



Case Reports - Year 2011 - Volume 26 -
Intraoperative skin traction for wound closure following hygienic bilateral mastectomy: a case report
Tração cutânea intraoperatória para fechamento de ferida após mastectomia bilateral higiênica: relato de caso
ABSTRACT
Introduction: Post-mastectomy chest wall defects require reconstruction using a safe and efficient procedure. In cases of local relapse, especially bilateral relapse, the surgical intervention indicated should be based on assessment of the patient's general condition and life expectancy. One such intervention, intraoperative skin traction, has been found to offer the benefits of rapid execution and low morbidity while reducing the scar formation associated with the use of skin flaps. Case Report: Hygienic bilateral mastectomy with dissection of the left axillary lymph nodes was performed on a 45-year-old woman after diagnosis of a relapsed tumor in the right breast and a new tumor in the left one. Based on the assessment of the general state of the patient, intraoperative skin traction of the wound edges was chosen for primary closure of the chest wall. Traction was performed according to the procedure described by Góes et al., which involved using Prolene 2-0 sutures, stretching the skin for 10 minutes, relaxation of the skin for two minutes, until the wound edges are sufficiently proximate to each other to perform primary suturing. This was achieved after three cycles of tension and relaxation. The procedure lasted two hours, and aspiratory drainage was performed with a Portovac 3.2 drain, which was removed after 7 days. The patient did not report pain or experience suture dehiscence or any other complications. Conclusion: In traoperative skin traction is a safe, functionally efficient, low-cost, and low-morbidity technique for wound closure following hygienic bilateral mastectomy.
Keywords: Skin. Traction. Mastectomy. Breast/surgery.
RESUMO
Introdução: As sequelas da parede torácica após mastectomia requerem reconstrução por meio de conduta segura e eficiente. Nos casos de recidiva local, sobretudo bilateral, a intervenção cirúrgica deverá ser indicada considerando o estado geral do paciente e a expectativa de vida. A tração intraoperatória é uma técnica de baixa morbidade e rápida execução, reduzindo as cicatrizes decorrentes da utilização de retalhos. Relato do Caso: Paciente do sexo feminino, 45 anos que, após diagnóstico de recidiva tumoral em mama direita e novo tumor em mama esquerda, foi submetida à mastectomia bilateral higiênica com esvaziamento axilar à esquerda. Optou-se pela realização de tração cutânea intraoperatória dos bordos da ferida para fechamento primário da parede torácica devido ao estado geral da paciente. A tração foi realizada conforme a técnica de Góes et al., utilizando-se fios de prolene 2, tracionando a pele por dez minutos, com descanso de dois minutos, até que se obtivesse proximidade suficiente dos bordos das lesões para realização de sutura primária, o que foi alcançado após três ciclos de tração e relaxamento. O procedimento teve duração de duas horas, e foi colocado dreno portovac 3.2, que foi retirado após 7 dias. A paciente evoluiu sem queixas álgicas, sem deiscência ou qualquer outra complicação. Conclusão: A tração intraoperatória demonstrou ser uma técnica segura, funcionalmente eficaz, com menores custo e morbidade, para fechamento de ferida resultante de mastectomia bilateral higiênica.
Palavras-chave: Pele. Tração. Mastectomia. Mama/cirurgia.
Post-mastectomy chest wall defects require reconstruction using a safe and efficient procedure. In cases of local relapse, especially bilateral relapse, the surgical intervention indicated should be based on assessment of the patient's ge neral condition and life expectancy. One such intervention, intraoperative skin traction, offers the advantages of rapid exe cution and low morbidity while reducing the scarring asso ciated with the use of skin flaps.
CASE REPORT
A 45-year-old female patient with a history of treated gas tric and uterine cervix cancer underwent right mastectomy and reconstruction with the use of an expander in September 2008. After diagnosis of a relapsed tumor in the right breast and of a new tumor of the left breast in June 2009, she un derwent bilateral mastectomy with hygienic left axillary dissection, removal of the expander, and resectioning of the major and minor pectoral muscles on the right breast with clear evaluation of margins by frozen section (Figure 1).

Figure 1 - The wound following bilateral hygienic mastectomy.
Based on assessment of the patient's condition, we de cided to perform intraoperative skin traction of the wound margins for primary closure of the chest wall according to the traction method developed by Garcia et al.1. According to this procedure, a Prolene 2-0 suture is inserted with a 7.5 cm needle in an area posterior to the minimal detachment, thereby externalizing it on the inside of the wound toward the opposite margin, where approximately 1 cm of the border transfixes the flap, followed by capping of the thread through the needle with a catheter section. The process is then reversed, by penetrating the needle at the end of the detachment and ex ternalizing it as far as possible from the detachment to complete a U-shape. The procedure is performed bilaterally by simultaneously pulling the two threads on each side in opposite directions to promote an approximation of wound edges up to the point of maximum tension. When that point is reached, the tension is maintained by clamping the ends of the threads close to the skin using four Kelly clamps. After 10 minutes, the Kelly clamps are removed to relax the tension for 60 seconds (Figure 2), after which another traction is performed. This cycle is repeated until the wound edges are sufficiently proximate to one another to perform primary suturing (Figure 3) without maintaining tension using Monocryl 4.0 (subdermal) and Mononylon 4.0 (separate simple) sutures.
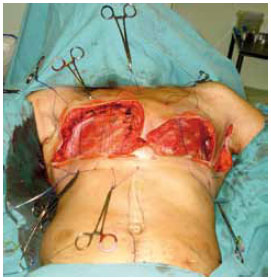
Figure 2 - Relaxation of the edges for 2 minutes after traction with Prolene 2-0 sutures.

Figure 3 - The closed wound following 3 cycles of traction.
By following this procedure, we achieved wound closure after three cycles of traction. During the approximately two-hour procedure, we performed aspiratory drainage using a Portovac 3.2 drain, which was removed after seven days. After completion of the procedure, the patient neither complained of pain nor experienced suture dehiscence or any other complication (Figure 4).

Figure 4 - The scar 3 weeks after the operation.
DISCUSSION
Intraoperative skin traction by rapid stretching based on consideration of the viscoelastic properties of the skin offers a simpler solution for suturing complex wounds with less morbidity compared to the use of grafts, expanders, or local or free flaps2. Moreover, as this technique does not require expensive equipment, it offers the benefits of reduced hospitalization and treatment costs. Large detachment of the edges of the wound is not recommended due to the increased risk of complications3. There are no reports on the use of skin traction for bilateral mastectomies.
Our use of intraoperative skin traction in the present case met the functional requirements for hygienic mastectomy4. Specifically, the use of this technique provided sufficiently dense cover tissue of adequate volume and quality, prevented the formation of "dead space" or collations, prevented the development of infection or chest restriction by scar fibrosis, and resulted in static and functional stability of the rib cage without valvulation or pulmonary restriction.
CONCLUSION
Intraoperative skin traction is a safe, functionally efficient, low-cost, and low-morbidity technique for wound closure following bilateral hygienic mastectomy.
REFERENCES
1. Góes CHFS, Kawasaki MC, Mélega JM. Fechamento de feridas por tração cutânea intra-operatória: análise de 23 casos. Rev Soc Bras Cir Plast. 2004;19(2):63-74.
2. Hirshowitz B, Lindenbaum E, Har-Shai Y. A skin-stretching device for the harnessing of the viscoelastic properties of skin. Plast Reconstr Surg. 1993;92(2):260-70.
3. Molea G, Schonauer F, Blasi F. Progressive skin extension: clinical and histological evaluation of a modified procedure using Kirschner wires. Br J Plast Surg. 1999;52(3):205-8.
4. Mendes FH, Freitas AG, Mélega JM. Reconstrução das sequelas de mastectomia e radioterapia. In: Melega JM, Montoro AF, eds. Cirurgia plástica fundamentos e arte: cirurgia reparadora de tronco e membro. Rio de Janeiro:Medsi;2004. p.104-8.
1. PhD in Medical Sciences, Faculty of Medicine, University of São Paulo; full Member of the Brazilian Society of Plastic Surgery (SBCP); Assistant at the Santa Cruz Plastic Surgery Institute, São Paulo, SP, Brazil.
2. PhD Student in Medical Sciences, Faculty of Medicine, Ribeirão Preto - University of São Paulo; Associate SBCP Member; Plastic Surgeon at Máster Hospital, Goiânia, GO, Brazil.
3. Aspirant SBCP Member-in-Training; Resident at the Santa Cruz Plastic Surgery Institute, São Paulo, SP, Brazil.
Corresponding author:
Rodrigo Gouvea Rosique
Av. Caramuru, 2100 - apto 1103 - República
Ribeirão Preto, SP, Brazil - CEP 14030-000
E-mail: gruguim@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: July 24, 2009
Accepted: September 18, 2009
Work performed at the Instituto de Cirurgia Plástica Santa Cruz (ICPSC) - (Santa Cruz Institute of Plastic Surgery - ICPSC), São Paulo, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket