ABSTRACT
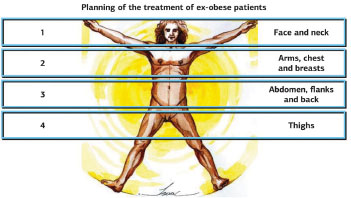
INTRODUCTION Ex-obese patients require a complex surgical approach because of the large amount of excess skin due to their massive weight loss. In some cases, several plastic surgeries are needed, and there is no existing standard in the coordination of these surgeries. In the upper segment of the body, the arms, side of the thorax, and breasts are usually affected, mainly in women. Several techniques have been developed with the aim of achieving better results with better hidden scars. Some techniques may be associated, being carried out in a single surgical procedure. A well-structured surgical team leads to a reduced surgical time, which means higher safety for the patient.
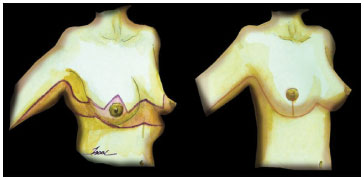
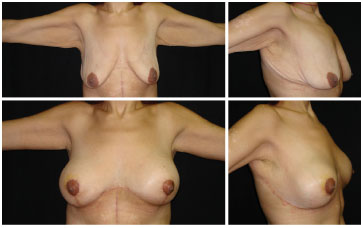
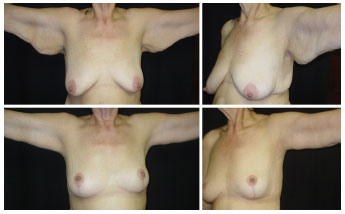
METHOD: We present a technique for standardization in the treatment of ex-obese patients that is performed in a single step, comprising mammoplasty (according to Pitanguy's technique or with placement of breast prosthesis), thoracoplasty (with the removal of excess skin on the side of the chest), and brachioplasty (performed with a rectilinear drawing at the lowest part of the arms).
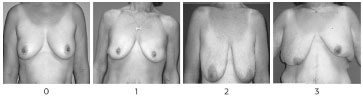
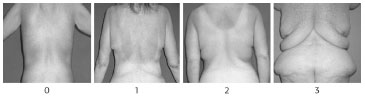
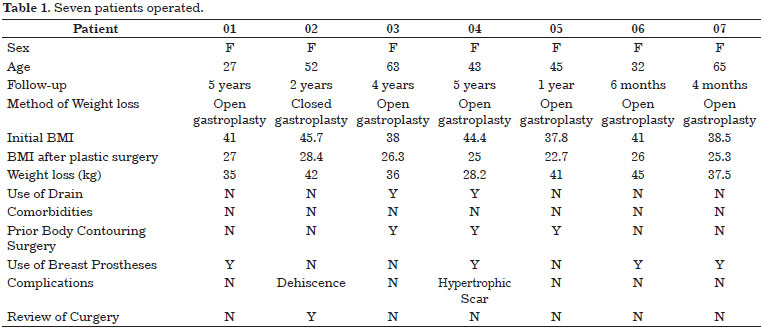
RESULTS: Seven cases were evaluated in terms of surgical time, location of the scars, and final shape and symmetry. The complications included partial dehiscence (14%) and hypertrophic scars (14%). The aesthetic result was satisfactory for 84% of the patients; on the other hand, the quality of cicatrization, keloid, and hypertrophic scars were the major causes of dissatisfaction.
CONCLUSION: The use of the thoracobrachio-mammoplasty technique in a single surgical time was effective in the treatment of ex-obese patients, offering yet another option among other surgeries that these patients usually need.
Keywords:
Mammoplasty; Brachioplasty; Thoracoplasty; Plastic surgery in ex-obese.
RESUMO
INTRODUÇÃO Os pacientes ex-obesos necessitam de uma abordagem complexa, diante do grande excesso de pele decorrente da perda ponderal. Em alguns casos, muitas cirurgias plásticas são necessárias, não havendo uma padronização na associação destas cirurgias. No segmento superior do corpo, a região dos braços, a lateral do tórax e as mamas normalmente são acometidas, principalmente nas mulheres. Diversas técnicas foram desenvolvidas com o objetivo de alcançar resultados melhores e com cicatrizes mais escondidas. Algumas técnicas podem ser associadas, sendo realizadas em um único tempo cirúrgico. Quando a equipe é bem estruturada, o tempo cirúrgico é reduzido, significando mais segurança para o paciente.
MÉTODO: Os autores apresentam uma técnica que oferece padronização no tratamento do ex-obeso, que é realizada em tempo único: a Mamoplastia (pela técnica de Pitanguy ou com aposição de prótese mamária), a Toracoplastia (com a retirada do excesso de pele na lateral do tórax) e a Braquioplastia (realizada com um desenho retilíneo na parte mais inferior dos braços).
RESULTADOS: Os sete casos foram avaliados quanto ao tempo cirúrgico, à localização das cicatrizes, à forma final e à simetria. Entre as complicações, houve deiscências parciais (14%) e cicatrizes hipertróficas (14%). O resultado estético foi satisfatório para os pacientes em 84% dos casos, sendo que a qualidade da cicatrização do paciente, queloide ou cicatrizes hipercrômicas, foi a maior causa de insatisfação.
CONCLUSÃO: A utilização da técnica de Toracobraquio-mamoplastia em um único tempo se mostrou efetiva no tratamento do ex-obeso, oferecendo mais uma opção, diante das outras cirurgias que estes pacientes normalmente necessitam.
Palavras-chave:
Mamoplastia; Braquioplastia; Toracoplastia; Cirurgia plástica em ex-obeso.