



Original Article - Year 2011 - Volume 26 -
Quality of life of patients in a burn treatment unit
Qualidade de vida do paciente internado em uma unidade de queimados
ABSTRACT
Objectives: The present study addressed the Quality of Life (QoL) of burn patients hospitalized in a burns unit. This study aimed to determine which domains of QoL of these patients were more impaired or preserved during hospitalization. Methods: The study was approved by the Ethics Committee of the Universidade Católica Dom Bosco, UCDB, in accordance with international and national laws. For the quantitative sample of 15 inpatients, we opted for descriptive and analytical statistics where the sampling represented 100% of the universe to be studied. The chosen survey instrument was the SF-36 (The Medical Outcomes Study Short-form Health Survey) because it is a generic questionnaire for health assessment and is easy to administer and understand. Results: The results showed that the domains of physical and emotional aspects, and pain were the most impaired during hospitalization. On the other hand, the domains that were more preserved were vitality, mental health, and general health status. Conclusion: The preponderant influence of individuals' perceptions of QoL in real conditions was ascertained. Even in physical conditions of great pain and limited movement, individuals tended to be optimistic, confident in their recovery, and demonstrated a good understanding of QoL patterns.
Keywords: Quality of life. Burns. Hospitalization. Burn Units.
RESUMO
Objetivos: O presente estudo abordou a Qualidade de Vida (QV) de pacientes queimados hospitalizados em uma Unidade de Queimados. O objetivo do estudo foi verificar quais domínios de QV desses pacientes estavam mais comprometidos ou preservados, durante a hospitalização. Método: A pesquisa foi aprovada pela Comissão de Ética da Universidade Católica Dom Bosco - UCDB, em consoante às legislações internacional e nacional. Pelo quantitativo da amostra de 15 pacientes internados, optou-se por uma estatística descritiva-analítica, onde a amostragem representava os 100% do universo a ser estudado. O instrumento de pesquisa escolhido foi o SF-36 - Medical Outcomes Short-form Health Survey, por ser um questionário de avaliação genérica de saúde, de fácil administração e compreensão. Resultados: Os resultados apresentados apontaram os domínios aspecto físico, aspecto emocional e dor como os mais comprometidos durante a hospitalização. Por outro lado, os domínios que se apresentaram como mais preservados foram: vitalidade, saúde mental e estado geral de saúde. Conclusão: Verificou-se a influência preponderante da percepção individual de QV sobre as condições da realidade. Mesmo estando em condições físicas de grande dor e limitação de movimentos, os indivíduos tenderam a se mostrar otimistas, confiantes na própria recuperação e demonstrando boa percepção de padrões de QV.
Palavras-chave: Qualidade de vida. Queimaduras. Hospitalização. Unidades de Queimados.
Over the past 10 years, working in hospital pedagogical care in a burn treatment unit, the author experienced working with burn patients, both children and adolescents, during hospitalization, and observed the difficultly patients had with the physical treatment combined with hospital realities.
It was noticed that adult patients desired to participate in complementary educational activities related to school curriculum (e.g., painting, drama, music, recreation, and reasoning games). Furthermore, it has been observed that people feel better when they can free themselves from their tensions through creative expression.
Professional intervention for adult patients was carried out using a pedagogic approach, particularly to listen, and understand and assist their development to improve their quality of life (QoL) during hospitalization. This intervention prompted the present QoL study.
QoL is currently considered one of the most interdisciplinary subjects, serving as a link between various specialized areas of knowledge such as sociology, medicine, nursing, psychology, economics, geography, social history, politics, religion, and philosophy1.
One of the most important publications on the subject is the book "Quality of Life and Pharmacoeconomics in Clinical Trials", (published in 1990), which included health professionals from various specialties and functions among its authors. Since then, medical professionals have linked patient health with QoL by means of various scientific publications. QoL started to be assessed either individually, in groups, and even in large populations2.
From this perspective, during the last decade, one of the greatest developments in the health field was the recognition of the importance of the patient's perception of their disease as well as the quality of employed therapeutic measures and treatment outcomes in his or her life3.
QoL assessment is now considered part of the patient's medical history and is being defended as a variable that is as important as survival or mortality rate; it is also becoming a topic of interest for research in the medical and psychosocial fields4.
This view is frequently expressed in the medical literature in that the best quality measure is not how often medical service can be offered to patients, but how close the treatment outcomes are relative to the essential objectives of prolonging life, relieving pain, restoring functions, and preventing disability5.
Various tools for measuring QoL can be used to evaluate the health and disease issues largely defined by the World Health Organization (WHO) and the techniques used for preventive and healing actions, and to instruct health area planners6.
The WHO has defined QoL as covering 5 dimensions: physical health, psychological health, level of independence, social relationships, and environment. Since the WHO defined health in terms of physical, psychological, and social conditions, some indexes along with traditional ones have been reviewed to consider situations or individuals as healthy6.
The literature on QoL, which is essentially medicalized and adopts a biostatistical and economic view of health, emphasizes that it is a mechanistic medicine that only aims to cure disease. Healthcare is primarily a human relationship in which the main objective is patient welfare7.
When incorporating researchers' perspectives within a multicultural and historical context, it is important is to consider that research on QoL in very different environments must account for diversity and not be limited to assumptions that are rooted in Western medicine8.
The QoL concept adopted by the WHO includes the observations necessary for research in a burns unit, including an individual's physical health, level of independence, social relationships, psychological state, personal beliefs, and relationships with key aspects of their environment9.
The burns unit where the present research took place has a multidisciplinary team that assists the entire midwest region of Brazil as well as some states in the north and neighboring countries, including Bolivia and Paraguay.
Therefore, hospitalization in such a burns unit may have different effects depending on the individual's age, burn intensity, involved professionals' efficiency, and the manner in which the family and patient deal with these factors.
Persistence in comorbidity situations (diseases accompanying the main pathology) often affects these patients' QoL10.
It is possible to observe the dynamics that are incorporated into health interventions, which consist of subjective elements related to the psyche, social life, and the cultural development of the sick individual, indicating the nature of the relationships established in the hospital context11.
Physical recovery depends on more than just proper sterilization or chemical treatment; it also seemingly increasingly depends on the correct approach regarding emotional impact12.
Treatment of acute trauma, deformity correction, appearance of sequelae, and rehabilitation are medical circumstances that require technical expertise and strong personal dedication. The multidisciplinary perspectives of general surgeons, plastic surgeons, dermatologists, clinicians, intensivists, pediatricians, anesthesiologists, hematologists, and other specialists provide a suitable approach considering that burn treatment success requires knowledge of various specialties13.
The importance of seeking the best QoL for patients is emphasized as a therapeutic precondition as indispensable as chemical treatment, nutritional supplementation, or physiotherapy.
The results achieved by the survey are included in the QoL assessment of inpatients in a burns unit and specifically identify which areas are most impaired and best preserved in the studied population.
METHODS
Fifteen inpatients at the burns unit were interviewed. The number of interviews represents all inpatients during the research period.
The established criteria for choosing study participants were the patient's ability to answer the questions and provide informed consent.
The instruments used to collect data were the sociodemographic characteristics survey and questionnaire SF-36 (The Medical Outcomes Study-36-item Short-Form Health Survey).
The sociodemographic characteristics survey is an instrument that collects information on biographical and identification data such as gender, age, education, and social information that may be associated with QoL such as marital status, occupation, income, number of children, religion, time of admission, type of burn, cause of the burn, and medical prognosis upon recovery.
Questionnaire SF-36 is a generic survey questionnaire to assess health that is easy to administer and understand. The questionnaire was chosen because it was available in Portuguese, was appropriate for the study goal, and had been validated in previous studies. Since it is a generic questionnaire, its concepts are not specific to one age, disease, or treatment group, enabling comparison with different diseases or different therapies14.
It is a multidimensional questionnaire consisting of 36 research items comprising 8 domains within 2 components as follows:
Physical component domain: functional capacity (FC), physical aspects (PA), pain (P), and general health status (GHS). Mental component domain: mental health (MH), emotional aspects (EA), social aspects (SA), and vitality (V).
To assess the responses, a score is given for each question that is later converted on a scale of 0 to 100, where 0 and 100 correspond to the worst and best health status, respectively. Each dimension was assessed separately.
The employed method qualitatively assessed the quantitative scores from the responses to each item. Therefore, this instrument is suitable for use when emotional responses submitted by each patient can be assessed individually.
The research procedure included the following steps:
1. An Authorization for Human Research was obtained from the Research Ethics Committee of Universidade Católica Dom Bosco (UCDB) as established by Resolution nº 196/1996 of the National Health Council (CNS) and in accordance with Article 30 of the Psychology Ethics Code, Resolution nº 016/2000 of the Federal Council of Psychology (CFP).
2. An Authorization for Research was then obtained from the hospital management according to the legislation in place.
3. All 15 inpatients were included in the expected interviews, taking into account the fact that this was the burn treatment center where it was possible to conduct the research.
4. Before each interview, the patient was informed of the research objectives and confidentiality; if they agreed, they signed an informed consent statement.
5. The patient was given the sociodemographic questionnaire and was required to fill it out thoroughly.
6. The procedure performed with the SF-36 questionnaire was conducted in a focused and independent way, with the researcher helping the patient whenever he or she requested.
Both questionnaires were applied in a single interview that lasted for about 30 minutes.
The SF-36 was administered by means of interviews and followed the express recommendation of this inventory's validation for cases in which the subject to be interviewed had a low socioeconomic or cultural level. In these cases, the use of an interview is the most viable way to obtain accurate results15.
Several variables were considered, including gender, age, income, burn degree, pain, and health status as well as variables related to FC, PA, V, SA, EA, and MH.
The results obtained from the SF-36 questionnaire were then converted into scores from 0 to 100 using the Likert scale14.
With the aim of organizing and describing the information from the research, tables and a graph were constructed.
Computed data were analyzed from descriptive and analytical statistics perspectives. For statistical studies, the bootstrap test was used (permutation test) with average test statistics. This test worked with scores obtained from each patient for each domain regarding the various aspects of QoL from the SF-36 instrument and sociodemographic questionnaire items list with some of these domains, mainly those most affected. The test revealed statistically significant differences among all known average values, giving p values of <0.05.
RESULTS
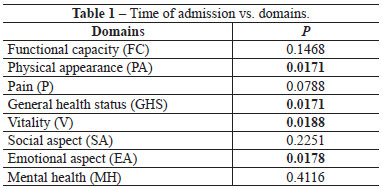
The studied patients were divided into 2 groups: one with patients hospitalized for more than 14 days and the other with patients hospitalized for 14 days or less.
When comparing the domains of each of the groups using the permutation test, there were significant differences in the domains of PA (p=0.0171), GHS (p=0.0171), V (p=0.0188), and EA (p= 0.0178) (Table 1).
In the permutation test performed between the 2 groups, there were significant differences with respect to PA, GHS, and EA between groups (Table 2). It was observed that shorter hospital admission times resulted in better QoL indicators.
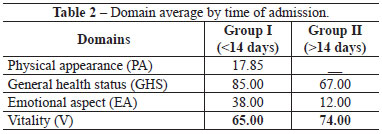
Longer admission times resulted in significantly better QoL with respect to the V domain. However, the indicators of the 2 groups were opposite with respect to other domains.
The comparison between the averages in Table 2 reinforces the idea that despite acquiring a better perception of their vitality with increasing admission time and the efforts of the multidisciplinary team, the hospital environment contributes to the deterioration of the individuals' perceptions of their QoL in the domains of PA, EA, and GHS.
Figure 1 shows the average values of all domains indicating those that are the most impaired and best preserved in the surveyed patients during hospitalization.

Figure 1 - Average values for each domain.
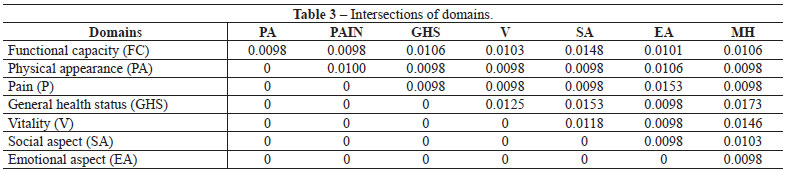
To determine which average values in Figure 1 are significantly different, a permutation test was performed to compare domains (Table 3). Note that all demonstrated p values are less than 0.05. Therefore, at the significance level of 5%, we observed statistically significant differences among all average values presented in Figure 1.
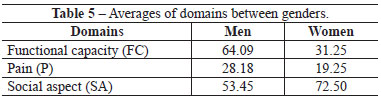
There were significant differences (p < 0.05) in all domains with respect to gender (Table 4). There were significant differences in FC, P, and SA.

As shown in Table 5, the FC, P, and SA domains were significantly different with respect to gender; men had higher averages in the FC and P domains, while women had a higher average in the SA domain.
DISCUSSION
Using the SF-36 instrument, the most impaired and most preserved QoL domains during hospitalization as well as the relationships between the domains and individual characteristics were studied in a group of 15 burn patients.
One of the biggest recent developments in the health field is the professionals' acknowledgment of the importance of the patients' perspective regarding their own disease3.
A good medical prognosis seems to influence the respondents' QoL. Studies on the psychological implications of prognoses on inpatients suggest that self-perception of welfare and uneasiness seems to contribute to the biological evolution of the disease, which might become a therapy cofactor; it is concluded that psychology contributes toward a better QoL in inpatients16.
The original sample showed significant results regarding the SF-36 instrument QoL domains. Domains that had lower averages were PA, EA, and P, implying that these domains were the most impaired during hospitalization.
These results are consistent with those of a study on patients with Stevens-Johnson Syndrome; because the subjects in that study had impaired visual acuity, they showed impairments in PA, EA, and P17.
Research on patients with sickle cell disease also corroborates the results of the present study, showing the PA, EA, and P domains as the most impaired18.
The FC and SA domains had averages that were quite similar: they were higher than those among the most impaired but below those of the most preserved domains. The large losses in the PA, EA, and P domains probably affected the results of the FA and SA domains.
These results are consistent with evidence that physical improvement increases functional activity independence, reducing negative psychological reactions and intensifying social contacts19.
A study that assessed patients with rheumatoid arthritis further corroborates the findings of this study that changes in physical aspects directly interfered with daily living and social activities and involved significant emotional aspects that somehow affect these patients' QoL14.
In this study, the domains with the highest averages, which were considered the most preserved, were V, MH, and GHS.
However, research on sickle cell disease patients revealed lower scores for mental components (i.e., V and MH) and a lower average score for GHS, in contradiction with the present results18.
Regarding the gender correlation of each domain, males had greater impairment in the domains of FC and P, while women had greater impairment in SA. The results of a study of elderly patients show greater impairment in men with respect to SA.
In QoL studies with patients with hyperhidrosis (excessive sweating), SA was identified as the most impaired domain among male patients, which also contradicts the results of the present study20.
Studies on QoL in women with fibromyalgia also contradict the present results in that the most impaired domains were related to physical components (i.e., FC and P)21.
Comparing the domains between two groups of inpatients according to hospitalization time, we observed that shorter hospitalization times resulted in better QoL indicators. Conversely, longer hospitalization times resulted in better averages for the V domain.
These data are consistent with the cited studies indicating that over time, patients gain control and confidence regarding their hospitalization. A patient who feels that he/she is a hospitalized citizen (i.e., an owner of rights) generally has a good QoL. Prolonged hospitalization makes the patient feel more prepared by increasing vitality12.
Prolonged hospitalization gives the patient more time to reflect on his/her own existence, helping the patient to plan and maintain confidence in recovery18.
Although the study sample comprised a small number of patients, the results contribute toward a better understanding of the psychosocial aspects of burn patients.
CONCLUSION
The sociodemographic survey and the SF-36 questionnaire were used to assess QoL of inpatients at a burn treatment center and revealed that the PA, EA, and P domains were the most impaired. On the other hand, the V, MH, and GHS domains were the most preserved. Thus, despite the small sample size used, the research objectives were achieved.
Further, apart from technical expertise, it is believed that human affection shown by professionals in a burn treatment center somehow minimizes the patients' suffering, increases their perception of good QoL, and substantially improves recovery speed and efficiency.
Further studies are necessary to better understand the recovery mechanisms influenced by the patient's perception of good QoL and using them in favor of the patient.
REFERENCES
1. Farquhar M. Elderly people's definitions of quality of life. Soc Sci Med. 1995;41(10):1439-46.
2. Souza JC, Guimarães LAM. Insônia e qualidade de vida. Campo Grande-MS: UCDB;1999.
3. Ruta DA, Garrat AM, Leng M, Russel IT, MacDonald LM. A new approach to the measurement of quality of life. The Patient-Generated Index. Medical Care. 1994;32(11):1109-26.
4. Silval G, Naspitz CK, Solè D. História clínica do paciente e avaliação de qualidade de vida. Rev Bras Alergia Imunopatol. 2000;23(6):260-9.
5. Bowling A, Brasier J. Quality of life in social science and medicine. Soc Sci Med. 1995;41:1337-8.
6. Fleck MPA. Avaliação de qualidade de vida. In: Fráguas Junior R, Figueiró JAB, orgs. Depressão em medicina interna e em outras condições médicas: depressões secundárias. São Paulo: Atheneu;2000. p.120-53.
7. Hubert A. De la difficulté de définir une definicion. Revue Prevenir, Paris, 1997;15-8.
8. Pope-Davis DB, Liu WM, Toporek RL, Brittan-Powell CS. What's missing from multicultural competency research: review, introspection and recommendations. Cultur Divers Ethnic Minor Psichol. 2001; 7(2):121-38.
9. Herdman M, Fox-Rushby J, Badia X. 'Equivalence' and the translation and adaptation of health-related quality of life questionaries. Qual Life Res. 1997;6(3):237-47.
10. Castro M, Caiuby AVS, Draibe SA, Canziani MEF. Qualidade de vida de pacientes com insuficiência renal crônica em hemodiálise, avaliada através do instrumento genérico SF-36. Rev Assoc Med Bras. 2003;49(3):32-9.
11. Vasconcellos EA. Enfrentando a doença no hospital: uma abordagem de pacientes com doenças crônicas [Dissertação de Mestrado]. Campinas:Faculdade de Ciências Médicas, Universidade de Campinas; 2000. 138p.
12. Medina A. Distúrbios de consciência. Rio de Janeiro: Cultura Médica; 1984.
13. Maciel E, Serra MC. Tratado de queimaduras. Belo Horizonte: Atheneu;2004.
14. Ciconelli RM. Avaliação da qualidade de vida em doenças reumáticas. Rev Sinopse Reumatol. 1999;2:1-4. Disponível em: br/pscologia/geral/pdf/qualidade.pdf>. Acesso em: 20/dez/2003
15. Ciconelli RM. Tradução para o português e validação do questionáriogenérico de avaliação de qualidade de vida [Tese de Doutorado]. São Paulo: Universidade Federal de São Paulo (EPM); 1997. 120p.
16. Nucci NAG. Qualidade de vida e câncer: um estado compreensivo [Tese de Doutorado]. Ribeirão Preto:Faculdade de Filosofia Ciências e Letras de Ribeirão Preto, Departamento de Psicologia, Universidade de São Paulo;2003. 225p.
17. Schwartz GS, Gomes JAP, Holland ES. Preoperative staging of disease severity. In: Holland ES, Mannis MJ, eds. Ocular surface disease: medical and a surgical management. New York: Spring-Verlay;2001. p.158-67.
18. Assis R. Qualidade de vida do doente falcêmico [Dissertação de Mestrado]. Campinas: Faculdade de Ciências Médicas, Universidade de Campinas;2004. 98p.
19. Barbosa CRM. Saúde, qualidade de vida e envelhecimento: a inclusão do homem idoso em programas para a terceira idade [Dissertação de Mestrado]. Rio de Janeiro:Universidade Federal do Rio de Janeiro; 2003. 134p.
20. Amir M, Arish A, Weinstein Y, Pfeffer M, Levy Y. Impairment in quality of life among patients seeking surgery for hyperhidrosis (excessive sweating): preliminary results. Isr J Psychiatry Relat Sci. 2000;37(1):25-31.
21. Martinez JE, Barauna Filho IS, Kubokawa K, Pedreira IS, Machado LA, Cevasco G. Evaluation of the quality of life in Brazilian women with fibromyalgia, through the medical outcome survey 36 item short-form study. Disabil Rehabil. 2001;23(2):64-8.
Masters in Psychology; Professor at the Pediatrics and Burn Unit of the Benevolent Association Santa Casa de Campo Grande, Campo Grande, MS, Brazil.
Corresponding author:
Teresinha de Jesus Abreu de Souza
Rua da Coroa, 29 - Vila Carlota
Campo Grande, MS, Brazil - CEP 79081-580
E-mail: tekajesus@yahoo.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: January 20, 2010
Accepted: January 22, 2011
Work performed at the Unidade de Queimados da Associação Beneficente Santa Casa de Campo Grande (Burns Unit of the Benevolent Association Santa Casa de Campo Grande), Campo Grande, MS, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket