



Original Article - Year 2011 - Volume 26 -
Anatomy of lower lateral nasal cartilage in African descendants: a cadaveric study
Detalhes anatômicos das cartilagens laterais inferiores em afrodescendentes: estudo em cadáveres
ABSTRACT
Introduction: Aesthetic deformity of the nose and impaired nasal functioning may be related to structural variations in the lower lateral cartilage (LLC) and these variations can be either congenital or acquired. Few studies have investigated LLC morphology, and even fewer have investigated LLC morphology among African descendants. To meet this research gap, this study conducted an in-depth examination of LLC anatomy and its variation among a sample of African descendants. Methods: The noses of 16 fresh cadavers were dissected through exorhinoplasty to collect data regarding the shape, length, and width of the lateral and middle/medial crus, variations in these parameters in terms of the right and left sides and gender, and distance between the domus and the caudal septum for analysis using BioEstat 5.0 software. Results: Convex shape of the lateral crus was found to be predominant among the samples. Only 12.5% of the samples were found to have a unilateral concave shape and 6.25% to have a bilateral concave shape. The feet of the medial crus were found to be united in 81.25% of the samples and separated in 18.75%. The distance between the angle of the caudal septum and the domus was found to range from 4 to 10 mm (mean 6.86 ± 1.75 mm) among the samples. Conclusion: The parameters of LLC morphology among African descendants measured in this study were found to be similar to those previously described in the literature.
Keywords: Nasal cartilages. Anatomy. Cadaver. Nose. Rhinoplasty. African Continental Ancestry Group.
RESUMO
Introdução: São poucos os estudos na literatura que descrevem a morfologia das cartilagens laterais inferiores, sendo ainda mais raros em populações afrodescendentes. O objetivo desse estudo foi descrever a anatomia das cartilagens laterais inferiores e suas variações em afrodescendentes. Método: Foram estudados 16 cadáveres frescos. Os narizes foram dissecados através de exorinoplastia, com identificação e liberação das conexões das cartilagens laterais inferiores. As cruras laterais e cruras médias/mediais foram analisadas quanto a forma, comprimento e largura, sendo identificadas quanto ao lado e sexo. A distância entre o dômus e o septo caudal foi avaliada. Foi utilizada uma régua milimetrada para as mensurações. As medidas encontradas foram registradas e analisadas com auxílio do software BioEstat 5.0. Resultados: A forma convexa das cruras laterais foi predominante; enquanto a forma côncava ocorreu unilateralmente em dois casos e bilateralmente em um. Os "pés" da crura mediais estavam unidos em 81,25% da amostra e separados em 18,75% dos casos. A distância entre o ângulo do septo caudal e o dômus foi de 4 a 10 mm (média = 6,86 ± 1,75 mm). Conclusão: As cartilagens laterais inferiores dos afrodescendentes apresentaram dimensões semelhantes aos descritos na literatura.
Palavras-chave: Cartilagens nasais. Anatomia. Cadáver. Nariz. Rinoplastia. Grupo com Ancestrais do Continente Africano.
Being situated centrally and having a natural projection, the nose assumes a prominent position on the face1. The structure of the nose depends on both the bony and the cartilaginous framework2. The cartilaginous skeleton of the lower third of the nose is bilaterally formed by lower lateral cartilage (LLC), also known as alar cartilage, and by the caudal septum, which influences the shape and support of the nasal tip and columella and plays a role in the functioning of the external nasal valve2,3.
The LLC is formed by the lateral, middle, and medial crura3. The lateral crus may have a concave, convex, or mixed shape, while the medial crus may have joint or separate feet besides a concave or convex shape. These variations influence the nasal shape, projection, and the tip support4,5. LLC structural variations can be congenital, for example cleft nose and globe-like tips, or can be acquired, resulting after trauma or surgery. These changes may cause aesthetic deformities that are difficult to correct and impair nasal functioning6-11.
A properly designed nasal tip should include a span of 6 to 10 mm in the projection between the LLC domus and the septal angle. The soft tissue revealed during surgery and skin thickness directly affect the designing of the nasal tip projection end12. Knowledge of these variables and other aspects of LLC anatomy and its variations is important in planning and performing rhinoplasty, whether aesthetic or restorative. Despite this need, few studies have investigated LLC morphology, and even fewer have investigated LLC morphology among African descendants. To meet this research need, this study conducted an in-depth examination of the LLC anatomy and its variations among African descendants.
METHODS
A convenience sample of 16 fresh adult cadavers of African descent was obtained from the Forensic Institute Nina Rodriguez, Salvador, Bahia, in accordance with an agreement between that institution and the Universidade Federal da Bahia. From January to September 2010, the noses of 13 male and 3 female cadavers aged between approximately 20 and 70 years were dissected through exo-rhinoplasty, which exposed the LLC and released its connections with the septum and upper lateral cartilage. The parameters subsequently assessed were the anatomical form of the lateral and medial crura; maximum width and length of the lateral crus (Figure 1); positioning of the feet of the middle/medial crus (joint or separate); total length of the middle/medial crus, as measured from the lowest portion of the medial crus to the domus of the middle crus (Figure 2); and distance between the angle of the caudal septum (upper limit of the caudal septum) and the domus. Measurements were taken using a millimeter rule, and were recorded and analyzed using BioEstat 5.0 software.

Figure 1 - Length and width of the lateral crus.

Figure 2 - Length of the middle/medial crus.
RESULTS
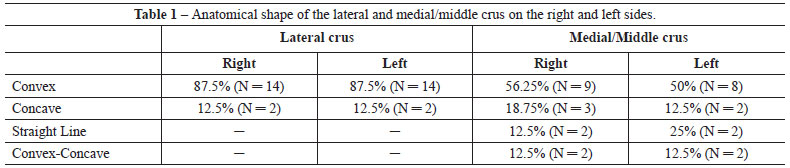
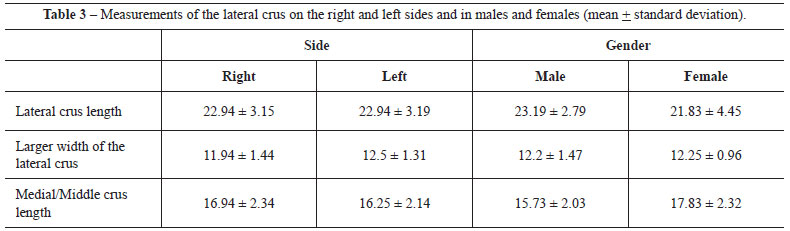
Convex shape of the lateral crus was predominant among the samples, whereas only 12.5% of the samples were found to have a unilateral concave shape and 6.25% to have a bilateral concave shape (Table 1). The distribution by gender is shown in Table 2. The measurements of the lateral and middle/medial crura on the right and left sides and in males and females are shown in Table 3. As can be observed, the feet of the medial crus were found to be joined in 81.25% of the samples and separated in 18.75% of the samples. The mean of the distance between the angle of the caudal septum and the domus was found to be 6.86 mm ± 1.75 mm (range 4-10 mm) for all the samples, 6.67 mm ± 2.08 mm in females, and 7.08 mm ± 1.78 mm in males.

DISCUSSION
Preservation or optimization of nasal functioning, a primary goal of aesthetic rhinoplasty, requires knowledge of cartilage morphology. Daniel subdivided the nasal tip, which corresponds to the lower third of the nose and is formed by the LLC, into the medial crus, the pillar upon which the tip rests and the primary component of the columella; the middle crus; and the lateral crus3. Among the various nasal structures, Doncatto et al.8 found that the nasal tip is the area of greatest dissatisfaction after rhinoplasty. The precision of nasal tip surgery depends on knowledge of the anatomical variations of the cartilage and the thoroughness of the assessment prior to amendment10. In a study of primary open rhinoplasty among Asians, Dhong et al.4 found the shape of the medial crus to be straight in 56% of the cases examined4. In contrast, this shape was found in only 23.08% of the samples in this study.
As the primary component of the nasal lobule, the lateral crus influences its shape, size, and position3. Regarding the mean width and length of the lateral crus, Zelnik and Gingrass reported the values to be 1.1 cm and 2.2 cm, respectively, among Caucasian populations6; Dhong et al. found them to be 1.0 cm and 1.9 cm, respectively, among Asian populations4; and Ofodile and James recorded values of 1.2 cm and 1.8 cm, respectively, among African populations5. We found the mean width and length of the lateral crus to be 1.2 cm and 2.3 cm, which are similar to the values reported in the literature. Regarding the shape of the lateral crus, we found it to be convex in 100% of the female samples and 84.62% of the male samples, findings that contrast with those of Dhong et al., who found the shape to be concave in 50% of their female samples and 40% of their male samples4. Regarding the distance between the angle of the caudal septum and the domus, referred to as the supratip break, we found the average value among all our samples to be 6.86 mm. Our value agrees with the default distance of 6 to 10 mm identified by Byrd et al., who proposed that this distance should vary according to skin thickness: specifically, from 6 to 8 mm in individuals with thin skin and from 9 to 10 mm in individuals with thick skin12. The wider variation found in our samples (4 to 10 mm) can likely be attributed to the miscegenation of the population from which they were obtained.
Highlighting the importance of the morphology of the feet of the medial crus in supporting and controlling the tip projection, Toriumi suggested that the relationship identified between the separate feet of the medial crus and middle/short medial crus favors the loss of projection in the postoperative period following rhinoplasty13. Obtaining detailed anatomical knowledge of the nasal framework and its variations, including those described here, is extremely important in the selection and proper planning of an effective approach to correct anatomic deformities, increase postoperative predictability, and prevent functional impairment.
CONCLUSION
The mean values that we obtained in our examination of the LLC morphology of African descendants are similar to those reported in the literature. Specifically, we found the lateral crus to be convex in 87.5% of the samples and observed greater morphological variation among the medial crus compared to the lateral and middle crura, mostly with regard to the joining or separation of the feet.
REFERENCES
1. Kawasaki MC, Tardelli HC, Costa CSS, Mélega JM. Rinoplastia transmucosa: técnica básica. In: Mélega JM, Baroudi R, eds. Cirurgia plástica fundamentos e arte, cirurgia estética. Rio de Janeiro:Medsi;2003. p.299-22.
2. Lessard ML, Daniel RK. Surgical anatomy of septorhinoplasty. Arch Otolaryngol. 1985;111(1):25-9.
3. Daniel RK. The nasal tip: anatomy and aesthetics. Plast Reconstr Surg. 1992;89(2):216-24.
4. Dhong ES, Han SK, Lee CH, Yoon ES, Kim WK. Anthropometric study of alar cartilage in Asians. Ann Plast Surg. 2002;48(4):389-91.
5. Ofodile FA, James EA. Anatomy of alar cartilages in blacks. Plast Reconstr Surg. 1997;100(3):699-703.
6. Zelnik J, Gingrass RP. Anatomy of the alar cartilage. Plast Reconstr Surg. 1979;64(5):650-3.
7. Bardach J, Cutting C. Anatomy of the unilateral and bilateral cleft lip and nose. In: Bardach J, Morris HL, eds. Multidisciplinary management of cleft lip and palate. Philadelphia:Saunders;1990.
8. Doncatto L, Giovanaz F, Decusati FL. Rinoplastia estético-funcional. Arq Cat Med. 2009;38(supl. 1):58-60.
9. Rohrich RJ, Adams WP Jr. The boxy nasal tip: classification and management based on alar cartilage suturing techniques. Plast Reconstr Surg. 2001;107(7):1849-63.
10. Tebbetts JB. Avaliação e modificação primárias da ponta. In: Tebbetts JB, ed. Rinoplastia primária: a nova abordagem lógica das técnicas. Rio de Janeiro:Di Livros;1998. p.103-35.
11. Rodney JR, Fritz EB, Larry H. Nasal reconstruction. In: Smith JW, Aston S, eds. Grabb and Smith's Plastic Surgery. 5th ed. Boston:Little Brown;1997. p.513-28.
12. Byrd HS, Andochick S, Copit S, Walton KG. Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg. 1997;100(4):999-1010.
13. Toriumi DM. New concepts in nasal tip contouring. Arch Facial Plast Surg. 2006;8(3):156-85.
1. Full Member of the Brazilian Society of Plastic Surgery (SBPC); Physician Assistant of the Discipline of Plastic Surgery at Universidade Federal da Bahia (UFBA), Salvador, BA, Brazil.
2. Full Professor; Associate Professor and Head of Cranio-Maxillo-Facial Surgery at Hospital das Clínicas of the School of Medicine of Universidade de São Paulo (HC-FMUSP), São Paulo, SP, Brazil.
3. Aspiring Member-in-training of SBCP; Resident Physician in Plastic Surgery at Hospital das Clínicas of UFBA, Salvador, BA, Brazil.
4. Medical Student at the UFBA School of Medicine, Salvador, Bahia, Brazil.
5. PhD; Associate Professor and Head of the Discipline of Plastic Surgery at FAMEB-UFBA; Supervisor of the Plastic Surgery League of Bahia, Salvador, BA, Brazil.
Corresponding author:
Victor Diniz de Pochat
Rua Conselheiro Correa de Menezes, 432, apto 201 - Horto Florestal
Salvador, BA, Brazil - CEP 40295-030
E-mail: victor.pochat@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: December 16, 2010
Accepted: February 21, 2011
Work performed at Hospital das Clínicas da Universidade Federal da Bahia (Clinical Hospital of Federal University of Bahia), Salvador, BA, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket