



Articles - Year 2000 - Volume 15 -
Advances in Profilemetric Study Applied to Facial Rejuvenescence
Avanços no Estudo Perfilométrico Aplicados ao Rejuvenescimento Facial
ABSTRACT
The anterior region of the neck is an area in which Plastic Surgery has been showing advances in aesthetic studies, with several surgical techniques and approaching ways for its performance. In spite of its great importance, the topographic study and outlining analyses of the cervical region have rarely deserved special attention. In this paper; the author presents a new focus in facial profilemetry. Upon radiological studies, points, angles and coordinates are outlined, which aids in the evaluation ofpatients with abnormalities at the submentonian, submandibular and anterior cervical requms, providing a new tool to successfully attain the profilemetry indicated. An abnormality degree classification in this region is also presented.
Keywords: Profilemetry; profileplasty; cervical-mentonian angle
RESUMO
A região anterior do pescoço é uma área em que a Cirurgia Plástica tem demonstrado avanços nos estudos estéticos, havendo várias técnicas cirúrgicas e formas de abordagem para a sua execução. Ainda assim, o estudo topográfico, análises da silhueta e contorno da região cervical raramente têm merecido uma atenção especial, apesar de sua grande importância. Neste trabalho, o autor apresenta um novo enfoque na perfilometria facial. Mediante estudos radiológicos, delimitam-se pontos, ângulos e coordenadas que são de grande ajuda na avaliação dos pacientes com alterações da região submentoniana, submandibular e cervical anterior, proporcionando uma nova ferramenta para alcançar, com êxito, a perfiloplastia indicada. É também apresentada uma classificação dos graus de alteração nessa região.
Palavras-chave: Perfilometria; perfiloplastia; ângulo cérvico-mentoniano
Beauty and harmony, size and balance of the contours: in order to have a clear idea of these concepts, it is quite important that the plastic surgeon be furnished with a good sense of proportion.
For centuries, the stereotypes of beauty for the human body have motivated several researchers. The interest for the aesthetic facial aspects goes back to the most ancient civilizations(1) - in all of them we may observe its importance, since the manifest in the beaus arts field (Figs. 1a, 1b, 1c, 1d and 1e). Leonardo Da Vinci(2) was the maximum exponent, and with his anatomical srudies and detailed sketches he provided conclusions, some of them accepted worldwide up to date (Figs 2a, 2b and 2c). Other researchers disagreed with the universal facial measures application(3), defending an individuality concept.

Fig. 1. (A, B, C, D, E) - Sculptures of different ages and civilizations are observed, in which the importance of me outline and profilemetric traces are appreciared.
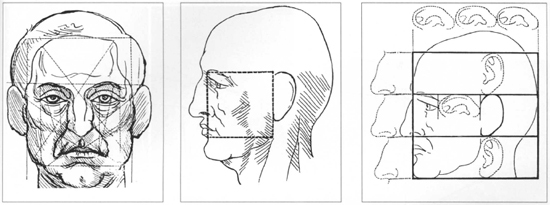
Fig. 2 - Drawings and traces made by Leonardo Da Vinci: A) Traces that relate, in a geometrical way, different facial structures. B)"Leonardo's square", which involves other anatomical points. C) Some facial profilemetry stereorypes.
The facial outline correction is a daily challenge for the plastic surgeon, and the treatment of submentonian, submandibular and anterior cervical regions, is a frequent procedure that is part of profileplasty arsenal(4,5).
Not only the plastic surgeon has the facial aesthetic as an objective. We may observe other specialties, such as Odontology and Maxilo-Facial Surgery(6), that are increasingly focusing their attention to the analysis and treatment of soft tissue areas in order to attain or complete the desired result. In several cases, we observe that the profileplasty aiming at the cervical region is the most simple and correct solution.
Despite being complex, cephalo-profilemetric studies (Figs. 3a, 3b and 3c) are quite important for the achievement of a definite diagnosis(7). The cervical region segment focused in this paper is subject to changes by various factors: age, weight increase, metabolic changes, etc. Anatomically, ir consists in well defined structures, in which the skin, fat tissue, superficial muscle aponeurotic system (SMAS) and platysma muscle stand out.

Fig. 3 - In this figure, we may observe the threesome of elements that comprise a cephalometric study to carry out a Profilemetry: A) Profile picture of a female patient; B) Lateral X-ray visualizing the facial outline. C) Points, planes and craniometrical lines identification.
Despite a number of papers on profileplasty at the cervical-facial region, the profilemetric study of the cervical region is probably the most overseen. Interventions such as ritidoplasty, liposuction, SMAS and platysma plication, etc, are the procedures most employed for this objective.
This subject is focused in the presem paper, gathering a set of new points and coordinates, aiming at providing a new tool for the evaluation and treatmcnt of this surgical regions, always darifying that the correct diagnosis and the most adequate intervention are directly related with surgeon's common sense(8).
PATIENTS AND METHOD
A total number of 40 patients, 20 females and 20 males, with ages between 16 and 28 years old (average 19 years old) was evaluated.
Patients were selected according to a cephalometric protocol based on studies of Zide(9), that determined the lack of craniofacial alterations and the presence of harmonious submentonian, submandibular and cervical regions(10). This study was carried out using the standard anthropometrical trace DOSP(11), lateral cranio-encephalic tele-X-rays made by a radiological Yoshida equipment, Pamoura 10-C, with the following specifications: mA= 10, Time=0.4-5.0 sec, kV=70-90.
SISTEMATICS
a) Anatomical drawing of cranio-encephalic tele-X-ray structures (Fig. 3c).
b) Points, planes and craniometrical lines (Fig. 4):

Fig. 4 - Determination of points, planes and craniometrical lines. S: Turcic saddle; N: Nasal; Po: Pogonian; Go: Gonian; M: Mento; Em: Articular prominence; Gnc: Cutaneous gnacio; Y: Growing axis (green tine); mandibular plane (red Line); Nasal- Pogonian line (blue line); Saddle-Nasal line; Frankfort plane.
1. Turcic Saddle Point (S).
2. Nasal Point (N).
3. Pogonian Point (Po).
4. Gonian Point (Go).
5. Mentonian Point (M).
6. Anterior Articular Prominence Point of the Glenoid Cavity (Em).
7. Mandibular plane trace (union of "Go" point with the lower tangential of mentonian symphysis "M").
8. Nasal-Pogonian trace (N-Po), up to the mandibular plane, which determines Gnacio point (Gn).
9. "Y" growing axis, which is the union of point "S" with point "Gn".
10. Cutaneous Gnacio point (Gnc), which is the projection of Gn point at the skin surface, following the growing "Y" axis.
11. Trace of the auxiliary line of the anterior articular prominence point, which is traced from "Em" up to "Go" point (Em-Go) (Fig. 5).
12. Trace of the perpendicular line of the mentonian point (M) to the auxiliary line (Em-Go). Line "A"(Fig. 5).
13. Trace of the Cervical-Mentonian line, which unites "Gnc" point with the most internal tangential point of the cervical outline. LINE "B" (Fig. 5).

Fig. 5 - Figure showing the obtaining of the cervical-mentonian angle, upon the intersection of lines A and B. We may also observe, in green, the auxiliary tine "Em Go", used to trace the perpendicular
to "M" point.*: Internal tangential point.
DETERMINATION OF THE CERVICAL MENTONIAN ANGLE ("DOUBLE CHIN")
Once the points are located and the lines and cephalometric planes are traced, we may proceed to the determination of the angle in focus. It is found at the intersection formed by lines A and B (Fig. 5).
We may highlight that during the performance of the present study other options to obtain line A and the measurement of the angle were analyzed. The mandibular plane was one of them. However, the angle result of the patients evaluated varied a lot, once it depended on the inclination degree of the mandible horizontal branch.
Other alternative considered for this line tracing was the hyoid bone line. This alternative was ruled out because this structure moves during deglutition.
RESULTS
40 cephalometric studies were analyzed so as to determine the cervical-mentonian angle. The results obtained and patient data are shown in table I.

The study has shown that there are no marked differences when we compare both female and male groups, the results of the evaluation were quite homogenous instead.
The lowest angle found in the female group was 5° and the highest was 19°, with an average of 13.6°. 6° to 18.5°, respectively, were the angles found in the male group, with an average of 13.1°.
When we analyze the group as a whole, we find an average of 13.3° of the cervical-mentonian angle.
The age of our group was not a determining factor for the angle's increase or reduction.
CLASSIFICATION OF THE CERVICAL-MENTONIAN ANGLE
A classification of the cervical-mentonian angle is pre presented bellow, based on the results obtained in the study (Figs. 6,7a1,7a2,7a3,7a4 and 7b).

Fig. 6 - Cephalometric study where we observe the overlaid trace of the four Cervical-mentonian angle levels. Degree I: up to 20°, Degree II:21°-40°, Degree III: 41°-60°, Degree IV: >60º.

Fig. 7 (A1, A2, A3, A4) - Graphic changes in a female patient where we sequentially observe the four cervical-mentonian angle levels. B: Schematic overlay of the four degrees.
DISCUSSION
Profilemetry, begun by Da Vinci, has been being ameliorated by other artists, who observed the need of studying humans proportions. It was noted that the perfection concept was not a convenience or something empirical being imposed; the curves and angles of a body were harmoniously detailed.
Currently, there is no information regarding the study of the cervical-mentonian angle, though there are techniques and tactics to repair it. The limit of beauty, in this anatomical set, has not had yet a scientific base. The performance of the present paper on the cervical-mentonian angle provides the plastic surgeon with the possibility to analyze the variations of this area, grouping patients in various degrees. This is important, specially nowadays, when legal-medical liability imposes us to perform more detailed studies.
The cephalometric orientation of normal cephalomentonian angle, with its different classification degrees, will aid in the technical choices and will provide inputs for a better surgical scheduling.
Considering this type of evaluation, the surgeon will have concrete arguments to indicate or not a double chin repair.
CONCLUSION
The harmony of a face depends on an adequate and proportional balance of the structures that comprises it. Doubtlessly, the region of the neck and its cervical- mentonian angle are essential and fundamental elements in its total evaluation (Fig. 8 al up to d2). This segment may suffer significant variations. In this work, we show a contribution to the Profilemetry, to perform Profileplasty, providing, after a series of studies, in addition to its classification, the ideal cervical-mentonian angle variation, which should not exceed 20°.

Fig. 8. Group of female patients where we observe examples of various cervical-mentonian angles. A1, A2) Degree 1: Patient presenting 18° of cervical-mentonian angle. B1, B2) Degree II: Patient presenting 36° of cervical-mentonian angle. C1, C2) Degree III: Patient presenting 47° of cervical-mentonian angle. Dl, D2) Degree IV: Patient presenting 63° of cervical mentonian angle.
REFERENCES
1. HAMBLETON RS. The soft tissue covering of the skeletal face as related to orthodontic problems. Amer. J. Orthodont. 1964;50(6):405-20.
2. McCARTHY JG. Introduction to Plastic Surgery. In MCCARTHY. Plastic Surgery. Vol. 1. Philadelphia : Saunders, 1990. p. 28-36.
2. ANGLE EH. Malocclusion of the teeth. 7th Edition. Philadelphia. SS White Dental Manufacturing Co. 1907.
3. ZANINI SA, SOUZA AM. Perfiloplastias. In: MÉLEGA, ZANINI, PSILLAKIS: Cirurgia Plástica - Reparadora e Estética. São Paulo : Medsi, 1992. p. 621-6.
4. PSILLAKIS JM. Perfiloplastias. Anais do XIII Congresso Brasileiro de Cirurgia Plástica. 1984.
5. SERAPHIM L. O perfil mole e sua importância como indicador das deformidades dentofaciais. São Paulo - Faculdade de Saúde Pública, 1973 (Trabalho de mestrado).
6. ZIDE B, GRAYSON B, McCARTHY JG. Cephalometric analysis: Part I. Plast. Reconstr. Surg.1981;68:816.
7. SPIRA M. Malformaciones de la mandíbula y alteraciones de la articulación temporomandibular. In Grabb-Smith:Cirugía Plástica.Barcelona : Salvat, 1984.p.159-187.
8. SPERLI AE. Perfil facial - Avaliação estética. In: ANAIS DO XIII CONGRESSO BRASILEIRO DE CIRURGÍA PLÁSTICA,1984.
9. ZIDE B, GRAYSON B, McCARTHY JG. Cephalometric analysis for upper and lower midface Surgery:Part II. Plast. Reconstr. Surg.1981;68:961.
10. DE PAIVA LA. Ortodontia Preventiva Básica. São Paulo : Artes Médicas,1994. p.142-59.
I - Resident of the Integrated Plastic Surgery Services - MEC/SBCP - Hospital Ipiranga - São Paulo - Brazil.
II - Headmaster of the Integrated Plastic Surgery Services - MEC/SBCP - Hospital Ipiranga São Paulo - Brazil.
III - Teaching Coordinator of the Integrated Plastic Surgery Services - MEC/SBCP Hospital Ipiranga - São Paulo- Brazil.
IV - Head Professor of Orthodontics of Universidade Camilo Castelo Branco.
Address for correspondence:
Diomar Flores, MD
Av.Cidade Jardim, 993
01453-000 - São Paulo - SP Brazil
Phone: (55 11) 3845-1279
e-mail: sperli@imedical.com
Work performed at Serviços Integrados de Cirurgia Plástica - Official postgraduate course, MEC-SBCP, Hospital Ipiranga - São Paulo.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket