



Case Reports - Year 2011 - Volume 26 -
Treatment of umbilical stenosis in a vertical dermolipectomy patient
Tratamento da estenose umbilical em paciente com dermolipectomia vertical
ABSTRACT
Introduction: Unaesthetic revision of the umbilical scar in vertical abdominoplasty is a common reason for patient dissatisfaction. Case Report: We propose the use of the opposite triangular-flap technique, an omphaloplasty technique that we developed, to treat and prevent recurrence of stenosis by insertion of two triangular flaps on the umbilical stump. After describing our initial use of this technique to treat a case of umbilical stenosis after vertical dermolipectomy, we explain why the positive outcomes that we observed in this case motivate us to recommend further use of this technique, primarily in vertical abdominoplasty.
Keywords: Constriction, Pathologic. Umbilicus/surgery. Reconstructive Surgical Procedures/methods. Cicatrix/pathology/surgery.
RESUMO
Introdução: As alterações inestéticas da cicatriz umbilical em abdominoplastias verticais são frequentes fatores de insatisfação com os resultados. Relato de Caso: Apresentamos neste artigo um caso de estenose umbilical em paciente com dermolipectomia vertical prévia, no qual utilizamos dois retalhos laterais interpolados ao coto umbilical, para o tratamento e a prevenção da recidiva, os quais designamos técnicas dos retalhos triangulares opostos. O resultado estético obtido nos incentivou a indicá-la como técnica primária de onfaloplastia nestes casos.
Palavras-chave: Constrição Patológica. Umbigo/cirurgia. Procedimentos Cirúrgicos Reconstrutivos/métodos. Cicatriz/patologia/cirurgia.
Prevention of umbilical scarring to the greatest extent possible remains a challenge in abdominoplasty. Unsightly scarring, particularly that due to hypertrophy or stenosis, can result in patient dissatisfaction. In our experience, dissatisfaction occurs more frequently among patients who experience median scarring after undergoing omphaloplasty, which often leads to stenosis due to scar contracture because it is performed circumferentially.
Several techniques that prevent or reduce umbilical scarring have been proposed for producing aesthetically pleasant outcomes in omphaloplasty and neo-omphaloplasty1-6. Although several of these techniques, such as the Avelar technique, have been established, few have been specifically indicated for vertical dermolipectomy. One of the few indicated for vertical dermolipectomy, the construction of a neoumbilicus with side flaps in patients with vertical scarring, was described by Franco et al. as yielding satisfactory results5.
We describe the treatment of a case of umbilical stenosis in a post-bariatric patient on whom we had performed complementary vertical dermolipectomy using an omphaloplasty technique that we developed specifically for this case. Using what we have termed the opposing triangular-flap technique, an omphaloplasty technique that we based on the work of Talita, we interpolated two lateral triangular flaps to the flaps of the patient's umbilical scar (Figure 1).
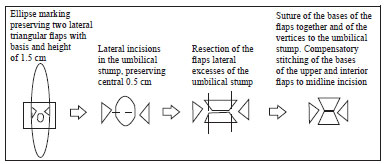
Figure 1 - Scheme of the major steps of the opposing triangular-flap technique.
CASE REPORT
Figure 2 shows the umbilical stenosis, widened hypertrophic scarring, and pubic ptosis experienced by the patient discussed here during the late postoperative stage after undergoing bariatric surgery and anchor-line abdominal dermolipectomy. We proposed treating this patient by revising the vertical dermolipectomy via repositioning of the horizontal line, correction of the pubic ptosis, and plication of the rectoabdominal muscles. Anticipating a lack of tissue when attempting to correct the umbilical stenosis, we preserved two triangular flaps for interpolation to the umbilical stump after resectioning of the stenosis ring.
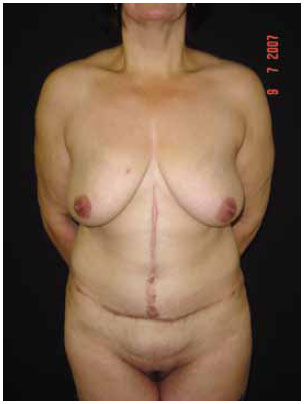
Figure 2 - Preoperative view showing hypertrophy, poorly positioned scars, and umbilical stenosis.
Surgical Technique
We performed vertical and horizontal ellipse marking to preserve two lateral triangular flaps with a base and length of 1.5 cm at the level of the umbilicus (Figure 3). Performing routine infiltration with 1:500,000 epinephrine solution at all incisions, we resected the marked flap, plicated the rectoabdominal muscles, and sutured all incisions except those in the umbilical region. We then repaired the umbilical stump by making one horizontal incision of a length of 1.5 cm on each side without transfixation to obtain two opposing triangular flaps (i.e., a top and a bottom flap). After excising excess skin from the umbilical stump, located at the vertices of the base of both triangles, we repaired the vertices of the side flaps with U-shaped stitches. After interpolating the side flaps to the flaps of the umbilical stump, we sutured the flaps together and completed suturing the incision. When, due to skin redundancy, we experienced difficulty in suturing between the supra- and infraumbilical midline incision and the respective top and bottom edges of the flaps of the umbilical stump, we performed compensatory stitching (Figure 1). Our experience indicates that it is possible to excise additional skin from the umbilical stump when necessary.
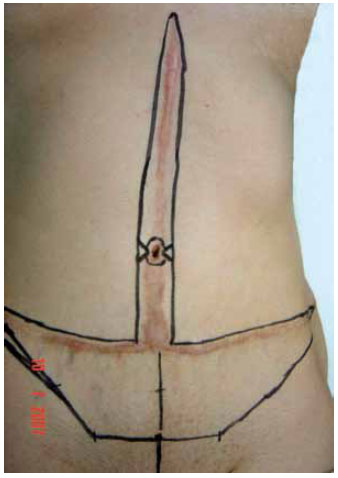
Figure 3 - Preoperative markings.
The outcome of our procedure was the effective treatment of umbilical stenosis, as evidenced by its lack of recurrence during a 1-year period of post-operative ambulatory care, as well as satisfactory aesthetic outcomes (Figures 4 and 5).

Figure 4 - Postoperative outcome.

Figure 5 - Magnified image of the postoperative umbilical scar.
DISCUSSION
After performing vertical or anchor-line abdominoplasty, we frequently observed the formation of hypertrophic or unaesthetic umbilical scarring, primarily resulting from scar contraction after circumferential omphaloplasty. It is common knowledge that a "break" in the scar line can be minimized by geometric patching or even zetaplasty to obtain more aesthetically pleasing results. The opposing triangular-flap technique that we propose is simply the application of this concept of scar breaking by the interpolation of flaps to correct umbilical stenosis in vertical dermolipectomy.
Common treatment options in vertical or anchor-line abdominoplasty are the revising of the scar or the crafting of a neoumbilicus. In our view, scar revision is unsatisfactory because the circular scar is maintained, while neo-omphaloplasty, despite yielding better cosmetic results, is more complex, and is unnecessary or overindicated in cases of umbilical stenosis restricted to its distal end. Therefore, we assert that neo-omphaloplasty should be indicated cautiously, even in cases of partial umbilical necrosis, and primarily used to treat cases of mild or moderate umbilical or incisional hernia. In these cases, we have successfully performed omphaloplasty using the technique described by Avelar, or even using the opposing triangular-flap technique, to obtain a less skeletized umbilical stump. We have also performed hernia repair by vertical incision over the hernia without detachment of the aponeurosis.
In our use of the opposing triangular-flap technique in this case, we observed beneficial outcomes in terms of increased aesthetic quality, primarily due to prevention of side scarring on the umbilicus, as well as reduced risk of stenosis recurrence, decreased tension over the median scar, reproducibility, and location of the scars over pre-existing scars. Encouraged by these positive outcomes, we began indicating use of this technique, primarily in vertical dermolipectomy, and, after observing the same beneficial outcomes, now routinely use it in these cases (Figures 6 to 9).

Figure 6 - Preoperative view of the dermolipectomy and primary application of the proposed omphaloplasty technique.

Figure 7 - Postoperative umbilical scar detail.

Figure 8 - Preoperative view of dermolipectomy revision and umbilical hernia correction by application of the opposing triangular-flap technique.

Figure 9 - Postoperative view.
CONCLUSION
We successfully treated a case of umbilicus stenosis using the opposing triangular-flap technique, a novel omphaloplasty technique by which we interpolated lateral flaps to the flaps of the umbilical stump. Based on our results, we recommend use of this technique, particularly to treat cases of vertical dermolipectomy aiming at cosmetic improvement with no significant navel scarring.
REFERENCES
1. Yotsuyanagi T, Nihei Y, Sawada Y. A simple technique for reconstruction of the umbilicus, using two twisted flaps. Plast Reconstr Surg. 1998;102(7):2444-6.
2. Malic C, Spyrou GE, Hough M, Fourie L. Patients satisfaction with two different methods of umbilicoplasty. Plast Reconstr Surg. 2007;119(1):357-61.
3. Shinohara H, Matsuo K, Kikuchi N. Umbilical reconstruction with an inverted C-V flap. Plast Reconstr Surg. 2000;105(2):703-5.
4. Sevin A, Sevin K, Senen D, Erdogan B. A new method for umbilicus reconstruction: preliminary report. Aesthetic Plast Surg. 2006;30(5):589-91.
5. Franco D, Medeiros J, Farias C, Franco T. Umbilical reconstruction for patients with a midline scar. Aesthetic Plast Surg. 2006;30(5):595-8.
6. Masuda R, Takeda A, Sugimoto T, Ishiguro M, Uchinuma E. Reconstruction of the umbilicus using a reverse fan-shaped flap. Aesthetic Plast Surg. 2003;27(5):349-53.
Plastic Surgeon, Associate Member of the Brazilian Society of Plastic Surgery, Porto Alegre, RS, Brazil.
Corresponding author:
André Luis Rosenhaim Monte
Rua Padre Chagas, 185 - cjto. 1102 - Moinhos de Vento
Porto Alegre, RS, Brazil - CEP 90570-080
E-mail: alrmonte@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: July 10, 2009
Accepted: May 16, 2010
Work performed at the author's private clinic, Porto Alegre, RS, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket