



Original Article - Year 2011 - Volume 26 -
Surgical treatment of retracted columella in primary noses
Tratamento cirúrgico da columela retraída em narizes primários
ABSTRACT
BACKGROUND: Retracted columella may be present in primary noses as well as in patients who have undergone aesthetic or functional rhinoplasty. This study aims to demonstrate the use of the labial portion of the depressor septi nasi (the depressive muscle of the nasal tip) and upper lip orbicularis muscle for retracted columella correction.
METHODS: The subjects included 20 patients between 20 and 35 years old (4 males and 16 females) who underwent primary aesthetic rhinoplasty.
RESULTS: Moderate edema was observed postoperatively in all patients and was resolved within 1 to 3 months. V-shaped scars at the base of the columella presented excellent aesthetic aspects.
CONCLUSIONS: The surgical technique is easy and the learning curve is fast. Columella correction with the presented technique provides natural and predictable results.
Keywords: Rhinoplasty. Nose/surgery. Plastic surgery/methods.
RESUMO
INTRODUÇÃO: A columela retraída pode estar presente em narizes primários e em pacientes já submetidos a rinoplastias estéticas e/ou funcionais. O objetivo deste trabalho é demonstrar a utilização do músculo depressor do septo nasal (músculo depressor da ponta nasal) em sua porção labial e do músculo orbicular do lábio superior na correção da columela retraída.
MÉTODO: No total, 20 pacientes com idades variando entre 20 anos e 35 anos, sendo 4 do sexo masculino e 16 do sexo feminino, foram submetidos a rinoplastia estética primária.
RESULTADOS: Presença de edema moderado pós-operatório foi observada em todos os casos, com resolução dentro de 1 mês a 3 meses. As cicatrizes em "V" na base da columela apresentaram excelente aspecto estético.
CONCLUSÕES: A técnica cirúrgica é de fácil execução e apresenta curva de aprendizado rápida. A correção da columela com a técnica apresentada proporcionou resultados naturais e previsíveis.
Palavras-chave: Rinoplastia. Nariz/cirurgia. Cirurgia plástica/métodos.
Retracted columella occurs when the posterior two thirds of the columella are not correctly projected and are inferior to the alar margin, obscuring their visibility especially in the profile position1-3.
According to Günter et al.2 and Sperli et al.4, it is necessary to first establish if the problem is in the columella - i.e., if it is really retracted or if it is normal and only appears to be retracted due to protrusion of the nasal alar. In addition, Günter et al.2 and Sperli et al.4 clarified the relationship between the columella and alar margin (Figure 1).
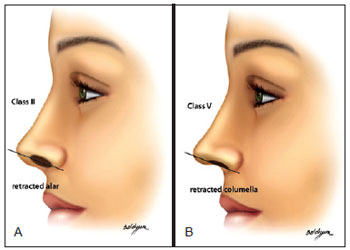
Figure 1 - In A, normal columella. In B, hidden columella.
Retracted columella may be present in primary and secondary noses subjected to aesthetic or functional rhinoplasties as a result of excessive and/or unnecessary resections of the caudal portion of the septal cartilage.
Once the diagnosis is established, the retracted columella should be projected so that its posterior two thirds are properly projected, inferior to the alar margin.
Cartilaginous grafts (e.g., septal cartilage, auricular cartilage, and the cranial portion of the lateral branches of alar cartilages) and muscle flaps can be used for retracted columella correction5-10.
This study aims to demonstrate the use of the labial portion of the depressor septi nasi (the depressive muscle of the nasal tip) and the upper lip orbicularis muscle for retracted columella correction.
METHODS
A prospective study was performed on 20 patients that were candidates for primary aesthetic rhinoplasty. All patients had noses with retracted columella. The patients ranged in age from 20 to 35 years old, including 4 males and 16 females.
In 7 patients, local anesthesia was used, and sedation was carried out by an anesthesiologist. In the other 13 patients, general anesthesia and local anesthesia were administered.
Surgeries were performed between 1990 and 2008 in private clinics and at the Integrated Services of Plastic Surgery of Hospital Ipiranga.
Surgical Anatomy
The muscle-ligament complex of the nose, which involves the nasal and depressor septi/tip muscles as well as Pitanguy's ligament, was studied in detail by Sperli et al.4. The muscle is classified as atrophic, normal, or hypertrophied (Figure 2). In this study, it was possible to verify that this complex can be divided into 3 parts: the base, body, and extremity (Figure 3). In the present study, the muscle-ligament complex base of the nose and part of the lip orbicularis muscle were used.
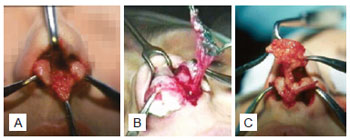
Figure 2 - In A, atrophic muscle. In B, normal muscle. In C, hypertrophied muscle.
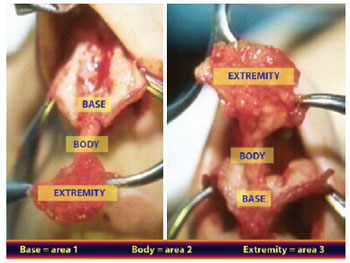
Figure 3 - Muscle-ligament complex divided into 3 areas: base, body, and extremity.
Surgical Technique
An exo-rhinoplasty was performed using an open technique with a V-shaped transcolumellar incision at the columella base (Figure 4) at the angle defined by the nose and upper lip.
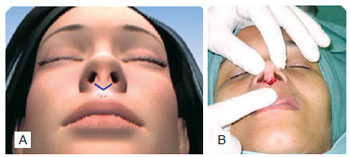
Figure 4 - Exo-rhinoplasty with open technique. In A, schematic marking. In B, incision at the columella base.
Upon preparing the flap, area 1 of the depressor septi/tip and part of the upper lip orbicularis muscle were dissected, making a detachment from the incision edges at the V-shaped incision of the columella base; this was done to identify the orbicularis muscles of the upper lip and labial portion of the nasal tip depressor muscle (Figures 5 and 6).

Figure 5 - Flap production. In A, schematic dissection of the muscle. In B, scheme demonstrating the released muscle. In C, scheme demonstrating the folded muscle.

Figure 6 - Flap production. In A, muscle dissection. In B, released muscle. In C, folded muscle.
The flap was marked in order to be pedicled at the columella base and to have dimensions of approximately 1.3-cm long and 0.6-cm wide.
Then, lateral and inferior incisions were made, elevating the flap with approximately one third of the thickness of the lip muscles. This makes it possible to decrease the flap volume according to the desired projection.
Next, the flap was sutured with 3 simple sutures of 6-0 mononylon, folding and fixing it to the medial branches of the alar cartilages, thus achieving the columella projection.
After fixing the flap in patients with an enlarged alar base, an approximation of the muscle edges resulting from the flap's donor area was performed with 1 or 2 inverted 4-0 mononylon sutures. In patients with a normal alar base width, approximation of the muscle edges was not performed.
The V-shaped incision suture at the columella base was made with simple 4-0 mononylon sutures, and marginal incisions were made with simple catgut 4-0.
RESULTS
All patients exhibited moderate edema postoperatively. In addition, the patients had impressions of hypercorrection of the retracted columella that normalized with gradual regression of the edema between 8 and 15 days after the procedure.
Flap fixation to the medial branches of the alar cartilages did not produce caudal traction of the nasal tip in either aesthetic or dynamic assessments during the postoperative follow-up.
The use of the orbicularis muscle did not cause any type of sequelae in the upper lip such as local retraction, sensitivity, or motor alterations.
The V-shaped scars at the base of the columella had excellent aesthetic aspects.
Figures 7 to 12 illustrate some cases among this case selection.

Figure 7 - Patient 1. In A and B, preoperative period. In C and D, postoperative period.

Figure 8 - Patient 2. In A and B, preoperative period. In C and D, postoperative period.

Figure 9 - Patient 3. In A, preoperative period. In B, postoperative period.
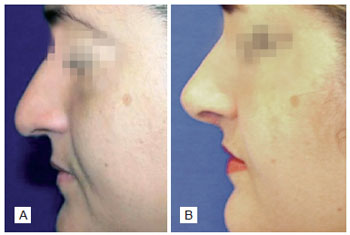
Figure 10 - Patient 4. In A, preoperative period. In B, postoperative period.

Figure 11 - Patient 5. In A, preoperative period. In B, postoperative period.
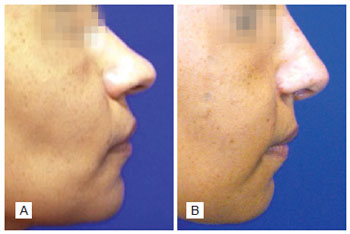
Figure 12 - Patient 6. In A, preoperative period. In B, postoperative period.
DISCUSSION
The technique utilizing the labial portion of the depressor septi muscle and upper lip orbicularis muscle for retracted columella correction is easy to implement and has a rather easy learning curve.
There is no need for columella hypercorrection, and the flap should have a sufficient volume to naturally project the columella in a natural manner at the end of the surgery.
It was more difficult to implement the technique in patients that did not require nasal tip treatment than in cases where marginal incisions were complete.
In cases where nasal tip treatment was required, more intense and persistent edema in the columella due to tip treatment was observed.
Approximation of the lateral edges of the lip orbicularis muscle at the flap's donor area resulted in slight thinning of the alar base. Moreover, previously scheduled nasal alar resection was unnecessary in some cases.
Orbicularis muscle edge approximation is unnecessary and should not be performed in patients with a normal alar base because it may cause nasal clamping, altering the external nasal valve.
In patients with retracted and short columella, a V-shaped incision was made at the upper lip with the aim of lengthening the columella.
The upper lip should have sufficient muscle for flap production; therefore, this technique cannot be used in patients with a short lip.
CONCLUSIONS
The technique for retracted columella correction using the labial portion of the depressor septi nasal muscle and upper lip orbicularis muscle produces natural and predictable results, and is easy to perform.
REFERENCES
1. Tebbetts JB. Complexo lábio-columelar. In: Tebbetts JB, ed. Rinoplastia primária: a nova abordagem lógica das técnicas. Rio de Janeiro: Di-Livros; 2002. p. 453-83.
2. Gunter JP, Rohrich RJ, Friedman RM. Classification and correction of alar-columellar discrepancies in rhinoplasty. Plast Reconstr Surg. 1996;97(3):643-8.
3. Mottura AA. Short columella nasolabial complex in aesthetic rhinoplasty. Aesthetic Plast Surg. 2001;25(4):266-72.
4. Sperli AE, Prado Neto JM, Pitombo V. Refinamentos em rinoplastia: uma visão atual. Rio de Janeiro: Di-Livros; 2009.
5. Cachay-Velásquez H. Rhinoplasty and facial expression. Ann Plast Surg. 1992;28(5):427-33.
6. Cronin TD. Lengthening columella by use of skin nasal floor and alae. Plast Reconstr Surg Transplant Bull. 1958;21(6):417-26.
7. Shin KS, Lee CH. Columella lengthening in nasal tip plasty of Orientals. Plast Reconstr Surg. 1994;94(3):446-53.
8. Rees TD. Unique problems associated with the lip-columella-tip complex: rhinoplasty problems and controversies. Aesthetic Plast Surg. 1988;12:118.
9. Rohrich R, Huynh B, Muzaffar AR, Adams WP Jr., Robinson JB Jr. Importance of the depressor septi nasi muscle in rhinoplasty: anatomic study and clinical application. Plast Reconstr Surg. 2000;105(1):376-83.
10. Santana PS. Treatment of the Negroid nose without nasal alar excision: a personal technique. Ann Plast Surg. 1991;27(5):498-507.
1. Full member of the Brazilian Society of Plastic Surgery (SBCP), head of the Integrated Plastic Surgery Services of Hospital Ipiranga, São Paulo, SP, Brazil.
2. Head physician of Integrated Plastic Surgery Services of Hospital Ipiranga, São Paulo, SP, Brazil.
3. Full member of the SBCP, plastic surgeon of the Integrated Plastic Surgery Services of Hospital Ipiranga, São Paulo, SP, Brazil.
Correspondence to:
Aymar Sperli
Rua Pedro de Toledo 129 - cj. 11/12
São Paulo, Brazil - CEP 04039-030
E-mail: aymar.sperli@uol.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Paper received: August 6, 2011
Paper accepted: October 17, 2011
Study conducted at Integrated Services of Plastic Surgery of Hospital Ipiranga, São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket