |

CONCLUSION
The proposed scale offers a universal language for classifying alterations in the region of the arms and armpits in ex-obese patients based on the anatomical region where the lipodystrophy is located and the presence of concomitant skin flaccidity. Seven types of alterations were identified by evaluating such parameters, and based on these findings, the types of preexisting deformities are aligned with the respective surgical modality necessary for the correction of each case. An objective and practical classification facilitates communication between professionals and guides the best treatment, providing the patient with an attractive arm contour, graceful scar, and a lower rate of complications.
1. Santa Casa de Campinas, Serviço de Cirurgia
Plástica Ricardo Baroudi, Campinas, SP, Brazil
Corresponding author: Erick Samuel Santos de Mello Av. José Bonifácio, 2001, Jardim das Paineiras, Campinas, - SP, Brazil, Zip Code: 13092-305, E-mail: santos2224@gmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket