ISSN Online: 2177-1235 | ISSN Print: 1983-5175
Correction of low or saddle nasal dorsum with a composite graft of fragmented conchal cartilage fixed to the perichondrium wrapped in mastoid fascia
Correção do dorso nasal baixo ou em sela com enxerto composto de cartilagem conchal fragmentada fixa ao pericôndrio envolvidos à fáscia da mastóide
ABSTRACT
INTRODUCTION: In many cases, augmentation rhinoplasty is more difficult than reduction rhinoplasty. Solid dorsal grafts performed with costal cartilage have been widely used for dorsal augmentation; however, they are associated with high rates of revision. Thus, many authors began to use cartilage cut into cubes wrapped in fascia. The mastoid fascia, connected to the perichondrium of the auricular conchal cartilage can form a composite graft to augment the nasal dorsum, which is also a treatment option. The objective is to demonstrate the possibility of using fragmented auricular conchal cartilage fixed to its perichondrium and wrapped in mastoid fascia to form a composite graft for augmentation of the nasal dorsum.
METHODS: This is a retrospective study of 9 patients who underwent operation between 2012 and 2016 at the Base Hospital of the Faculty of Medicine of São José do Rio Preto, in which the nasal dorsum was augmented with fragmented conchal cartilage fixed to its perichondrium and wrapped in the mastoid fascia.
RESULTS: The patients were followed up for up 6 to 48 months. They were questioned about their satisfaction with the nasal procedure and hearing sensitivity, and provided a positive evaluation of the surgeons.
CONCLUSION: The conchal cartilage seems a highly valuable alternative graft for nasal dorsum augmentation procedures. The technique of using cartilage wrapped in mastoid fascia seems to be an advantageous alternative when compared with those using cartilage wrapped in other fasciae: it has low morbidity and complications rates and can be a great option for saddle nose treatment.
Keywords:
Rhinoplasty; Nasal acquired deformities; Nasal bone; Surgery, Plastic; Nasal Cartilages.
RESUMO
INTRODUÇÃO: A rinoplastia de aumento em muitos casos torna-se mais difícil que a rinoplastia de redução. Enxertos dorsais sólidos realizados com cartilagem costal têm sido muito utilizados para aumento dorsal, porém estão associados com altos índices de revisão, por isso, muitos autores passaram a utilizar cartilagem em cubos envoltos por fáscia. A fáscia da mastoide, conectada ao pericôndrio da cartilagem conchal auricular, pode formar um enxerto composto para o aumento do dorso nasal, sendo também uma opção de tratamento. O objetivo é demonstrar a possibilidade do uso de cartilagem da concha auricular fragmentada fixa ao seu pericôndrio, e envoltos na fáscia da mastoide, formando um enxerto composto para aumento do dorso nasal.
MÉTODOS: Trata-se de um estudo retrospectivo de 9 pacientes operados entre 2012 e 2016 no Hospital de Base da Faculdade de Medicina de São José do Rio Preto, em que foi realizado aumento do dorso nasal com cartilagem conchal fragmentada fixa ao seu pericôndrio e envolto à fáscia da mastoide.
RESULTADOS: Os pacientes foram acompanhados de 6 a 48 meses. Foram questionados quanto à satisfação do procedimento nasal e sensibilidade auricular, com avaliação positiva dos pacientes e cirurgiões.
CONCLUSÃO: A cartilagem conchal parece ser uma alternativa de grande valia para procedimentos de aumento de dorso nasal. Esta cartilagem envolta com fáscia da mastoide parece ser uma alternativa vantajosa em comparação ao uso de outras fáscias, com baixa morbidade e taxa de complicações, podendo ser uma grande opção para tratamento do nariz em sela.
Palavras-chave:
Rinoplastia; Deformidades adquiridas nasais; Osso nasal; Cirurgia plástica; Cartilagens nasais.
INTRODUCTION
Augmentation rhinoplasty, in general, is more difficult than reduction rhinoplasty in many cases. To obtain a satisfactory result, the subunits, including the root, dorsum, tip, and alar base, should be individually evaluated1. Repair of an insufficient nasal dorsum is of utmost importance to obtain a good aesthetic quality of the nose.
According to the literature, the use of cartilage graft cut into cubes and wrapped in the fascia began in the 1940s2. However, the technique became popular after the study conducted by Erol on 2,365 patients where he used cartilage graft cut into cubes wrapped in synthetic material (Surgicel, Ethicon, Inc., Somerville, NJ)3.
The surgical planning for the treatment of low, insufficient, or "saddle" nasal dorsum for cosmetic or reconstructive purposes has significantly improved in the last decades owing to better management of grafts and implants4,5. However, the choice is a subject of controversies and discussions. Several materials are currently described for this purpose, which can be classified into autologous, homologous, and synthetic according to origin.
Solid dorsal grafts performed with costal cartilage have been widely used for nasal augmentation; however, they are associated with high revision rates because of resorption and visible shape changes6-8. Therefore, many surgeons started to use cartilage cut into cubes and wrapped in fascia.
The mastoid fascia is composed of two layers, superficial and deep9. We used the superficial fascia, which corresponds to the superficial temporal fascia. This is connected to the perichondrium of the auricular conchal cartilage, which is fixed to the conchal cartilage. A composite graft was used to naturally join these component structures into a single unit.
OBJECTIVE
The objective was to demonstrate the possibility of using fragmented auricular conchal cartilage fixed to its perichondrium and wrapped in the mastoid fascia, naturally joined in a single unit to form a composite graft augmenting the nasal dorsum and eliminating a new distant surgical site.
METHODS
This was a new proposal for nasal dorsal augmentation that was used in 9 patients operated between 2012 and 2016 at the Base Hospital of the Faculty of Medicine of São José do Rio Preto, SP, where nasal dorsum was augmented with a fragmented conchal cartilage fixed to its perichondrium and wrapped in the mastoid fascia. Eight patients were female, and only one was male. They all had a low or saddle nose as an ethnic or genetic trait, surgically derived, or even induced by traumatic sequelae. The proposed surgery was performed through an "open" technique.
The study was approved by the Ethics Research Committee of the Faculty of Medicine of São José do Rio Preto, under protocol No. 60203316.1.0000.5415.
Surgical technique
A "V"-shaped incision was made in the transition between the triangular and quadrangular forms of the columella to perform an open rhinoplasty technique. Nasal subunits were treated regardless of the dorsum, as the use of grafts or osteotomies.
After the end of this rhinoplasty phase and preparation of the space to augment the dorsum, the auricular conchal cartilage was captured along with its perichondrium and mastoid fascia. A spindle of retroauricular skin was removed without removing the perichondrium. The upper portion of the graft to be obtained (lateral side of the nasal concha; Figure 1) was cut. This was then removed from the skin of the anterior portion of the concha until the desired width and length of the graft was attained, and the lower part of the graft was entirely incised, anteroposteriorly, by preserving the perichondrium (Figure 2).
 Figure 1.
Figure 1. Exposure of the conchal cartilage while keeping the posterior perichondrium intact.
 Figure 2.
Figure 2. Lifting the nasal concha without its anterior perichondrium. The posterior-most incision of the nasal concha is made without damaging the posterior perichondrium.
The graft was folded, and the mastoid fascia was detached from front to back until reaching the desired length and width (Figure 3). The fascia was incised and then fixed to the perichondrium. The cartilage was fragmented with a scalpel, maintaining the connection of the three structures. Subsequently, the cartilage was wrapped in the fascia and fixed to it with 6.0 mononylon wire, making these structures look like a cigar (Figure 4).
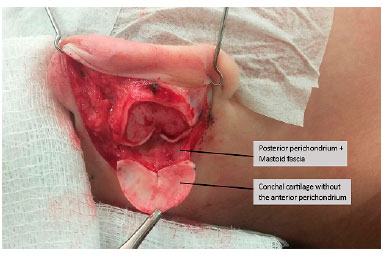 Figure 3.
Figure 3. Dissection of the posterior perichondrium along with the mastoid fascia.
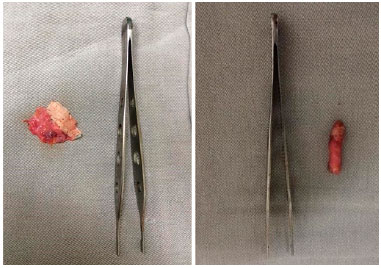 Figure 4.
Figure 4. Composite graft. A. Conchal cartilage fixed to the posterior perichondrium and mastoid fascia. Cartilage incisions were made on the anterior face of the cartilage without incising its posterior perichondrium to fragment the cartilage without detaching it. B. Prepared composite graft with cigar-like appearance.
Once prepared, this composite graft (fascia, perichondrium, and cartilage) was positioned on the nasal dorsum (Figure 5).
 Figure 5.
Figure 5. Positioned graft in the nasal dorsum.
The detached area should be appropriate to the volume and shape of the graft, and does not require its fixation. However, in cases where the dorsum is larger than the graft, the latter should be fixed to the dorsum or sutured. The plaster or moldable bandages were left for 2 weeks.
RESULTS
The results obtained were of good aesthetic quality in all the patients. No complication occurred regardless of the infection, exposure, or graft migration. The patients were monitored for a period ranging from 6 months to 4 years, and were asked regarding their satisfaction with the aesthetic results obtained and hearing sensitivity.
The nine patients were satisfied (3) or happy (6) with the nasal procedure. The patients had no aesthetic complaints regarding the donor area of the graft, and 3 patients reported paresthesia in the posterior region of the ear in the first few postoperative months. Those with greater evolution who were monitored for a longer period did not report paresthesia eventually (Figures 6-9).
 Figure 6.
Figure 6. Ethnic characteristics before and after operation.
 Figure 7.
Figure 7. Ethnic characteristics before and after operation.
 Figure 8.
Figure 8. Surgical sequelae before and after operation.
 Figure 9.
Figure 9. Traumatic sequelae before and after operation.
DISCUSSION
Conchal cartilage is a valuable alternative graft for nasal dorsal augmentation procedures, as demonstrated in this and previous studies. Complication rates are low, and the results are satisfactory. The cartilage is flexible but resistant, and its natural contours, along with its fragmenting procedure, allow an easy modeling10.
This cartilage wrapped in the mastoid fascia seems to be an advantageous alternative when compared with using other fasciae (e.g., the deep temporal fascia), as the latter require an additional donor site. In relation to using the costal cartilage, the advantage relies on the lower morbidity and complication risks of its capturing procedure.
The use of this technique, maintaining the conchal cartilage fixed to its perichondrium and fascia, allows the graft to maintain a more stable length and thickness owing to the low movement of the fragments. The fact that they are naturally bound allows a better integration and vascularization of the components, which does not occur in grafts where parts are connected independently from each other.
CONCLUSION
Augmentation of the nasal dorsum in saddle nose with fragmented auricular conchal cartilage fixed to its perichondrium and wrapped in the superficial fascia of the mastoid is a procedure of easy execution and low morbidity, capturing the graft in a single surgical site of low risk, that provided aesthetic satisfaction in all the cases presented.
For a more positive conclusion, a greater number of operated cases would be required. However, the presented technique is an alternative in situations like these. The results obtained so far compel us to use the technique and search for improvements, as well continue research on the technique.
COLLABORATIONS
AMR Analysis and/or interpretation of data; statistical analyses; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
ARB Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
CGS Conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
MSF Completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
CMRJ Conception and design of the study; completion surgeries and/or experiments.
DHL Completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
REFERENCES
1. Rohrich RJ, Ahmad J. Rhinoplasty. Plast Reconstr Surg. 2011;128(2):49e-73e. PMID: 21788798 DOI: http://dx.doi.org/10.1097/pRS.0b013e31821e7191
2. Calvert JW, Brenner K, DaCosta-Iyer M, Evans GR, Daniel RK. Histological analysis of human diced cartilage grafts. Plast Reconstr Surg. 2006;118(1):230-6. PMID: 16816701 DOI: http://dx.doi.org/10.1097/01.prs.0000220463.73865.78
3. Erol OO. Long-Term Results and Refinement of the Turkish Delight Technique for Primary and Secondary Rhinoplasty: 25 Years of Experience. Plast Reconstr Surg. 2016;137(2):423-37. PMID: 26818276 DOI: http://dx.doi.org/10.1097/01.prs.0000475755.71333.bf
4. Warren RJ, ed. Neligan. Cirurgia Plástica. Volume 2 Estética. 3a ed. Rio de Janeiro: Elsevier; 2015.
5. Sajjadian A, Rubinstein R, Naghshineh N. Current status of grafts and implants in rhinoplasty: part I. Autologous grafts. Plast Reconstr Surg. 2010;125(2):40e-49e. PMID: 19910845 DOI: http://dx.doi.org/10.1097/pRS.0b013e3181c82f12
6. Gurley JM, Pilgram T, Perlyn CA, Marsh JL. Long-term outcome of autogenous rib graft nasal reconstruction. Plast Reconstr Surg. 2001;108(7):1895-905. DOI: http://dx.doi.org/10.1097/00006534-200112000-00007
7. Gunter JP, Landecker A, Cochran CS. Frequently used grafts in rhinoplasty: nomenclature and analysis. Plast Reconstr Surg. 2006;118(1):14e-29e. PMID: 16816668 DOI: http://dx.doi.org/10.1097/01.prs.0000221222.15451.fc
8. Cárdenas-Camarena L, Guerrero MT. Use of cartilaginous autografts in nasal surgery: 8 years of experience. Plast Reconstr Surg. 1999;103(3):1003-14. PMID: 10077096 DOI: http://dx.doi.org/10.1097/00006534-199903000-00039
9. Park C, Lee TJ, Shin KS, Kim YW. A single-stage two-flap method of total ear reconstruction. Plast Reconstr Surg. 1991;88(3):404-12. PMID: 1871216 DOI: http://dx.doi.org/10.1097/00006534-199109000-00004
10. Mischkowski RA, Domingos-Hadamitzky C, Siessegger M, Zinser MJ, Zöller JE. Donor-site morbidity of ear cartilage autografts. Plast Reconstr Surg. 2008;121(1):79-87. PMID: 18176208 DOI: http://dx.doi.org/10.1097/01.prs.0000293879.46560.4c
1. Hospital de Base de São José do Rio Preto, São José do Rio Preto, SP, Brazil
2. Faculdade de Medicina de São José do Rio Preto, São José do Rio Preto, SP, Brazil
3. Hospital Pérola Byington, São Paulo, SP, Brazil
Institution: Faculdade de Medicina de São José do Rio Preto, São José do Rio Preto, SP, Brazil.
Corresponding author:
Aluísio Marino Roma
Av. Brigadeiro Faria Lima, 5416
São José do Rio Preto, SP, Brazil - Zip Code 15090-000
E-mail: zo_roma@hotmail.com
Article received: September 22, 2016.
Article accepted: September 23, 2017.
Conflicts of interest: none.
 All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license


