



Original Article - Year 2011 - Volume 26 -
Abdominoplasty with liposuction and minimal undermining
Abdominoplastia com lipoaspiração e descolamento mínimo
ABSTRACT
The paper describes a method for combining abdominoplasty and liposuction while preserving the abdominal blood supply and lymphatic drainage. The method involves a modification of the vascular-preservation technique: namely, two triangular segments of the lateral infraumbilical transverse fascia are retained and the medial infraumbilical segment is resected, enabling broad and adequate plication of the rectus abdominis fascia and partial pubectomy. This modification ensures improved cosmetic results compared with the classical approach and allows the additional benefit of extensive liposuction of all parts of the abdomen and flanks, improving the procedural outcome and reducing the incidence of complications such as seromas.
Keywords: Abdomen/surgery. Abdominal wall/surgery. Lipectomy. Plastic surgery/methods.
RESUMO
O autor descreve sua metodologia, em abdominoplastia associada à lipoaspiração, utilizando os princípios de manutenção da vascularização e da drenagem linfática do abdome. Introduz uma modificação na preservação do sistema vascular, mantendo dois triângulos de fáscia superficial lateral e a ressecção do segmento medial infraumbilical, que permite uma plicatura ampla e adequada da fáscia muscular abdominal, bem como uma pubectomia parcial (PP). Esta modificação tem sido importante para a obtenção de resultados estéticos semelhantes àqueles conseguidos com a técnica clássica, acrescidos do benefício de uma lipoaspiração ampla, em toda a extensão do abdome e flancos, melhorando o resultado final, e reduzindo a incidência de complicações.
Palavras-chave: Abdome/cirurgia. Parede abdominal/cirurgia. Lipectomia. Cirurgia Plástica/métodos.
From 1980 onward, the classical abdominoplasty technique1,2, involving full undermining, without liposuction and with plication of muscular diastasis3,4 was applied at the ArtClinic (Fortaleza, CE, Brazil). The procedure was performed carefully to avoid compromising the blood circulation and aspirating the abdominal flap5. Although drainage was systematically maintained for 48 h, as in the classical technique6, a high incidence of seromas was noted. Further, secondary liposuction was frequently required 6 months after the abdominoplasty procedure. The combination of abdominoplasty and liposuction of the abdominal flap was considered a high-risk procedure leading to complications such as skin necrosis.
Since 2001, abdominoplasty with liposuction1,7 and minimal central undermining has been applied to allow efficient correction of the abdominal muscular diastasis, good visibility of the muscular fascia8, and maintenance of the musculocutaneous circulation and lateral infraumbilical transverse fascia, which plays an important role in accessory circulation and lymphatic drainage. Plication of the muscular fascia prevents the formation of a dead space and thus avoids the need for drainage.
This paper describes a new method for combining abdominoplasty and liposuction by resection of the medial infraumbilical segment, which not only facilitates the plication of the muscular fascia but also reduces the amount of infraumbilical vascularized connective tissue, ensuring cosmetic results.
METHODS
Between June 2001 and July 2010, 483 abdominoplasties, including 480 procedures in women and 3 procedures in men, were performed on patients aged 24-61 years at the ArtClinic (Fortaleza, CE, Brazil). The procedures involved 418 full abdominoplasties (surgical removal of the whole infraumbilical skin; Figure 1A), 35 miniabdominoplasties (minimal suprapubic skin excision without umbilical incision and scarring limited to the pubic region; Figure 1B), and 30 midabdominoplasties (broader skin excision than in miniabdominoplasty, extending laterally to the pubis, but less than in full abdominoplasty and without umbilical incision; Figure 1C).
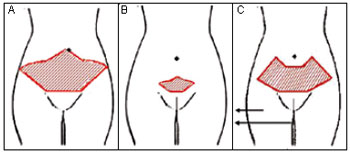
Figure 1 - A: Full abdominoplasty, B: miniabdominoplasty, and C: midabdominoplasty.
Surgical Techniques
Full abdominoplasty: Preoperatively, the locations for liposuction, including the dorsal flanks and anteroposterior sites, were demarcated while the patients were standing. After the administration of general anesthesia, the reference sites were demarcated while the patients lay in the dorsal position (Figure 2). Initially, the pubis was demarcated and a line was extended to follow the lower abdominal groove, through the laterals, toward the line for the pubic incision. The pubic incision was designed to ensure a pubis of adequate size (~5-6 cm), which mostly necessitated partial pubic resection (partial pubectomy). Then, the umbilical incision was drawn in a lozenge shape, comprising two straight lines from the top of the navel that covered an area of the same width as the pubis (Figure 2). The demarcation delimiting the upward curves were complimented from the lateral end of the latter straight line segments to the end of the lateral lines (Figure 2). Thereafter, the excision area of the skin and subcutaneous tissue was defined in the medial infraumbilical region (Figures 2 and 3A), lying between two oblique lines starting from the top edges of the line segments and converging at a point 2 cm from the center of the pubis. This demarcation created three areas in the lower abdomen: two triangular segments of the lateral infraumbilical transverse fascia (Figures 2 and 3B) and a medial infraumbilical segment.
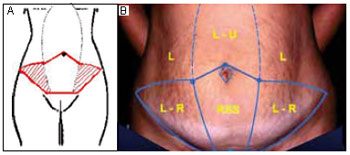
Figure 2 - A: Sketch showing the infraumbilical resection of subcutaneous tissue and muscular fascia ready for plication. B: Surgical planning. L, liposuction; L-U, liposuction and detachment; LR, liposuction and skin resection; RSS, resection of skin and subcutaneous tissue.
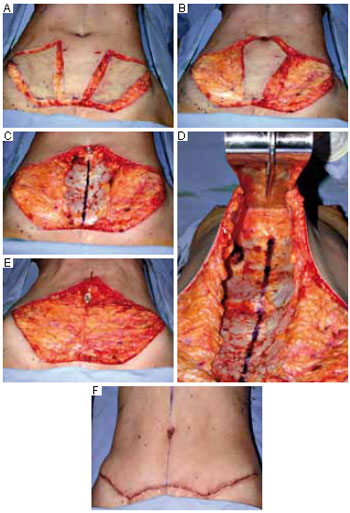
Figure 3 - A: Before the surgery, the sites for liposuction and incision of the lateral flaps of the abdomen are demarcated. B: Excision of the whole skin of the lateral flaps of the abdomen while keeping the superficial fascia intact. C: Resection of the medial infraumbilical skin, exposing the muscular fascia and preserving the superficial fascia in the lateral areas. D: Tunnel undermining for plication of the navel up to the xiphoid appendix. E: Conclusion of the plication while preserving the entire lymphatic system and vasculature. F: Final result with good body delineation.
All patients received a saline injection with epinephrine (1:500,000) to reduce blood loss. The operation began with liposuction of the entire abdomen according to previously described criteria9. A greater degree of liposuction was performed under the skin to be resected than in other areas. Next, the entire skin of the lateral triangular segments was removed (Figure 3B), while paying attention to the excision of all attachments and maintaining the transverse fascia and its blood supply and lymphatic drainage (Figures 3B and 3C). The medial infraumbilical segment was resected (Figures 2 and 3A), resulting in partial pubectomy. Then, the navel was incised along with sufficiently wide supraumbilical subcutaneous undermining to perform plication, according to each case (Figure 3D). Plication for treating diastasis of the rectus abdominis was performed by using double mononylon 0 sutures with separate stitches. The preserved lateral infraumbilical transverse fascia was automatically approximated by the muscular plication. If necessary, the superficial fascia and lower abdominal connective tissue were plicated, while maintaining the accessory vasculature (inferior epigastric and superficial circumflex iliac vessels) and lymphatic vessels in this area (Figure 3E). Finally, with the patient in the flexed position, the wound was closed with 5 main mononylon 0 stitches in the pubic region followed by nylon or colorless Monocryl 3-0 sutures and Dermabond (Figure 3F). The navel was sutured with nylon 4-0 (Figure 4).

Figure 4 - A and C: Preoperative planning for full abdominoplasty. B and D: Postoperative condition 6 months later.
Miniabdominoplasty and midabdominoplasty: In the miniabdominoplasty (Figure 5) and midabdominoplasty procedures (Figure 6), the same approach as in full abdominoplasty but with less skin resection was applied, according to each case (Figures 1B, 1C, 6, and 7). Drains were not placed, and the surgical site was covered with padded gauze and elastic strap.

Figure 5 - A and C-E: Preoperative and intraoperative steps for miniabdominoplasty. B and F: Postoperative condition 6 months later.
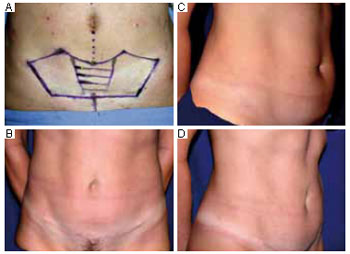
Figure 6 - A and C: Preoperative stage. B and D: Postoperative condition 6 months later.

Figure 7 - A and C: Preoperative planning for midabdominoplasty. B and D: Postoperative condition 6 months later.
RESULTS
The combination of liposuction and abdominoplasty1,9 with minimal central undermining, resection of the medial infraumbilical segment, and partial pubectomy resulted in improved cosmetic results as compared to the classical abdominoplasty technique. The rate of patient satisfaction was very high, around 98%. The number of complications also greatly reduced, especially for seroma, epitheliosis, and wound dehiscence. Further, the rate of reintervention (liposuction 6 months postoperatively), which was very high with the classical technique, decreased to around 4%.
The only complication was one case of hematoma, which required secondary lipoaspiration; however, the outcome was good. Two of the first 10 patients underwent massive supraumbilical liposuction and had some sagging skin in this area.
DISCUSSION
The appropriate framework for surgical correction of cosmetic deformities of the abdomen should include preoperative evaluation of candidates for abdominoplasty (Figure 1). The important parameters in this evaluation are skin type and texture, localized and generalized adiposity, muscle tone, patient age, lung capacity, and peripheral vascular system, in addition to factors related to plastic surgery in general.
In this paper, two alternatives to full abdominoplasty and miniabdominoplasty have been introduced: midabdominoplasty and partial pubectomy. The midabdominoplasty approach is suitable for patients requiring extensive skin resection, but it cannot be extended to the umbilical region, because the supraumbilical skin is insufficient to redo the whole abdomen, without a periumbilical incision, with or without undermining of the umbilicus (Figures 1C, 6, and 7). Partial pubectomy involves partial resection of the transverse part of the pubis, preventing elevation of scarring in this area, regardless of the stitch attachment, and allowing adequate delineation of the pubic size (Figure 5).
In all the procedures, maintenance of the vascular supply to the skin flap1 without extensive skin undermining ensures safety during liposuction, thus representing a historical advancement in the abdominoplasty technique. Further, surgical resection of the central part of the subdermal tissue without affecting its vasculature8 and limited supraumbilical undermining ensure direct visualization of the abdominal fascia and safe and proper plication, avoiding the risks of only connective tissue suturing, abdominal cavity penetration in an abdomen with large diastasis or significant muscle atrophy, and intestinal obstruction by inadvertently plicating an intestinal loop, a serious complication. Such resection also improves the cosmetic results (Figure 4).
In 2006, Graf et al.10 used Doppler imaging to demonstrate that abdominoplasty with undermining and preservation of perforating musculocutaneous vessels reduces the rate of complications such as necrosis and seroma. The modified technique also leads to greater patient satisfaction because of increased maneuverability with regard to liposuction not only in the abdominal flap but also in the back-flank-iliac regions, allowing better delineation and contouring of the waist and improving the global esthetic results.
The central resection of the skin and subcutaneous tissue does not harm the circulation of the abdominal flap, sourced from the lateral and musculocutaneous perforator vessels7 and through anastomotic arches between the inferior epigastric vessels (deep and superficial) and circumflex iliac vessels (deep and shallow), and prevents blood accumulation after plication of the lower abdomen. This procedure, coupled with partial pubectomy and minimal supraumbilical undermining, is therefore an important contribution to this area of medicine8. The main complication, which mostly led to a reintervention, was the need for secondary liposuction to correct the remaining irregularities8,11. The drastically reduced rate of complications may be attributable to two factors: (i) extensive liposuction of the abdominal flap and (ii) absence of seromas.
CONCLUSION
Resection of the medial infraumbilical segment during abdominoplasty with liposuction enables good visualization of the abdominal muscular fascia, well-preserved blood circulation, and safe plication of the rectus abdominis. Partial pubectomy guarantees well-consolidated scarring, ensuring a pleasant and satisfactory shape in relation to the height of the pubis. Therefore, liposuction and abdominoplasty with minimal undermining along with medial infraumbilical resection and partial pubectomy yield favorable esthetic results, due to better body contouring and reduced risk of complications, such as seromas, necrosis, and high incidence of secondary liposuction or lipoaspiration, commonly noted in the classical abdominoplasty technique.
REFERENCES
1. Avelar JM. Uma nova técnica de abdominoplastia: sistema vascular fechado de retalho subdérmico dobrado sobre si,combinado com lipoaspiração. Rev Bras Cir. 1999;6:3-20.
2. Sinder R. Cirurgia plástica do abdome. Rio de Janeiro: Ed. Ramil Sinder, 1979.
3. Pitanguy I. Abdominal lipectomy: an approach to it through an analysis of 300 consecutive cases. Plast Recosntr Surg. 1967;40(4):384-91.
4. Uebel CO. Cirurgia do abdome associada à lipoescultura. In: Tourniex AAB ed. Atualização em Cirurgia Plástica Estética. São Paulo:Robe Editorial; 1994. p.483-9.
5. Matarasso A. Liposuction as an adjunct to a full abdominoplasty revisited. Plast Reconstr Surg. 2000;106(5):1197-205.
6. Callia WEP. Contribuição para o estudo da correção cirúrgica do abdome pêndulo e globoso: técnica original [Tese de doutorado]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 1965.
7. Saldanha OR, Pinto EB, Matos WN Jr, Lucon RL, Magalhães F, Bello EM. Lipoabdominoplasty without undermining. Aesthet Surg J. 2001;21(6):518-26.
8. Erfon J. Abdominoplasty through a closed vascular system associated to liposuction: Avelar's technique. In: Avelar JM, ed. Abdominoplasty. São Paulo. Hipócrates,2002. p.299-307.
9. Illouz YG. Une nouvelle technique pour les lipodystrophies localiseés. Rev Chir Esthet Franc. 1980;6(9).
10. Graf R, Araujo LR, Rippel R, Neto LG, Pace DT, Cruz GA. Lipoabdominoplasty: liposuction with reduced undermining and traditional abdominal skin flap resection. Aesthetic Plast Surg., 2006;30(1):1-8.
11. Baroudi R, Ferreira CA. Seroma: how to avoid it and how to treat it. Aesthet Surg J. 1998;18(6):439-41.
Plastic Surgeon, Full Member of the Brazilian Plastic Surgery Society, Member of the Cearence Academy of Sciences (ACECI), Director of the ArtClinic, Fortaleza, CE, Brazil.
Corresponding author:
João Erfon Almeida Ramos
Av. Atilano de Moura, 530 - Edson Queiroz
Fortaleza, CE, Brazil - CEP 60810-180
E-mail: erfon@artclinic.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: January 6, 2011
Accepted: February 22, 2011
This work was performed at ArtClinic, Fortaleza, CE, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket