



Review Article - Year 2011 - Volume 26 - Issue 4
Psychological approach for post-bariatric plastic surgery
Abordagem psicológica em cirurgia plástica pós-bariátrica
ABSTRACT
Nowadays, plastic surgery plays an important role in the surgical treatment of morbid obesity, and it is used to restore optimal body contour in a large number of patients with massive weight loss. The outcome of surgery may affect the patient's psychological behavior, and a multispecialty approach should be adopted, before and after the gastric bypass, to better educate and prepare patients for the dramatic changes they will experience in their body image. The increase in bariatric surgery has also resulted in a greater demand for plastic surgery. In addition to the multispecialty services, patients are seeking out private practice surgeons who will need to recognize and manage the psychological aspects of candidates who undergo body reshaping. This paper reviews the literature on the complex psychological environment of obese patients, emphasizing the identification and management of psychological disorders, and providing plastic surgeons with tools for safer planning and superior outcomes in body contouring after massive weight loss.
Keywords: Mental disorders. Plastic surgery. Bariatric surgery. Motivation.
RESUMO
Atualmente, a cirurgia plástica vem se firmando cada vez mais como parte integrante do tratamento cirúrgico da obesidade mórbida, na medida em que visa a devolver as melhores condições de contorno corporal ao enorme contingente de pacientes submetidos a grandes perdas ponderais. Os aspectos peculiares que acompanham essa nova trajetória do paciente obeso exigem abordagem interdisciplinar, com cuidadoso acompanhamento psicológico, antes e depois da cirurgia bariátrica, que deverá prepará-lo continuamente para as grandes transformações impostas a sua imagem corporal. Com a popularização das gastroplastias e a crescente demanda por procedimentos de contorno corporal após grandes emagrecimentos, é cada vez mais comum a presença desses pacientes nos consultórios de cirurgiões que não estão ligados aos serviços multidisciplinares, e que, portanto, precisam conhecer, avaliar e lidar também com os aspectos psicológicos envolvendo candidatos a cirurgia plástica pós-bariátrica. Este trabalho estabelece uma revisão da literatura acerca do complexo ambiente psicológico na obesidade, voltada para o cirurgião plástico, com ênfase na identificação e no controle das condições psíquicas desfavoráveis, possibilitando o melhor planejamento operatório em pacientes com perda significativa de peso após cirurgia bariátrica.
Palavras-chave: Transtornos mentais. Cirurgia plástica. Cirurgia bariátrica. Motivação.
The psychoemotional profile of candidates for post-bariatric plastic surgery is of great importance in the general approach to treating these patients; failure to perform an adequate assessment and provide proper professional psychological support may lead to failure of the procedure, with disastrous consequences such as surgical morbidity. Obesity is generally a chronic condition and may have affected the patient since early childhood; this may be a reason why psychological disorders are common and, unlike clinical morbidities, are not always alleviated by weight loss.
Patients seen in large centers, multispecialty services, and specialized obesity treatment centers normally undergo complete psychological assessment before and after weight loss, with strict follow-up by experienced professionals as part of a standard assistance protocol. However, the increase in bariatric surgery has also created a greater demand for body contouring procedures after massive weight loss. In addition to the multispecialty services, these patients are seeking out private practice surgeons who will need to recognize and manage the psychological aspects of candidates who undergo body reshaping.
This study reviews the literature on the complex psychological aspects of obese patients, emphasizing the identification and management of psychological disorders, and providing plastic surgeons with tools for safer planning and superior outcomes in body contouring after massive weight loss.
METHODS
We searched MEDLINE/PubMed, Ovid, and LILACS databases for English, Spanish, and Portuguese language papers on the psychological aspects of obese patients before and after bariatric surgery, and their consequences for body contouring.
Combinations of the keywords "psychological," "bariatric surgery," "massive weight loss," and "body contouring" and their translations were used for the searches.
The published studies were used as source material for a discussion on the psychological aspects of weight loss patients after bariatric surgery, with special emphasis on those seeking plastic surgery for body contouring.
The importance of the publications was assessed by the level of scientific evidence, as well as by the experience of the different multispecialty services that followed the patients. Recommendations are offered (by the plastic surgeon) for a preliminary assessment of the psychological conditions that affect post-bariatric patients seeking body contouring surgery.
DISCUSSION
There is no consensus in the literature that obesity increases the prevalence of psychological disorders. However, the obese population faces a number of unfavorable situations that, in association with other variables such as gender, age, education, and socioeconomic status, make them susceptible to psychological problems. Similarly, obese individuals do not display a single pattern of personality traits, although most patients have low self-esteem resulting from their poor body image and eating compulsions, accompanied by feelings of guilt and regret. Many patients feel disappointed in their inability to control their eating habits and lose weight by themselves. Moreover, they are frequently humiliated in their social lives, either by the prejudiced and discriminatory attitude of others, or by their unpleasant experiences with the use of chairs, corridors, restrooms, and other installations that are not adapted for use by obese individuals. Difficulties in maintaining personal hygiene may lead to the development of unpleasant smells. In addition, the sexual and interpersonal relationships of obese individuals, when they occur, are generally dissatisfying due to poor choices of partner, or to thoughts that it would be impossible to find someone "better." Life then becomes unsatisfactory, with an irremediable feeling of hopelessness1.
Obese patients often experience chronic depression, and the decreased quality of life leads many to feel they have nothing to lose, and thus approach bariatric surgery without fear. Differing degrees of anxiety are commonly encountered, and social isolation is usually experienced in proportion to the person's weight, resulting from feelings of rejection and the physical limitations of carrying out daily activities. Among the most severe diseases that may be present and require diagnosis and treatment are bipolar disorders, obsessive-compulsive disorders, and schizophrenia2.
Despite the negative psychological environment, the major motivating factor for obese patients to undergo bariatric surgery is not the desire to improve their self-image, but the need to control clinical comorbidities that are often disabling and threaten quality of life3. It is recognized that bariatric surgery promotes considerable improvement in the obese individual's quality of life, and that weight loss may significantly decrease, or even cure, many clinical comorbidities such as diabetes, hypertension, and sleep apnea4. However, some studies have demonstrated that psychological disorders are more intractable, and often persist after bariatric surgery5.
Most bariatric surgery services follow a protocol for the assessment and management of psychological conditions in obese patients, with preoperative exams and postoperative follow-up. The objective of these assessments is to identify psychological conditions that are optimal for or detrimental to achieving favorable post-bariatric outcomes, although the efficacy of these protocols is controversial6.
Rutledge et al.7 prospectively compared the psychological behaviors of patients who underwent massive weight loss with and without bariatric surgery, and concluded that psychological conditions detected in preoperative assessments, provided they are managed, do not preclude a successful surgical outcome.
The findings of Guisado et al.8 demonstrate that post-bariatric patients with psychological disorders have more eating behavior disorders than do psychologically stable patients. Among such disorders, the most frequently encountered in the literature is uncontrolled eating compulsion, which has an incidence of between 50%9,10 and 5%11 in the post-bariatric population.
Odom et al.12 researched the causes of obesity recurrence in post-bariatric patients and identified some behavioral disorders that were more tied to improvement of quality of life and development of self-control skills than to pre-existing psychological disorders. Rigorous education and follow-up of patients in the postoperative period is essential for prevention of weight gain, and requires management of alcohol misuse and eating compulsions. This position was also advocated by Funnell et al.13, who suggested an educational program tailored to the patient.
Hayden et al.14 observed that weight loss greatly reduces depressive symptoms in bariatric patients regardless of their preoperative condition. This same position is advocated by more recent studies that consider that preoperative psychological assessments should identify and propose treatment of pathological situations, rather than excluding the patient from surgery15-20.
There is no doubt that indexes of depression, anxiety, and other diseases persist and may increase in the 18 to 24 months after bariatric surgery. In many cases, they may lead to recurrence of obesity or even to substitution with other self-destructive behaviors, such as anorexia nervosa and bulimia, or alcohol and drug abuse. It is not clear if such behavior relates more to conditions prior to surgery or to the discomfort from excess skin that results from pronounced weight loss. Several studies have sought to perform comparisons, and to identify the variables involved in this process21,22.
Specialized centers for the treatment of obesity invest in a multispecialty approach that promotes the diagnosis and treatment of conditions to maintain psychological health at all stages of treatment - before and after bariatric surgery and preparation for body contouring plastic surgery23-26. Individual psychiatric care focuses on specific conditions, while group counseling offers broader discussion of the possibilities and limitations of treatment, and enables the exchange of experiences in a support group with a common ideal, bringing together patients, family, and health professionals27,28. The so-called "obesity workshops" that were popularized by Resende29 offer great assistance and motivation for successfully fighting against obesity. Among other benefits, these educational meetings promote and encourage relationships between professionals and their patients through the routine exchange of information and experiences at all phases of treatment.
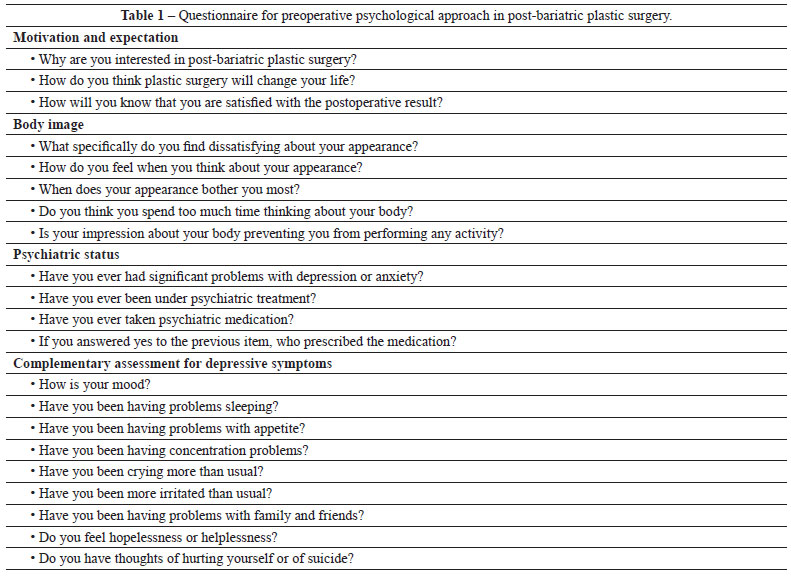
Regardless of the method of patient follow-up, a preliminary psychological assessment should be conducted by the plastic surgeon when the contouring procedures are scheduled. Sarwer et al.30 suggested the use of a standard questionnaire (Table 1) that seeks to assess, albeit superficially, the patient's real motivations and expectations with regard to the procedure, as well as their perception of body image and psychiatric status.
Motivation and Expectations
The post-bariatric patient should be encouraged to undergo plastic surgery. However, the motivation to do so should result from the patient's own desire to increase self-esteem by improving the physical conditions that he or she identifies and recognizes as unfavorable.
When the patient's major surgical motivation is to satisfy a third party's needs or aspirations, whether family or spouse, a new multispecialty approach is required that includes professional counseling. The patient should be helped to understand his or her real motivations and to exclude others' opinions as motivating factors because it is not possible to foresee or ensure what the reactions might be.
Similarly, the patient's expectations of the postoperative result should be realistic in terms of both body contour improvement and its potential impact on their quality of life. Some patients may imagine that the plastic surgery will transform their lives, as if by having a "perfect body" they will be able to do things and achieve goals that had not previously been possible. In this sense, the extent of scarring from these procedures should be exhaustively presented and discussed with the patients, as well as the possibility of enlargements and hypertrophies that will not always be possible to resolve. Skin irregularities and residual sagging are also complications that should be mentioned.
The patient should receive all relevant information in writing during the visit, including the need for multiple procedures, the risk of surgical complications, the time period before which the person can resume work, and the postoperative recovery period. The patient should also receive and sign the consent forms. These steps ensure that the patient's expectations are as realistic as possible with regard to the results of body contouring18.
Self Body Image
For the patient to have realistic expectations of the postoperative outcomes, they must first have an accurate self body image. It is necessary to identify not only how the patient views him or herself, but also how they feel about this view. A good way to do this is to encourage the patient to describe, in their own words, the defects they see in their body contour and how they would like them to be after the surgery. The patient should be able to objectively describe their dissatisfaction and also assign a degree of intensity that can help prioritize their treatment.
The patient's degree of dissatisfaction with their deformities should be consistent with their expectations and the therapeutic possibilities. Patients who focus intensely on their complaints demonstrate an excessively limited vision with regard to their deformities and have high emotional burden or disabling attitudes may be suffering from more severe disorders such as dismorphophobia and may require a specific psychotherapeutic approach before any surgery30.
Psychiatric Status
The plastic surgeon should assess the historical and current psychiatric status of the patient before planning body contour surgery. Patients with deep sadness, especially with neural-negative symptoms of depression (sleeping disorders, appetite, and concentration), should be sent for specialized assessment. Many of them will be or will have been in psychiatric follow-up; thus, contact with the professionals involved can be very helpful in determining the ideal time to start the surgical treatment.
Some patients dissatisfied with their body contouring surgeries have used their preoperative psychiatric condition in legal suits against their surgeons, saying that they were not mentally capable of understanding the consequences and possibilities of the surgery. Therefore, complete documentation of the preoperative psychiatric approach, with reports from specialized professionals, also provides a measure of protection for the plastic surgeon.
Another important aspect of the psychiatric status is the patient's ongoing medication. Antidepressant drugs are often first prescribed by primary care professionals; however, the dose or formulation may not be adequate. Even when medication has been prescribed, the formal approach should be to look for depressive symptoms and mood disorders, then send the patient to a specialist whenever the findings and history are justified.
Similarly, eating disorders such as anorexia, bulimia, and obsessive-compulsive disorder may be present, and misuse of alcohol and drugs is relatively frequent among post-bariatric patients. An accurate diagnosis with specialized management of the possible eating disorders is also essential in preparing for body contouring surgery. This will provide better nutritional support to allow optimal postoperative recovery and to prevent recurrence of obesity12,13.
CONCLUSIONS
Several studies in the medical literature direct attention to the importance of identifying and controlling the psychological conditions of patients throughout treatment for obesity. Ideally, the follow-up should comply with an institutional and multispecialty protocol, with participation of experienced professionals who are able to handle the macro-environment of obese patients and the consequences of their different treatments.
Even when this extended and more complete approach is not available, the plastic surgeon should routinely perform his or her own initial assessment, aiming to identify potential psychological disorders in post-bariatric patients who are candidates for body contouring surgeries. The goal is to collaborate with other professionals in the area to create the best conditions for an optimal surgical outcome for these patients.
REFERENCES
1. Fox KM, Taylor SL, Jones JE. Understanding the bariatric surgical patient: a demographic, lifestyle and psychological profile. Obes Surg. 2000;10(5):477-81.
2. van Hout GC, van Oudheusden I, van Heck GL. Psychological profile of the morbidly obese. Obes Surg. 2004;14(5):579-88.
3. Munoz DJ, Lal M, Chen EY, Mansour M, Fischer S, Roehrig M, et al. Why patients seek bariatric surgery: a qualitative and quantitative analysis of patient motivation. Obes Surg. 2007;17(11):1487-91.
4. Ogden J, Clementi C, Aylwin S, Patel A. Exploring the impact of obesity surgery on patients' health status: a quantitative and qualitative study. Obes Surg. 2005;15(2):266-72.
5. Bloom JMP, Koltz PF, Shaw RB, Gusenoff JA. Prospective assessment of medical and psychiatric comorbidities in the massive weight loss population prior to body contouring surgery. Plast Reconstr Surg. 2010;126:75.
6. Fabricatore AN, Crerand CE, Wadden TA, Sarwer DB, Krasucki JL. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16(5):567-73.
7. Rutledge T, Adler S, Friedman R. A prospective assessment of psychosocial factors among bariatric versus non-bariatric surgery candidates. Obes Surg. 2010;21(10):1570-9.
8. Guisado JA, Vaz FJ, López-Ibor JJ Jr, Rubio MA. Eating behavior in morbidly obese patients undergoing gastric surgery: differences between obese people with and without psychiatric disorders. Obes Surg. 2001;11(5):576-80.
9. Mitchell JE, Lancaster KL, Burgard MA, Howell LM, Krahn DD, Crosby RD, et al. Long-term follow-up of patients' status after gastric bypass. Obes Surg. 2001;11(4):464-8.
10. Wadden TA, Sarwer DB, Arnold ME, Gruen D, O'Neil PM. Psychosocial status of severely obese patients before and after bariatric surgery. Problems Gen Surg. 2000;17:13-22.
11. Allison KC, Wadden TA, Sarwer DB, Fabricatore AN, Crerand CE, Gibbons LM, et al. Night eating syndrome and binge eating disorder among persons seeking bariatric surgery: prevalence and related features. Obesity. 2009;14:77S-82S.
12. Odom J, Zalesin KC, Washington TL, Miller WW, Hakmeh B, Zaremba DL, et al. Behavioral predictors of weight regain after bariatric surgery. Obes Surg. 2010;20(3):349-56.
13. Funnell MM, Anderson RM, Ahroni JH. Empowerment and self-management after weight loss surgery. Obes Surg. 2005;15(3):417-22.
14. Hayden MJ, Dixon JB, Dixon ME, Shea TL, O'Brien PE. Characterization of the improvement in depressive symptoms following bariatric surgery. Obes Surg. 2011;21(3):328-35.
15. Shiri S, Gurevich T, Feintuch U, Beglaibter N. Positive psychological impact of bariatric surgery. Obes Surg. 2007;17(5):663-8.
16. Ashton D, Favretti F, Segato G. Preoperative psychological testing: another form of prejudice. Obes Surg. 2008;18(10):1330-7.
17. Abilés V, Rodríguez-Ruiz S, Abilés J, Mellado C, García A, Pérez de la Cruz A, et al. Psychological characteristics of morbidly obese candidates for bariatric surgery. Obes Surg. 2010;20(2):161-7.
18. van Hout GC, Verschure SK, van Heck GL. Psychosocial predictors of success following bariatric surgery. Obes Surg. 2005;15(4):552-60.
19. Walfish S, Vance D, Fabricatore AN. Psychological evaluation of bariatric surgery applicants: procedures and reasons for delay or denial of surgery. Obes Surg. 2007;17(12):1578-83.
20. Sogg S, Mori DL. The Boston interview for gastric bypass: determining the psychological suitability of surgical candidates. Obes Surg. 2004;14(3):370-80.
21. Lier HO, Biringer E, Stubhaug B, Eriksen HR, Tangen T. Psychiatric disorders and participation in pre- and postoperative counseling groups in bariatric surgery patients. Obes Surg. 2011;21(6):730-7.
22. Mahony D. Psychological assessments of bariatric surgery patients. Development, reliability, and exploratory factor analysis of the PsyBari. Obes Surg. 2011;21(9):1395-406.
23. Kaluf R, Lima Jr. EM, Araújo BGO. Avaliação pré-operatória. In: Lima Jr. EM, ed. Tratado de cirurgia plástica após grandes perdas ponderais. São Paulo: Atheneu; 2010. p. 35-41.
24. Aly AS. Approach to the massive weight loss patient. In: Aly AS, ed. Body contouring after massive weight loss. St. Louis: QMP; 2006. p. 49-56.
25. Rohrich RJ, Kenkel JM. Body contouring after massive weight loss supplement. Plast Reconstr Surg. 2006;117(Suppl.):S1.
26. O'Toole JP, Rubin JP. Evaluation of the massive weight loss patient who presents for body contouring surgery. In: Rubin JP, Matarasso A, eds. Aesthetic surgery after massive weight loss. Philadelphia: Elsevier; 2008. p. 13-20.
27. Sarwer DB, Cohn NI, Gibbons LM, Magee L, Crerand CE, Raper SE, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-56.
28. Sarwer DB. Psychological considerations in cosmetic surgery. In: Goldwyn RM, Cohen MN, eds. The unfavorable result in plastic surgery: avoidance and treatment. 3rd ed. Philadelphia: Lippincott-Raven; 2001. p. 14-23.
29. Resende JHC. Oficina da obesidade em cirurgia plástica ou oficina da vida. In: Resende JHC, ed. Tratado de cirurgia plástica na obesidade. Rio de Janeiro: Rubio; 2008. p. 239-44.
30. Sarwer DB, Thompson JK, Mitchell JE, Rubin JP. Psychological considerations of the bariatric surgery patient undergoing body contouring surgery. Plast Reconstr Surg. 2008;121(6):423e-34e.
1. Former resident in the Plastic Surgery Service of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
2. Psychologist in the Bariatric Surgery Service of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
3. Professor and assistant physician of the Discipline of Plastic Surgery of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
4. Full professor and head of the Bariatric Surgery Service of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
5. Head of the Plastic Surgery Service of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
Correspondence to:
Flavio Henrique Mendes
Rua Cláudio Manoel da Costa, 65
Lins, SP, Brazil - CEP 16400-464
E-mail: mendesmd@fhmendes.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástic /Brazilian Journal of Plastic Surgery).
Paper received: March 30, 2010
Paper accepted: August 14, 2011
Study conducted at the Plastic Surgery Service of the School of Medicine of Botucatu, Botucatu, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket