



Ideas and Innovation - Year 2026 - Volume 41Issue 1
Neuroguided Surgery: A Safe Technique to Prevent Nerve Injuries in Rhytidoplasty
Cirurgia neuroguiada: uma técnica segura para prevenir lesões nervosas em ritidoplastia
Marcelo de Oliveira e Silva1 ; Paulo Liborio1,; Rosa Maria Marquezine Cara1
; Paulo Liborio1,; Rosa Maria Marquezine Cara1
ABSTRACT
Rhytidoplasty (facelift surgery) ranks among the most frequently performed esthetic procedures worldwide. However, the growing volume of surgeries has increased the incidence of complications, particularly nerve injuries. Among these complications, facial nerve damage remains one of the most feared, due to its potential to cause facial paralysis, resulting in both esthetic and functional issues. In response to this challenge, neuronavigation has emerged as a viable, effective tool. By providing real-time,millimetric location of facial nerve branches, neuronavigation enables safer surgical dissection, even in cases with altered or challenging anatomical landscapes. The present article introduces the concept of neuroguided facial surgery, a technique that can be integrated into facelift procedures to minimize the risk of iatrogenic facial nerve injury. The current study has the4 goal of describing the neuroguided approach in facelift surgery, highlighting its efficacy in reducing the incidence of nerve-related complications.
Keywords: neuroguided surgery; facial nerve injury; rhytidoplasty
RESUMO
A ritidoplastia (cirurgia de lifting facial) está entre os procedimentos estéticos mais frequentemente realizados em todo o mundo. O aumento do volume de cirurgias tem sido acompanhado por uma maior incidência de complicações, especialmente lesões nervosas. Entre essas, a lesão do nervo facial continua sendo uma das mais temidas, devido ao seu potencial de causar paralisia facial, com consequências tanto estéticas quanto funcionais. Em resposta a esse desafio, a neuronavegação surgiu como uma ferramenta viável e eficaz. Ao fornecer a localização milimétrica e em tempo real dos ramos do nervo facial, a neuronavegação permite uma dissecção cirúrgicamais segura, até mesmo em casos com anatomia alterada ou de difícil identificação. Este artigo apresenta o conceito da cirurgia facial neuroguiada, uma técnica que pode ser incorporada aos procedimentos de ritidoplastia para minimizar o risco de lesões iatrogênicas do nervo facial. Este estudo tem como objetivo descrever a abordagem neuroguiada na cirurgia de lifting facial, com destaque para sua eficácia na redução da incidência de complicações relacionadas a lesões nervosas.
Palavras-chave: cirurgia neuroguiada; lesão de nervo facial; ritidoplastia
Introduction
Facelift surgery (rhytidoplasty) is one of the most popular cosmetic procedures, with several techniques for facial reju-venation. As this surgery has evolved, so have its complica-tions. Among these complications, facial nerve injuries are a critical concern. Damage to a facial nerve branch can result in facial muscle paralysis, leading to facial asymmetry, func-tional impairments, and psychosocial issues.1
Nerve injuries occur in up to 4% of the cases,2 and permanent damage leads to facial-muscle atrophy, oral asymmetry, nasal collapse, lower-lip deformities, ectropion, lagophthalmos, and keratitis. These complications vary depending on the etiology, the level of injury, the duration of the paralysis, and individual biological characteristics.3,4 They are often irreversible and can have profound esthetic and functional repercussions. The treatment of facial paral-ysis remains a challenge for plastic surgeons and has limited results. Restoring a symmetrical facial expression to its fullness is virtually impossible.5-7
As surgical techniques become more complex, the risk of nerve damage increases. The deep-plane facelift technique, for instance, involves deeper dissection planes and releases facial ligaments close to facial nerves. Moreover, the increas-ing use of collagen biostimulators, thread lifts, and fillers in previous facial treatments can alter healthy anatomical structures, presenting an additional challenge for surgeons. In this context, the need for more precise and reliable methods to prevent nerve injury is evident.
In neurosurgery and craniofacial surgery, nerve injury is also a concern, and neuronavigation has proven invaluable. This technology enables the precise identification of key anatomical structures, including cranial nerves. As such, it enhances the surgeon’s ability to perform procedures with millimetric precision and minimizes the risk of injury.2,8
Inspired by this approach, the current article presents the neuroguided facial surgery technique. This technique can be widely combined with facelift procedures, employing intra-operative navigation and monitoring to protect the facial nerve and its branches, preventing iatrogenic injuries during facelifting.
Objective
The present article describes the technique of nerve moni-toring during facelift surgery. The study focused on the safe identification of facial nerve branches and emphasized its benefits in the prevention of nerve injuries.
Materials and Methods
The current study involved 10 patients (7 women and 3 men) eligible for deep-plane facelift surgery, aged between 45 and 67 years, who were selected sequentially. None of the patients had undergone previous facial surgeries. Two patients had never undergone previous esthetic procedures.
The remaining eight subjects had already undergone treat-ments with injectable collagen biostimulators (polylactic acid and calcium hydroxyapatite) and non-permanent fillers (hyaluronic acid).
All selected patients underwent electroneuromyography (ENMG) no later than 30 days before surgery to rule out preexisting nerve lesions. No abnormal findings were iden-tified on the ENMG.
Surgical procedure
The patients were in the supine position under general anesthesia with no muscle relaxants to avoid interfering with nerve stimulation. A sterile preparation using 2% chlor-hexidine degerming solution and 0.2% chlorhexidine alcohol solution was performed on the face, followed by the applica-tion of sterile drapes. Neuronavigation was then installed bilaterally on the face to monitor areas at risk of nerve injury during dissection.9
Before starting the surgery, the patients received a sub-dermal infiltration (25 mL per hemiface) of a 0.5% saline solution with adrenaline (1:200,000), without local anes-thetics, covering an area in the shape of a 4-cm radius semicircle, centered on the anterior border of the tragal tubercle, to minimize bleeding during subcutaneous dissec-tion before proceeding to the sub-submuscular aponeurotic system (sub-SMAS) layer.
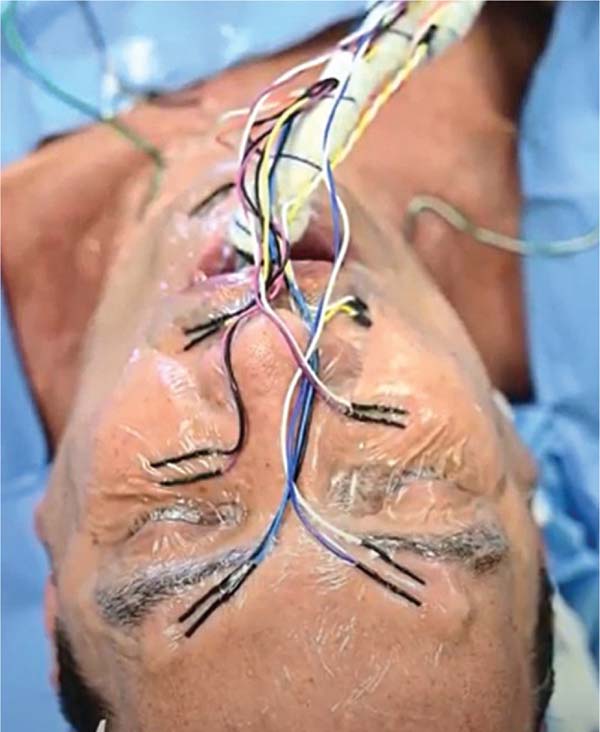
Lead placement
Five pairs of leads were placed bilaterally along the main branches of the facial nerve:
Temporal branches: 1 cm above the orbital rim, on the midpupillary line;
Zygomatic branches: 2 cm below the orbital rim, on the midpupillary line;
Buccal branches: Midway between the labial commis-sure and the nasal ala;
Mandibular branches: 2 cm laterally to the midline of the chin; and
Cervical branches: 1.5 cm below the mandible, on the anterior border of the sternocleidomastoid muscle.
The leads were inserted obliquely (30-45°) into the subdermal plane and protected with sterile, transparent dressings (►Fig. 1). Placement and preparing of all leads, as well as setting up the device, took 15 to 20 minutes.

Intraoperative neuromonitoring
During the surgeries, the NIM Response 3.0 system (Med-tronic plc) monitored facial nerve activity. The surgeon used an electrical stimulation probe connected to the system. The distal portions of the leads and the probe were also attached to the same interface. The parameters included a variable intensity between 0.5 mA and 1.0 mA, which ensured a depth and approximation margin of 0.3 to 0.5 mm between the stimulation point and the nerve.
The risk of injury to any branch of the facial nerve, either from direct contact or excessive traction, triggered an audible alarm and recorded a change in the ENMG waveform, reflecting the intensity of the stimulus (►Videos 1-2).
Video 1
Using an electrical stimulation probe, the surgeon identifies the buccal branch of the facial nerve. Online content including video sequences viewable at: https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0046-1816068.
Video 2
Monitor view of intraoperative electroneuromyography showing the facial nerve and its branches. Online content including video sequences viewable at: https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0046-1816068.
Dissection was performed with a high-frequency electro-surgical unit, set to coagulation mode at 10 MHz, which provided precise tissue separation while preserving nerve integrity. The surgeon monitored the neuronavigation screen and ENMG feedback to ensure safe dissection, making real-time adjustments as needed.
At the end of the procedures, the surgeon checked the integrity of each facial nerve branch using an electrical probe. Next, the leads were removed, and the surgery was complet-ed with sutures and dressings.
Each patient underwent an ENMG of the face 30 days after surgery to confirm full functionality of the facial nerve and its branches.
Results
A comparative analysis of the pre-, intra-, and postoperative ENMG scans revealed that no patient presented with facial nerve injury. All branches of the facial nerve remained intact, with no record of damage during surgery or in the 30-day follow-up.
Discussion
The increasing complexity of facial rejuvenation surgeries, especially those involving deeper anatomical planes, has heightened concerns about nerve injury. The proximity of facial nerve branches to key surgical areas, combined with alterations in facial anatomy resulting from previous esthetic treatments, highlights the need for more precise surgical techniques to minimize the risk of injury. Neuroguided facial surgery involving neuronavigation and ENMG monitoring offers a highly-effective solution. Real-time identification of nerve branches and the ability to monitor proximity during surgery significantly reduce the risk of injury. Fur-thermore, this approach enables surgeons to perform precise dissections with greater safety, even under altered anatomi-cal conditions. The current study demonstrates that neuro-guided facial surgery is an effective method to prevent nerve injury, offering valuable surgical safety and peace of mind to the surgeon. The integration of intraoperative monitoring has the potential to become standard practice in esthetic surgery, minimizing risks. It is strongly recommended that surgeons perform intraoperative monitoring of facial-nerve branches whenever possible. Moreover, the neuroguided facial surgery technique provides a crucial additional safety measure, which can pave the way for the development of new surgeries for facial rejuvenation.
Conclusion
In neuroguided facial surgery, the use of neuronavigation and ENMG results in a safe, effective, and precise technique to protect the branches of the facial nerve during facelifting. This method significantly reduces the risk of iatrogenic injuries, ensures safer dissection in the vicinity of facial ligaments, and enables a more effective release of the SMAS layer. The present article underscores the need for contin-uous innovation in cosmetic surgery, particularly in the integration of technologies to increase safety. The use of neuroguided surgery in facelifting paves the way for safer and more predictable results in the field of facial rejuvenation.
REFERENCES
1. Baker TJ, Gordon HL. Complications of rhytidectomy. Plast Reconstr Surg 1967;40(01):31-39. Doi: 10.1097/00006534-196707000-00004
2. Eisele DW, Wang SJ, Orloff LA. Electrophysiologic facial nerve monitoring during parotidectomy. Head Neck 2010;32(03): 399-405. Doi: 10.1002/hed.21190
3. Stuart RM, Byrne PJ. The importance of facial expression and the management of facial nerve injury. Neurosurg Q 2004;14(04):239-248. Doi: 10.1097/00013414-200412000-00009
4. Ferreira MC. Aesthetic considerations in facial reanimation. Clin Plast Surg 2002;29(04):523-532. Doi: 10.1016/s0094-1298(02) 00017-2
5. Labbé D, Hamel M, Bénateau H. [Lengthening temporalis myo-plasty and transfacial nerve graft (VII-V). Technical note]. Ann Chir Plast Esthet 2003;48(01):31-35. Doi: 10.1016/S0294-1260 (02)00180-2
6. Lazarini PR, Fouquet ML. Paralisia facial: avaliação, tratamento e reabilitação. 1ª ed. São Paulo: Lovise; 2006
7. Vlastou C. Facial paralysis. Microsurgery 2006;26(04):278-287. Doi: 10.1002/micr.20240
8. Lydiatt DD. Medical malpractice and facial nerve paralysis. Arch Otolaryngol Head Neck Surg 2003;129(01):50-53. Doi: 10.1001/archotol.129.1.50
9. Seckel BR. Facial Danger Zones: Avoiding Nerve Injury in facial plastic surgery. Can J Plast Surg 1994;2(02):59-66. Doi: 10.1177/229255039400200207
1. Plastic Surgery Service, Hospital Quinta D’Or, Rio de Janeiro, RJ, Brazil
Address for correspondence Paulo Liborio, M.D., Serviço de Cirurgia Plástica, Hospital Quinta D’Or, Rua Almirante Baltazar, 435, Rio de Janeiro, RJ, CEP: 22471-211, Brazil (e-mail: prliborio@gmail.com).
Article received: September 18, 2024.
Article accepted: August 26, 2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket