ABSTRACT
BACKGROUND: Venous ulcers are a major public health problem worldwide and are responsible for considerable economic impact because of their high incidence. In addition to restricting daily living and leisure activities, they may result in changes in quality of life and self-esteem, and even lead to depression. The aim of this study is to evaluate the quality of life in patients with venous ulcers who are being treated with Unna's boot compression therapy.
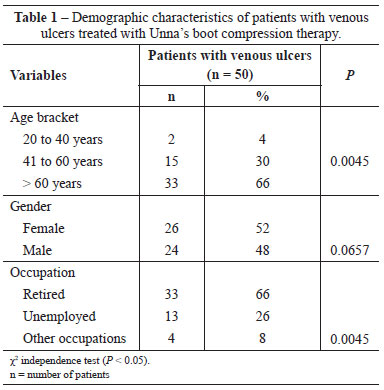
METHODS: Fifty patients with venous ulcers treated at the Conjunto Hospitalar de Sorocaba were enrolled. Data were collected using the Short Form-36 (SF-36) health survey upon inclusion in the study and after 4, 8, and 12 months of compression therapy.
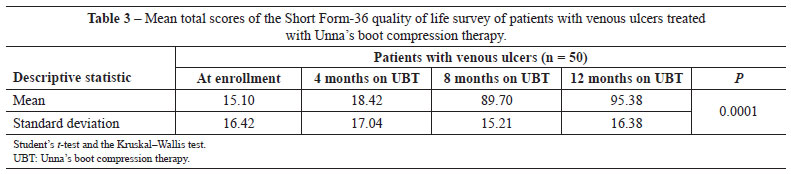
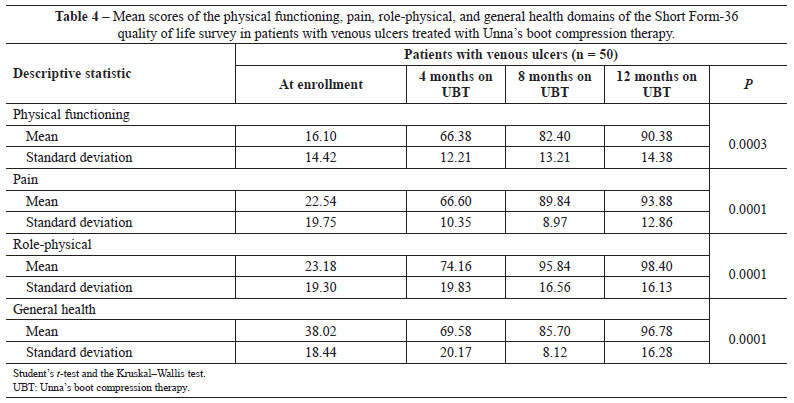
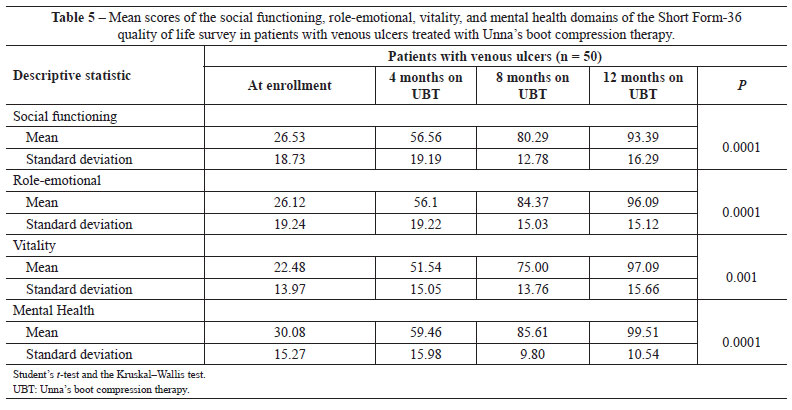
RESULTS: Initial mean SF-36 scores were low (15.10), indicating decreased quality of life. After 12 months of Unna's boot compression therapy, the mean SF-36 score was 95.38, indicating improved quality of life (P = 0.0001).
CONCLUSIONS: Patients with venous ulcers at the beginning of data collection had lower quality of life but improved after 8 months of treatment with Unna's boot compression therapy.
Keywords:
Leg ulcer. Varicose ulcer. Quality of life. Pain. Self concept. Nursing care.
RESUMO
INTRODUÇÃO: As úlceras vasculares vêm se constituindo um grande problema de saúde pública em todo o mundo, sendo responsáveis por considerável impacto econômico pela elevada incidência dessas lesões crônicas. Além de restringir as atividades da vida diária e o lazer, pode ter como consequência alteração na qualidade de vida e na autoestima, levando o paciente, até mesmo, à depressão. O objetivo deste estudo é avaliar a qualidade de vida em pacientes com úlcera venosa que estão sendo tratados com terapia compressiva por bota de Unna.
MÉTODO: Foram selecionados 50 pacientes com úlcera venosa em tratamento no Ambulatório de Feridas do Conjunto Hospitalar de Sorocaba (Sorocaba, SP, Brasil). A coleta de dados foi realizada no momento da inclusão no estudo, sendo repetida aos 4 meses, 8 meses e 12 meses após a primeira coleta de dados, utilizando o questionário Short Form-36 (SF-36).
RESULTADOS: Durante a inclusão do paciente no estudo, os escores médios do SF-36 foram baixos (15,10), caracterizando queda da qualidade de vida. Após 12 meses de terapia compressiva por bota de Unna, o escore médio foi de 95,38, caracterizando melhora da qualidade de vida dos pacientes analisados (P = 0,0001).
CONCLUSÕES: Os pacientes com úlcera venosa, no início da coleta de dados, apresentaram qualidade de vida baixa, e após 8 meses de tratamento com bota de Unna foi observada melhora da qualidade de vida.
Palavras-chave:
Úlcera da perna. Úlcera varicosa. Qualidade de vida. Dor. Auto-imagem. Cuidados de enfermagem.