



Ideas and Innovation - Year 2015 - Volume 30 -
Frontotemporal minilifting for eyebrow tail suspension: Minimally invasive Reis-Sundfeld technique
Minilifting fronto-temporal para suspensão de cauda de supercílio: técnica minimamente invasiva de Reis-Sundfeld
ABSTRACT
INTRODUCTION: An important sign of facial aging is the fall of the eyebrow tail. Frontotemporal minilifting aims to reposition the brow and soften the expression marks to restore youthful appearance. To describe an ambulatory surgical technique capable of eyebrow tail lift with minimal scarring and wound camouflage in the capillary line that reduces the facial signs of aging.
METHOD: The study included 10 consecutive patients who attended the Plastic Surgery outpatient clinic of the UNIFESP and submitted to minilifting after receiving the diagnosis of eyebrow fall.
RESULTS: Preliminary results did not show the occurrence of major complications. All patients were women. One patient presented with small suture line dehiscence 15 days after surgery. A total of 90% of the patients scored their body image index as extremely satisfied or satisfied. The average eyebrow tail lift was 5 mm. The average preoperative eyebrow fall was 13.3 mm, with a mean elevation and maintenance of 18.2 mm in 12 months.
CONCLUSION: The technique is easily reproducible, provides outcomes comparable to those of other procedures published in the literature, and presents the following advantages: is low cost; can be performed in an outpatient clinic; provides a rejuvenating periocular effect since it also reduces wrinkles, expression marks, and sagging of the lateral region of the orbital and glabellar fissure; and achieves significant long-lasting results.
Keywords: Face; Rejuvenation; Ambulatory surgical procedures; Reconstructive surgical procedures
RESUMO
INTRODUÇÃO: Um sinal importante do envelhecimento facial é a queda da cauda da sobrancelha. O minilifting frontotemporal visa reposicionar a sobrancelha e amenizar as marcas de expressão, restaurando uma aparência mais jovial. Descrever uma técnica cirúrgica, ambulatorial, capaz de elevar a cauda da sobrancelha, com cicatriz mínima e camuflada na linha capilar, melhorando o aspecto de envelhecimento facial.
MÉTODO: Foram arregimentados dez pacientes sequenciais do ambulatório de cirurgia plástica da UNIFESP, que após diagnóstico de queda de supercílio foram submetidos ao minilifting.
RESULTADOS: Como resultados preliminares, não houvera nenhuma complicação importante, todos pacientes eram mulheres, um caso apresentara pequena deiscência em linha de sutura após 15 dias de cirurgia. 90% apresentaram índice de imagem corporal em extremamente satisfeitos ou satisfeitos. A média de elevação da cauda do supercílio foi de 5 mm. A média de queda de supercílio pré-operatória foi de 13,3 mm, tendo sua elevação média e manutenção em 12 meses de 18,2 mm.
CONCLUSÃO: A técnica sugerida pelos autores é de fácil reprodutibilidade, produz resultados comparáveis às demais técnicas da literatura com as vantagens de apresentar baixo custo, ser realizada ambulatorialmente e ter um efeito rejuvenescedor periocular, pois atenua também as rugas, marcas de expressão e flacidez da região lateral da fissura orbitária e glabelar com significativo tempo de manutenção de resultados.
Palavras-chave: Face; Rejuvenescimento; Procedimentos cirúrgicos ambulatoriais; Procedimentos cirúrgicos reconstrutivos.
Facial aging is multifactorial. Over time, gravity, constant muscular contractions, and loss of skin elasticity form lines in the frontal region and glabellar furrows that lead to eyebrow fall1,2.
The orbital region is an extremely expressive facial area. Eyebrow position in particular conveys facial expressions. Depending on its shape and position, an individual may assume an air of fatigue, vigor, or other moods. Eyebrow and eyelid ptosis are among the main complaints during plastic surgery consultations1,3.
This phenomenon usually occurs after 45 years of age, when the lateral region of the eyebrow tail presents the greatest degree of ptosis, thus causing excess skin on upper eyelids that sometimes exceeds the eyelashes2,4. In addition to the aged appearance of the orbital region, another common complaint is visual difficulty due to the decreased amplitude of eyelid opening that reduces the visual field3.
Eyebrow ptosis results in a false appearance of excess upper eyelid skin. If not promptly recognized upon physical examination, it might lead the patient to undergo inappropriate procedures that worsen the ptosis. This is due to the decreased space between the eyebrow and the "ciliary level" induced by conventional blepharoplasty4. Therefore, careful evaluation should be performed along with morphological characteristic assessment to contextualize the patient's complaints. Eyelid pseudoptosis caused by eyebrow ptosis in patients who do not desire to undergo more invasive surgeries and/or procedures that can result in visible marks on the eyebrows when inadequately treated with blepharoplasty will hinder passive eyelid closure during sleep and might cause severe ocular involvement3.
Numerous brow lift5 procedures and surgical techniques have been described to date. Since 1919, when the first technique using elliptical excisions of the frontal and temporal regions was published, such procedures have undergone major advances, especially with the introduction of the endoscope5.
Among the cited techniques, we highlight the surgery performed by Castañares because using an elliptical excision of the skin just above the eyelids6 or through small lateral incisions of the eyebrows (mini Castañares), long-lasting and desirable eyebrow tail lifting7 results have been achieved. However, this procedure may result in visible scars, decreased eyebrow thickness, or super arching with a "clown makeup" effect.
As a non-surgical alternative to eyebrow repositioning and instead of using lasers that redensify and contract the collagen, it is possible to inject botulinum toxin in different depressant muscles. However, this procedure leads to an ephemeral lifting effect of this region8.
OBJECTIVE
To describe a minimally invasive surgical technique for correcting eyebrow tail ptosis.
MATERIAL AND METHOD
In a screening performed at the Plastic Surgery outpatient clinic of the UNIFESP, we sequentially selected a group of 10 patients aged > 45 years who presented with eyebrow tail ptosis. All patients were informed about the surgical procedures, risks, and possible complications and provided written informed consent for the surgery, participation in the study, and use of their images.
These procedures were performed according to the protocols and regulations established by the Research Ethics Committee of the Paulista Medical School-Federal University of São Paulo-and the standards of the Resolution 196/96 of CNS.
After a medical consultation, the patients answered the body image index questionnaire9 and were referred to the outpatient surgical clinic. First, markings were made according the following images: Figures 1 and 2 in which the lines were delimited as mid-pupillary (MP), the line that passes through the excantium parallel to the mid-pupillary (EC), and the line delimited by the eyebrow final excantium (EFEC). After these markings were made, point X was defined by digital examination and represented the apex of a triangle used to determine the degree to which the eyebrow tail would be lifted. This figure point was on a line parallel to the EFEC line and intersected the EC line with the highest eyebrow portion. Finally, the last apex of the triangle was defined by the intersection between a line parallel to the EFEC line and the line that crosses the MP line intersection at the highest eyebrow portion (Figures 1 and 2).

Figure 1. Baseline markings: Mid-pupillary (MP), Excantium (EC), Eyebrow Final-Excantium (EFEC) and point X, according to the lifting required.
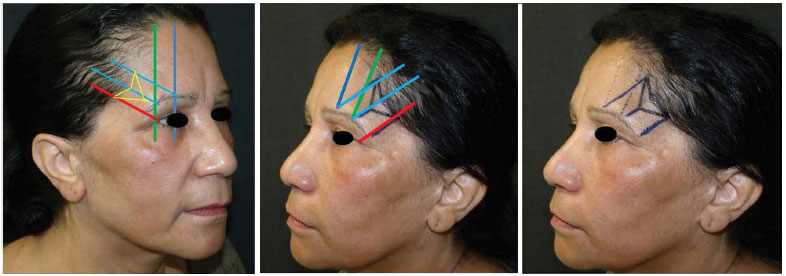
Figure 2. Schematic marking performed on the patient.
Following these markings, the patients were placed in the supine position. Antisepsis was performed with 2% chlorhexidine. The patients submitted to local anesthesia (2% xylocaine solution with vasoconstrictor) and were placed within a sterile field. Cephalosporin was used as the first-generation antibiotic. After the excision of the triangular contour of the frontotemporal skin region to the subdermal level, the procedure was continued under strict hemostasis.
We then performed the technique proposed by these authors using a subdermal Mononylon 4.0 suture that was colorless in the portion of the triangle apex toward the base midpoint. This provided the suspension of the eyebrow tail to the distance that was previously determined during the clinical examination by measuring the Frankfurt's plane (FP) and the end of the eyebrow tail (Figure 3). Other sutures were placed to ensure wound symmetry. External Mononylon 5.0 sutures were separately added, and it was then possible to observe the procedural effects.

The aforementioned procedures were repeated in the contralateral frontotemporal region and compared for symmetry. A skin-colored Micropore dressing was applied. Patients returned for follow-up on the 1st, 7th, and 14th postoperative days as well as 1, 3, 6, and 12 months after surgery.
In all visits, the patients were photographed for later comparison and evaluated for the occurrence of complications such as infection, hematoma, epidermolysis, paresthesia, suture dehiscence, recurrence of eyebrow ptosis, and wire extrusion. Measurements were taken directly between FP and the end of the eyebrow tail to control the suspension effects (Figure 4).
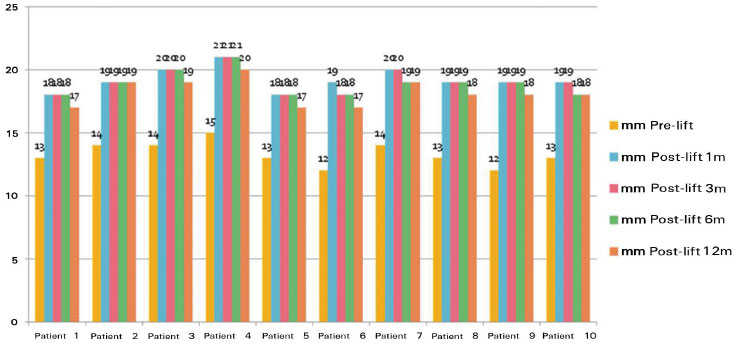
Figure 4. Lifting levels before surgery and 1, 3, 6, and 12 months after surgery.
The measurement was taken with patients in the orthostatic position with a neutral look fixed on the horizon and the facial muscles relaxed. A digital caliper (0.01-mm precision; OTMT Machines, NY, USA) was used to measure the distance between the endpoint of the eyebrow and FP (Figure 3), which defined a line (X) connecting these points and created a 90º angle with FP (Figures 5, 6, and 7).

Figure 5. Measurement parameters.
Source: www.cleber.com.br/padrao2011/erros.html

Figure 6. Measurement parameters.
Source: www.cleber.com.br/padrao2011/erros.html
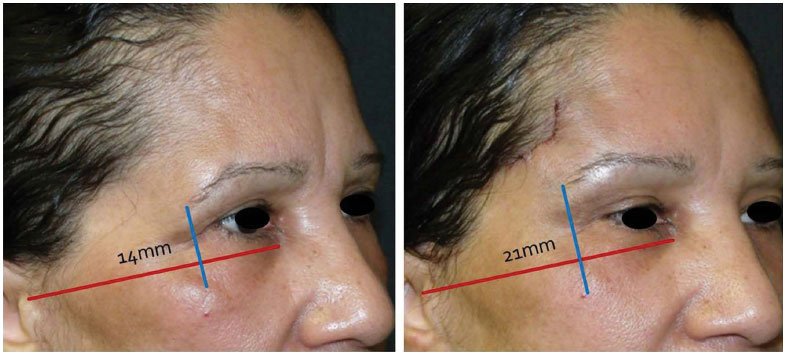
Figure 7. Measurement examples during the immediate pre- and postoperative periods.
By definition, FP is the plane established by the lowest point of the orbital margin and the highest point of the external ear conduct10. Therefore, it represents an important reference point since it undergoes little change with age. This allows it to be chosen as the fixed point in the measurements performed in this study.
All patients completed the body image index questionnaire within 6 months after surgery.
The results and analysis of the questionnaires were plotted on graphs to better visualize the obtained data.
RESULTS
The initial results obtained during follow-up within 12 months show that there were no cases of infection, hematoma, paresthesia, or relapse in this group of 10 patients. The only complication, a case of small unilateral dehiscence that was observed 15 days after surgery, was resolved without compromising the surgical results.
In the initial measurements, we set the average value at 13.3 mm, thus leading to a median of 13 mm among the 10 patients. One month after surgery, the average was 19.2 mm and the median was 19 mm. During the sixth postoperative month, the average was 18.9 mm and the median was 18 mm. At the end of the 12th postoperative month, the average was 18.2 mm and the median was 18 mm. These results are shown in Figure 4.
Regarding the self-assessed satisfaction questionnaires, the results obtained (Figures 8 and 9) show significant improvement in patient self-esteem: 70% of the patients declared preoperative dissatisfaction, whereas 90% were extremely satisfied or satisfied 6 months after surgery.

Figure 8. Preoperative satisfaction index.

Figure 9. Postoperative index 6 months after surgery.
As a portrait of the surgical results illustrating our findings in addition to the graphs, several examples of patient evolution before versyus 12 months after surgery are illustrated in Figures 10 and 11.

Figure 10. Patient before surgery and 12 months after surgery, showing lifting maintenance.

Figure 11. Patient before surgery and 12 months after surgery without visible scarring.
DISCUSSION
As an archetype, the human beauty is represented mainly by the face with all its nuances and emotional expression in addition to the characteristics of body aging phases. This demonstrates the great importance of facial expressions and the proportions of its constituents in social relationships and human health.
In this context, the eyebrows, especially their tail movements and positions, represent the region of the face with the greatest ability to portray an individual's emotions as well as age. The artist Gordon C. Aymar stated: "the eyes are the place which reveal the most complete, relevant and reliable information about the subject, and the eyebrows can report, almost by themselves, wonder, pity, fear, pain, cynicism, concentration, nostalgia, discontent, and hope, in infinite variations and combinations"11.
The Reis-Sundfeld frontotemporal minilifting technique aims to soften periocular wrinkles and reposition the eyebrow to restore a more youthful13 and vigorous look12,13,14. An important sign of aging is loss of the eyebrow tail, which gives the face a sad look. With the minimally invasive suspension described herein, the eyebrow as well as the adjacent upper eyelid tissue can be lifted. This results in reduced wrinkles, expression marks and sagging developing in the lateral region of the orbital and glabellar fissure.
To obtain satisfactory results with eyebrow lifting, a thorough evaluation of the position and characteristics of the tissue surrounding the eyes, brows, and forehead is required13,14. The shape and face bone structure as well as the shape and height of the eye in relation to the hairline (the upper third of the face, nose, mouth, eyelids, and temples) should be considered during the physical evaluation of the face1,2,4.
The medial end of the eyebrow should start at the level of the ipsilateral nostrils, and the space between them is equal to the distance between the eyes1,4. The lateral end of the eyebrow corresponds to an imaginary line connecting the nostrils to the region of the outer corner of the eye. The highest part of this curvature (arch) should be perpendicular to the external side of the iris1,2,4.
These anatomical characteristics determine the need to adapt the lifting vector of the eyebrow tail to achieve a more natural result. Several authors to date have attempted to determine the best lifting vector for the treatment of eyebrow tail ptosis. Among them, we should mention the vectors recommended by Westmore, Lamas, and Anastasia, as described in the article published by Hamamoto et al.15. In the technique proposed by this author, the vector used is similar to that used by Anastasia, which is now characterized by the experts as the most accepted method.
Patients who benefit from the surgery performed using the technique proposed by the authors are those with sagging and ptosis of the eyebrow tail but no excess eyelid tissue. This technique uses marks including the mid-pupillary line, lateral border of the orbital fissure, and lateral end of the eyebrow. A triangular incision in the frontotemporal region is performed with the base of the triangle in the capillary insertion to camouflage the suture line. There are no absolute or specific contraindications to performing this surgery.
The choice of this technique, instead of possible rhytidoplasty or video-assisted frontal surgeries, both of which are extended procedures, should be made according to the surgical indication with consideration of its advantages and limitations.
In the literature, we found techniques that envision facial rejuvenation, particularly in the ocular region. However, when compared to the technique described herein, these present an increased realization complexity and the use of non-absorbable sutures to fix the flaps after extensive dissection13,14. Frontotemporal minilifting allows lifting of the eyebrow tail to the same extent as that in the procedures described by Castañares and video-assisted frontal lifting. The eyebrow tail suspension level is comparable but lacks eyebrow scar stigma compared to that in Castañares technique and less scarring than that of video-assisted frontal lifting.
Another factor that should be highlighted is that the results can be seen immediately after the procedure and last for > 12 months. Even as an adjuvant treatment to the surgery, it is possible to use botulinum toxin in the depressant muscles of the frontal region to provide a synergistic effect in the rejuvenation of the upper third of the face caused by the frontotemporal minilifting13. This would further improve the results obtained with the technique described herein.
CONCLUSION
The technique proposed here is an excellent option for the treatment of eyebrow tail ptosis since it is minimally invasive, low cost, and performed on an outpatient basis. It also presents minimal or no complications.
This procedure is easy to perform and its associated delimiting lines are easy to determine with well-defined points, which renders this technique reproducible to surgeons. The results we obtained showed an average lifting comparable to that of techniques that are currently considered the standard, e.g. video-assisted and coronal frontoplasty, with a long lasting result as evidenced at 12 months postoperative.
It should be noted that due to the initial small number of patients who underwent this surgery and were followed up for > 12 months, further procedures will be required to fully confirm its efficacy. However, the obtained results already demonstrate the procedure's quality and feasibility since the simplicity of its realization, reproducibility of delimiting lines, and durability in maintaining the results achieved in a midterm timeframe are highly significant for the current state of the art of facial surgery.
From the above, when well indicated, we propose this simple surgical technique that is reproducible, performed with local anesthesia, and can provide satisfactory aesthetic outcomes.
REFERENCES
1. Naif-de-Andrade NT, Hochman B, Naif-de-Andrade CZ, Ferreira LM. Computerized photogrammetry used to calculate the brow position index. Aesthetic Plast Surg. 2012;36(5):1047-51. DOI: http://dx.doi.org/10.1007/s00266-012-9961-7
2. Feser DK, Gründl M, Eisenmann-Klein M, Prantl L. Attractiveness of eyebrow position and shape in females depends on the age of the beholder. Aesthetic Plast Surg. 2007;31(2):154-60. DOI: http://dx.doi.org/10.1007/s00266-006-0149-x
3. Knize DM. Anatomic concepts for brow lift procedures. Plast Reconstr Surg. 2009;124(6):2118-26. PMID: 19952669 DOI: http://dx.doi.org/10.1097/PRS.0b013e3181bd0726
4. Griffin GR, Kim JC. Ideal female brow aesthetics. Clin Plast Surg. 2013;40(1):147-55. DOI: http://dx.doi.org/10.1016/j.cps.2012.07.003
5. Paul MD. The evolution of the brow lift in aesthetic plastic surgery. Plast Reconstr Surg. 2001;108(5):1409-24. PMID: 11604652 DOI: http://dx.doi.org/10.1097/00006534-200110000-00048
6. Castañares S. Forehead wrinkles, glabellar frown and ptosis of the eyebrows. Plast Reconstr Surg. 1964;34:406-13. DOI: http://dx.doi.org/10.1097/00006534-196410000-00011
7. Vinas JC, Caviglia C, Cortinas JL. Forehead rhytidoplasty and brow lifting. Plast Reconstr Surg. 1976;57(4):445-54. PMID: 1273125 DOI: http://dx.doi.org/10.1097/00006534-19760400000006
8. Punthakee X, Keller GS, Vose JG, Stout W. New technologies in aesthetic blepharoplasty and brow-lift surgery. Facial Plast Surg. 2010;26(3):260-5. DOI: http://dx.doi.org/10.1055/s-0030-1254337
9. Mélega MP. Aspectos psicológicos do paciente em cirurgia plástica. In: Mélega MP, ed. Cirurgia Plástica. Fundamentos e Arte. Rio de Janeiro: Medsi; 2002. p.221-7.
10. Noções e Conceitos Básicos em Oclusão, Disfunção Temporomandibular e Dor Orofacial; Helson José de Paiva e Colaboradores; Livraria Santos Editora, 2008.
11. Gordon C. Aymar, The Art of Portrait Painting, Chilton Book Co., Filadélfia, 1967, p. 93.
12. Arneja JS, Larson DL, Gosain AK. Aesthetic and reconstructive brow lift: current techniques, indications, and applications. Ophthal Plast Reconstr Surg. 2005 Nov;21(6):405-11.
13. Centurión P, Romero C. Lateral brow lift: a surgical proposal. Aesthetic Plast Surg. 2010 Dec;34(6):745-57. doi: 10.1007/s00266010-9537-3. Epub 2010 Jun 30.
14. Alex JC. Aesthetic considerations in the elevation of the eyebrow. Facial Plast Surg. 2004 Aug;20(3):193-8.
15. Hamamoto AA, Liu TW, Wong BJ. Identifying ideal brow vector position: empirical analysis of three brow archetypes. Facial Plast Surg. 2013 Feb;29(1):76-82. doi: 10.1055/s-0033-1333841. Epub 2013 Feb 20.
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Universidade Federal de São Paulo, São Paulo, SP, Brazil
Institution: Universidade Federal de São Paulo - Escola Paulista de Medicina, São Paulo, SP, Brazil.
Corresponding author:
Daniel Sundfeld Spiga Real
Rua Passeio das Palmeiras, 520
São Carlos, SP, Brasil Zip Code 13561-353
E-mail: daniel.ssr@hotmail.com
Article received February 2, 2014.
Article accepted August 31, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket