



Original Article - Year 2018 - Volume 33 -
Breast reconstruction after prophylactic contralateral mastectomy
Reconstrução mamária após mastectomia contralateral profilática
ABSTRACT
Introduction: Prophylactic contralateral mastectomy (PCM)
has been increasingly indicated in recent years for patients
outside of the high-risk group, although its cancer benefit
in terms of survival remains controversial. The possibility
of breast reconstruction is one of the most important factors
for this indication. The objective of this study was to evaluate
the indications and complications after immediate breast
reconstruction in patients who underwent PCM.
Method:
Indications and complications were evaluated in patients who
underwent immediate breast reconstruction after therapeutic
mastectomy and PCM.
Results: Of the 13 patients in the study,
only 4 had a high-risk indication for PCM (strong family history).
The other indications were desire for symmetry, control of
anxiety related to neoplasm recurrence, and age-related
risk. Only minor complications occurred, without a need for
reoperation, in 4 of the 13 patients (30.76%). Eight complications
(30.76%) in 26 reconstructed breasts were recorded.
Conclusion:
The number of PCM procedures has been increasing and the
indications transcend the oncological point of view, directly
influencing the performance of plastic surgeons with respect
to the planning and complications of breast reconstruction.
Keywords: Subcutaneous mastectomy; Breast implant; Breast neoplasms; Postoperative complications; Risk factors; Mammoplasty
RESUMO
Introdução: A indicação da mastectomia contralateral profilática (MCP) tem aumentado nos
últimos anos nas pacientes fora do grupo de alto risco, apesar de seu
benefício oncológico controverso em relação à sobrevida. A possibilidade da
reconstrução mamária é um dos fatores mais importantes desse aumento. O
objetivo é avaliar pacientes submetidas à MCP quanto às indicações e
complicações após a reconstrução imediata.
Método: Avaliação das pacientes submetidas à reconstrução mamária imediata após
mastectomia terapêutica e MCP quanto às indicações e complicações.
Resultados: Das 13 pacientes do estudo, apenas 4 apresentavam indicação de MCP por alto
risco (forte história familiar). As outras indicações foram busca pela
simetria, controle da ansiedade em relação à nova neoplasia e risco
acumulado pela idade. Ocorreram apenas complicações menores, sem necessidade
de reoperação em 4 das 13 pacientes (30,76%) e num total de 26 mamas
reconstruídas foram registradas 8 complicações (30,76%).
Conclusão: A realização da MCP tem aumentado, sendo que as indicações transcendem o
ponto de vista oncológico, com impacto direto na atuação do cirurgião
plástico quanto aos aspectos que envolvem a reconstrução, tanto no
planejamento quanto suas complicações.
Palavras-chave: Mastectomia subcutânea; Implante mamário; Neoplasias da mama; Complicações pós-operatórias; Fatores de risco; Mamoplastia
INTRODUCTION
Prophylactic contralateral mastectomy (PCM) is intended to reduce the risk of contralateral breast cancer in selected patients with unilateral breast cancer. According to the consensus of the American Society of Breast Surgeons, high-risk patients indicated for PCM are those with the following characteristics1:
Positive genetic test for BRCA1 and BRCA2 gene mutations;
Strong family history (first-degree relatives);
History of thoracic irradiation before 30 years of age.
Recent studies have shown that the probability of developing contralateral cancer among patients with unilateral breast cancer who do not fall into the high-risk category ranges from 0.2% to 0.75% per year. In some series, the probability reaches up to 6.5% in 15 years. The survival benefit of PCM in these patients is highly controversial2-4.
However, in recent years, there has been a large increase in the indication for PCM in this group. Increases in indications of up to 300% were reported by reference institutions based on the Surveillance, Epidemiology, and End Results program3-5.
Despite advances in adjuvant therapies allowing conservative breast cancer surgeries, many breast surgeons and patients have opted for therapeutic mastectomy associated with PCM, despite the absence of a cancer benefit1,6.
One of the most important factors for this choice is the possibility of immediate breast reconstruction coupled with the overestimated fear of cancer in the contralateral breast. Aesthetic desire and symmetry are also important factors1,4-8.
Bilateral reconstruction does provide a favorable aesthetic result. Although higher satisfaction rates have been reported, few long-term studies have compared bilateral reconstruction with symmetrization after conservative surgeries and unilateral therapeutic mastectomy1,4,7,9,10.
A possible disadvantage of PCM as a preventive treatment is its high cost for patients. As most patients choose mastectomy and bilateral reconstruction, greater morbidity results from these techniques3,11.
OBJECTIVE
The objective of this study was to evaluate the indications and complications after immediate reconstruction in patients who underwent PCM.
METHOD
From a retrospective analysis of medical records, 38 patients who underwent breast reconstruction for cancer, performed by the author in his private practice in Florianópolis, Santa Catarina, from November 2015 to February 2017, were selected. Patients who underwent late mammary reconstruction and those who underwent immediate, bilateral breast reconstruction after PCM concomitantly with therapeutic mastectomy met the inclusion criteria. A total of 13 patients were included (Table 1).
| Patient | Age (y) | Indications |
|---|---|---|
| 1 | 45 | Anxiety related to neoplasm recurrence |
| 2 | 66 | Symmetry |
| 3 | 33 | Strong family history (sister with a positive genetic test) and age-related risk |
| 4 | 33 | Symmetry, anxiety related to neoplasm recurrence, and age-related risk |
| 5 | 37 | Symmetry and age-related risk |
| 6 | 58 | Anxiety related to neoplasm recurrence |
| 7 | 47 | Strong family history of breast cancer and symmetry |
| 8 | 32 | Symmetry and age-related risk |
| 9 | 52 | Symmetry and anxiety related to neoplasm recurrence |
| 10 | 55 | Lobular neoplasia and anxiety related to neoplasm recurrence |
| 11 | 31 | Symmetry and age-related risk |
| 12 | 43 | Strong family history and anxiety related to neoplasm recurrence |
| 13 | 48 | Strong family history |

The indication for therapeutic mastectomy with or without nipple-areolar complex (NAC) sparing was defined by the breast surgeons according to the clinical and pathological criteria of each patient. PCM with and without NAC sparing was also indicated according to oncological criteria and discussion with the patient. None of the patients underwent a genetic test before surgery.
All patients were properly instructed and signed the informed consent form authorizing the responsible and confidential use of their medical records.
RESULTS
The mean follow-up time of patients who underwent bilateral mastectomy with immediate breast reconstruction was 6 months and 18 days. The patient age ranged from 32 to 66 years (mean age, 44 years and 7 months), and the mean body mass index was 23.52 kg/m2. The NAC was spared in the breast with cancer in 4 patients. The NAC of the contralateral breast was spared in 7 patients, whereas the other 6 patients who were seeking breast symmetry opted for contralateral NAC excision.
For breast reconstruction, breast prosthesis was used in 9 patients and temporary expander was used in 4 patients. Autologous reconstructions were not performed in this group.
The length of hospital stay of all patients was up to 24 h.
Among the patients, only 4 had a high-risk indication for PCM (strong family history of breast cancer). The other reasons for PCM discussed with the patients included anxiety and fear of neoplasm in the contralateral breast in 6 patients, age-related risk in 5 patients, and desire to undergo PCM for symmetry in 7 patients (Figures 1 and 2).
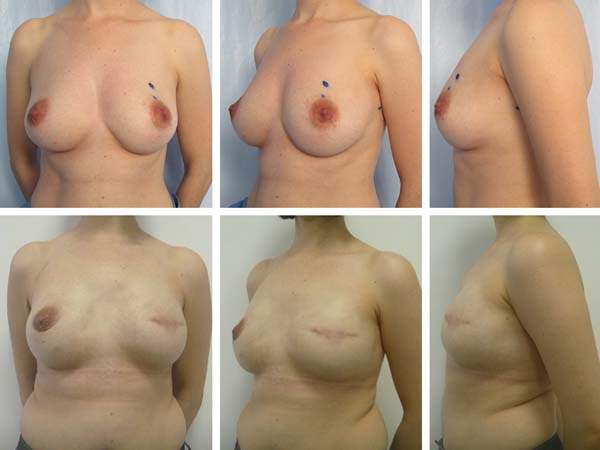



There were no major complications that required reoperation. There was 1 case of cellulitis that required treatment with antibiotics, and this same patient had partial necrosis of the NAC both in the breast with cancer and in the contralateral breast. One patient required drainage of hematoma in the ipsilateral breast 8 days postoperatively and developed a small seroma after 20 days, which was properly aspirated.
Moreover, partial necrosis of the NAC was observed in 1 patient and partial necrosis of the contralateral NAC was observed in 2 other patients (Figure 3).


Therefore, we observed only minor complications without a need for reoperation in 4 of the 13 patients (30.76%). A total of 8 complications in 26 reconstructed breasts (30.76%) were recorded.
DISCUSSION
In recent years, there has been an increase in reconstructive surgeries after unilateral mastectomy, bilateral mastectomy, and PCM compared with therapeutic mastectomy. An almost 4-fold increase in the rate of PCM was observed in extensive reviews of data from the National Cancer Institute and National Cancer Database2,5.
A decline in the rate of conservative surgeries was also observed, but without a corresponding increase in unilateral mastectomy as expected. In our practice, 61% of breast reconstructions were bilateral and immediate, which is similar to the rate in the literature. That is, patients eligible for conservative surgery are increasingly opting for bilateral mastectomy rather than unilateral mastectomy or conservative surgery2,5.
The analysis of the epidemiological profile in the literature shows that patients are increasingly younger and of a high socioeconomic level6,9,12. According to Sabel et al.6, age is a highly significant predictor of not only an indication for mastectomy but also of the PCM option (p < 0.0001)6. This is especially true for women younger than 40 years, as two-thirds of them opt for therapeutic surgery and PCM5,6.
All of our patients underwent breast reconstruction with a prosthesis or expander, which is undoubtedly the prevailing method in most services (71-96%)6,9,11,12.
Discussions with patients reveal that factors such as fear of developing contralateral breast disease, fear of maintaining frequent imaging follow-up, and even influence of media (such as the “Angelina Jolie effect”) highly affect their decision6, whereas some patients overestimate the risk of the procedure or misinterpret the benefit of bilateral mastectomy versus conservative surgery4-6.
Among our group of patients, only 4 (30%) were indicated for PCM owing to a high risk for contralateral disease (strong family history); however, all of them reported 1 or more reasons (symmetry, anxiety, age-related risk) for their decision to choose PCM. Studies suggest that, currently, 60-70% of PCMs are performed in patients without high-risk indications. There is a consensus that the indication for PCM has increased despite its lack of cancer benefit, which constitutes a “cancer paradox”1,2,5,6,9-11.
The consensus of the American College of Surgeons suggests that PCM should be discouraged in patients who are not at a high risk for contralateral breast disease, but that it can be considered when there is difficulty in the follow-up of the contralateral breast, when the patient desires symmetry, and for the management of extreme anxiety1. The patient’s objective, preferences, and values should be included in the discussion with both the breast surgeon and the plastic surgeon4,8,10.
Few detailed studies have compared the incidence of all major and minor reconstructive complications after PCM. When major complications (requiring reoperations and/or prolonged admissions) and mortality rate were analyzed, immediate bilateral breast reconstruction had a higher incidence than mastectomies without breast reconstruction, unilateral mastectomy, and conservative surgeries9,11-13.
Miller et al.11 evaluated 600 patients and found a complication rate of 26.8% in unilateral mastectomy and 41.6% in PCM. Among the most frequent complications in PCM are cellulitis/infection requiring antibiotic treatment (21.1%), expander or implant loss (17.3%), and difficult healing/partial necrosis (15.1%). In our series, the most frequent complications were partial necrosis of the contralateral NAC (23.08%) and partial necrosis of the ipsilateral NAC (15.38%).
Many studies in the literature do not specify the occurrence of NAC necrosis. In older reviews, mastectomies were performed without sparing the NAC and sometimes the skin. Thus, it is difficult to establish, based on the literature, a reliable rate for this complication after breast reconstruction in simultaneous PCM and therapeutic mastectomy.
Obviously, the risk of complications is greater in mammary reconstruction after bilateral mastectomy than in unilateral mastectomy. However, the indications for the procedure, including risk of contralateral cancer, difficult follow-up, desire for symmetry, and reduction of anxiety, should be evaluated11-13.
The literature has shown significant short-term benefits in terms of quality of life, although there is no evidence of increased survival for patients without mutations5,7,9. Spear et al.7 demonstrated in 2008 that practically all patients who underwent reconstructive surgery after prophylactic mastectomy declared that they would undergo the procedure again.
Boughey et al.9 also reported that in the long term (10 and 20 years), 84% of patients would undergo PCM again. They also observed a high satisfaction rate among patients who underwent only PCM, those who underwent breast reconstruction, and even those who had complications requiring reoperations. Reconstruction is associated with increased self-esteem, femininity, and body acceptance9,10.
Other authors reported that the most frequent complaints and dissatisfactions (21-33%) of patients who underwent bilateral reconstruction are related to worse-than-expected complications, aesthetic result, and number of unexpected procedures2,10,11.
However, the question remains whether a healthy breast should be put at risk to aim for symmetry without a cancer benefit.
It is known that breast reconstruction, especially when done with prostheses, is not an innocuous procedure in the long term. The possibility of contracture, chronic pain, muscular atrophy, and need for frequent fat grafting do not have the same impact of cancer but may require even more interventions and investment than conservative surgery. Nearly 40% of patients require 1 or more unplanned surgeries, which is the main cause of dissatisfaction with bilateral reconstruction2,3,5,6.
With regard to breast reconstruction, the pursuit of aesthetic excellence was addressed by Spear14 in a recently published editorial, titled “We became hostages of our success.” The possibility of breast reconstruction is one of the most important factors in the decision to undergo PCM4,5,9. A high-quality orientation must be aligned to realistic decisions and expectations2.
The plastic surgeon is responsible for informing the patient of the advantages and disadvantages, such as complication rates ranging from 7% to 60%2,11; the limitations of aesthetic and symmetry results requiring multiple procedures throughout life; and the risk of operating the healthy breast, when the patient may be overestimating the risk of a new disease.
More long-term comparative studies on satisfaction, quality of life, costs, reoperations, and refinements comparing ipsilateral reconstruction and symmetrization (when necessary) after conservative surgery, unilateral mastectomy, and reconstruction after bilateral mastectomy (therapy and PCM) are needed.
CONCLUSIONS
The number of PCM procedures has been increasing, and the indications transcend the oncological point of view, directly influencing the performance of plastic surgeons with respect to the planning and complications of breast reconstruction.
REFERENCES
1. Boughey JC, Attai DJ, Chen SL, Cody HS, Dietz JR, Feldman SM, et al. Contralateral Prophylactic Mastectomy (CPM) Consensus Statement from the American Society of Breast Surgeons: Data on CPM Outcomes and Risks. Ann Surg Oncol. 2016;23(10):3100-5. DOI: http://dx.doi.org/10.1245/s10434-016-5443-5
2. Albornoz CR, Matros E, Lee CN, Hudis CA, Pusic AL, Elkin E, et al. Bilateral mastectomy versus breast-conserving surgery for early-stage breast cancer: the role of breast reconstruction. Plast Reconstr Surg. 2015;135(6):1518-26. DOI: http://dx.doi.org/10.1097/PRS.0000000000001276
3. Davies KR, Cantor SB, Brewster AM. Better contralateral breast cancer risk estimation and alternative options to contralateral prophylactic mastectomy. Int J Womens Health. 2015;7:181-7.
4. Agarwal S, Kidwell KM, Kraft CT, Kozlow JH, Sabel MS, Chung KC, et al. Defining the relationship between patient decisions to undergo breast reconstruction and contralateral prophylactic mastectomy. Plast Reconstr Surg. 2015;135(3):661-70. DOI: http://dx.doi.org/10.1097/PRS.0000000000001044
5. Wong SM, Freedman RA, Sagara Y, Aydogan F, Barry WT, Golshan M. Growing Use of Contralateral Prophylactic Mastectomy Despite no Improvement in Long-term Survival for Invasive Breast Cancer. Ann Surg. 2017;265(3):581-9. DOI: http://dx.doi.org/10.1097/SLA.0000000000001698
6. Sabel MS, Kraft CT, Griffith KA, Bensenhaver JM, Newman LA, Hawley ST, et al. Differences between Breast Conservation-Eligible Patients and Unilateral Mastectomy Patients in Choosing Contralateral Prophylactic Mastectomies. Breast J. 2016;22(6):607-15. DOI: http://dx.doi.org/10.1111/tbj.12648
7. Spear SL, Schwarz KA, Venturi ML, Barbosa T, Al-Attar A. Prophylactic mastectomy and reconstruction: clinical outcomes and patient satisfaction. Plast Reconstr Surg. 2008;122(1):1- 9. DOI: http://dx.doi.org/10.1097/PRS.0b013e318177415e
8. Chagpar AB. Prophylactic bilateral mastectomy and contralateral prophylactic mastectomy. Surg Oncol Clin N Am. 2014;23(3):423-30. DOI: http://dx.doi.org/10.1016/j.soc.2014.03.008
9. Boughey JC, Hoskin TL, Hartmann LC, Johnson JL, Jacobson SR, Degnim AC, et al. Impact of reconstruction and reoperation on long-term patient-reported satisfaction after contralateral prophylactic mastectomy. Ann Surg Oncol. 2015;22(2):401-8. DOI: http://dx.doi.org/10.1245/s10434-014-4053-3
10. Anderson C, Islam JY, Elizabeth Hodgson M, Sabatino SA, Rodriguez JL, Lee CN, et al. Long-Term Satisfaction and Body Image After Contralateral Prophylactic Mastectomy. Ann Surg Oncol. 2017;24(6):1499-506. DOI: http://dx.doi.org/10.1245/s10434-016-5753-7
11. Miller ME, Czechura T, Martz B, Hall ME, Pesce C, Jaskowiak N, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113-20. DOI: http://dx.doi.org/10.1245/s10434-013-3108-1
12. Silva AK, Lapin B, Yao KA, Song DH, Sisco M. The Effect of Contralateral Prophylactic Mastectomy on Perioperative Complications in Women Undergoing Immediate Breast Reconstruction: A NSQIP Analysis. Ann Surg Oncol. 2015;22(11):3474-80. DOI: http://dx.doi.org/10.1245/s10434-015-4628-7
13. Osman F, Saleh F, Jackson TD, Corrigan MA, Cil T. Increased postoperative complications in bilateral mastectomy patients compared to unilateral mastectomy: an analysis of the NSQIP database. Ann Surg Oncol. 2013;20(10):3212-7. DOI: http://dx.doi.org/10.1245/s10434-013-3116-1
14. Spear SL. Underpromise. Plast Reconstr Surg. 2016;137(6):1961-2. PMID: 27219249 DOI: http://dx.doi.org/10.1097/PRS.0000000000002145
1. Serviço de Cirurgia Plastica, Hospital de
Caridade, Florianópolis, SC, Brazil.
2. Sociedade Brasileira de Cirurgia Plástica, São
Paulo, SP, Brazil.
Corresponding author: Raidel Deucher Ribeiro, Av. Osvaldo Rodrigues Cabral, 1570, sala 208, Centro - Florianópolis, SC, Brazil. Zip Code 88015-710. E-mail: dr. raidel@gmail.com
Article received: March 6, 2017.
Article accepted: May 9, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket