



Original Article - Year 2026 - Volume 41Issue 1
Epidemiological Profile of Patients Submitted to Intralesional Triamcinolone for the Treatment of Keloids
Epidemiological Profile of Patients Submitted to Intralesional Triamcinolone for the Treatment of Keloids
Gabriella Ueharo Pereira1, ; Luiz Eduardo Felipe Abla1; Sidney Mamoru Keira1; José Octavio Gonçalves de Freitas1
; Luiz Eduardo Felipe Abla1; Sidney Mamoru Keira1; José Octavio Gonçalves de Freitas1
ABSTRACT
Introduction Materials and
Methods The present retrospective study analyzed data from the electronic medical records of 17 patients undergoing TCN treatment from January 2022 to July 2023.
Results The demographic profile indicated that 88.2% of patients were female, 35.3% were Black, and 41.2% identified as Brown. Less than half (41.3%) of the patients completed treatment. Following the first TCN application, 53% of patients reported improvement in the appearance of the keloid, characterizing the outcome as good or excellent.
Conclusion The epidemiological profile of the treated patients aligns with literature data - in which more than 80% of subjects were Black or Brown and more than 80% were women. Approximately 40% of the sample presented keloids in the thoracic region (anterior chest and inframammary fold).
Keywords: cicatrix; epidemiology; hypertrophic cicatrix; keloid; triamcinolone
RESUMO
Introdução Queloides correspondem a alterações fibroproliferativas decorrentes de lesões cutâneas profundas causadas por traumas locais. A triancinolona (TCN) intralesional é uma das formas usadas no tratamento. O objetivo deste estudo foi avaliar o perfil epidemiológico dos pacientes com queloides, tratados com TCN no Serviço de Cirurgia Plástica do Hospital Ipiranga.
Materiais e Métodos Estudo retrospectivo, comdados de prontuários eletrônicos de 17 pacientes submetidos a injeção de TCN, de janeiro de 2022 até julho de 2023.
Resultados O perfil demográfico indicou que 88.2% dos pacientes eram do sexo feminino, 35.3% eram negros e 41.2% pardos. Menos da metade (41.3%) dos pacientes completou o tratamento. Com a primeira aplicação, 53% dos pacientes relataram melhora do aspecto do queloide, caracterizando o resultado como bom ou ótimo.
Conclusão O perfil epidemiológico dos pacientes tratados condiz com os dados encontrados na literatura - mais de 80% eram negros ou pardos e mais de 80% eram mulheres. Aproximadamente 40% da amostra apresenta o achado na região torácica (tórax anterior e sulco inframamário).
Palavras-chave: cicatrizes; cicatriz hipertrófica; epidemiologia; queloide; triancinolona
Introduction
Keloids are fibroproliferative abnormalities resulting from deep skin lesions caused by several types of local trauma (previous surgeries, burn injuries, and even piercings or tattoos).
They extend beyond the edges of the original wound, invading adjacent healthy skin, with no spontaneous regression.1
Keloids can appear years after the triggering factor, as firm nodules, often itchy and painful. Their spontaneous resolution is rare. Keloid growth can continue, unlike hypertrophic scars, which typically stabilize or regress after reaching a certain size.2
Keloids represent a multifaceted clinical and scientific challenge, and their understanding transcends the simple scar response to trauma. Their pathophysiology, marked by a complex dysregulation of collagen synthesis and pro-fibrotic cytokine signaling, reflects an intricate interplay between genetic predisposition, epigenetic factors, and environmental stimuli. Studies indicate that polymorphisms in genes such as those encoding the transforming growth factor-beta (TGF-β) or SMAD may contribute to fibroblast hyperproliferation, suggesting that the etiology of keloids is not restricted to local mechanisms but involves systemic molecular networks that have not yet been fully elucidated.3,4
Beyond their biological implications, keloids carry a significant psychosocial burden. Their location in exposed areas, such as the chest, face, and ears, supports hypotheses that they occur primarily in areas of high skin tension.5 They are often associated with chronic itching and pain, compromising self-image and quality of life, especially in young populations and in more susceptible ethnic groups, such as Black, Hispanic, and Asian populations.6,7 This ethnic disparity, with an incidence up to 15 times higher in people of African descent, not only reinforces genetic influence but also highlights gaps in access to effective treatments in vulnerable socioeconomic contexts, in which practices such as piercings or untreated trauma may be more prevalent.
A key treatment for keloids is intralesional corticosteroid injection, most commonly using triamcinolone (TCN), whose administration is the first-line treatment for this condition4 and can occur in an outpatient setting, facilitating outcome monitoring. This medication can reduce scar vascularization, pigmentation, and size.3 Triamcinolone treatment leads to resolution rates ranging from 50 to 100%.8
This variation in therapeutic success highlights the urgency for multimodal approaches, integrating cryotherapy, laser therapy, pressure therapy, and emerging biological therapies, such as TGF-β inhibitors. Personalized treatment, considering not only clinical characteristics but also the patient’s epidemiological profile, including gender, ethnicity, and history of relapses, is a fundamental axis for optimizing outcomes. In this context, local epidemiological studies, such as ours, are crucial in guiding initial protocols with adaptations to the particularities of the population, including social classes, since TCN is a treatment modality accessible to patients covered by the Brazilian Unified Health System (Sistema Único de Saúde, SUS, in Portuguese), reducing disparities and strengthening evidence-based medicine.
Keloid treatment is broad and requires an interdisciplinary approach, combining basic, clinical, and public health research to unravel its enigmas and transform therapeutic challenges into opportunities for innovation.
Objective
To evaluate the epidemiological profile of patients with keloids undergoing treatment with intralesional TCN in the Plastic Surgery Service of Hospital Ipiranga (SICPHI), São Paulo, SP, Brazil, from January 2022 to July 2023.
Materials and Methods
The current retrospective study analyzed data from the electronic medical records of patients who underwent intralesional TCN injection on an outpatient basis from January 2022 to July 2023 at Hospital Ipiranga. The study included patients over 16 years old with keloids and symptoms such as pain and pruritus who desired local treatment. We excluded patients who did not accept the proposed treatment methodology. The Ethics Committee approved the study (CAAE 89273925.1.00005488).
Treatment consisted of TCN hexacetonide (20 mg/mL) combined with lidocaine without vasoconstrictor (1:200,000) in the same proportion, in doses divided according to the keloid size in each patient. Treatment administration occurred at 21-day intervals, with a total of up to 8 treatments and an average of 3 applications. No patient in the present study required surgery after treatment.
Patients’ personal data was kept confidential, with no identification or exposure, in compliance with the principles of the Declaration of Helsinki.
Results
Seventeen patients underwent TCN applications on an outpatient basis from January 2022 to July 2023. The treatment was deemed complete after the end of the proposed applications for each patient (according to their lesion) and the report of their satisfaction level with the outcome (reduction of symptoms, such as itching and pain, regression of the lesion’s dimensions, and improvement of the aesthetic appearance of the local skin).
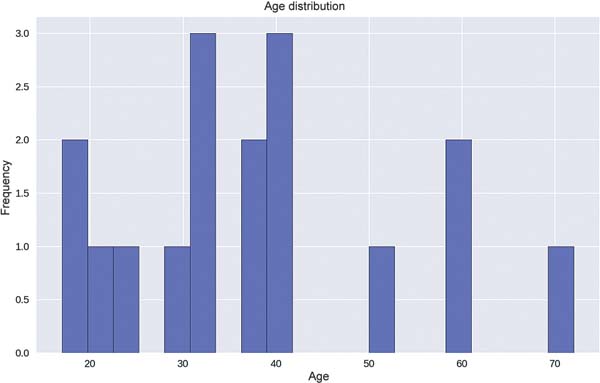
Regarding age, 11.8% of the patients were under 20 years old, 17.7% were between 20 and 30 years old, 4.2% were between 30 and 40 years old, 17.7% were between 50 and 60 years old, and 5.9% were between 70 and 80 years old. The mean age of the sample was 37.8 years (►Fig.1).

Most patients (88.2%) were female, with only 11.8% being male. Of the patients, 35.3% were Black, 41.2% were Brown, and 23.5% were Caucasian (►Table 1).
| Number of patients | Percentage | |
|---|---|---|
| Brown | 7 | 41.2% |
| Black | 6 | 35.3% |
| Caucasian | 4 | 23.5% |

As for the factor triggering the keloid, 5.9% of patients had the initial trauma 34 years ago (1989), 5.9% 14 years ago (2009), and 88.2% in the last 5 years (17.6% in 2018, 5.9% in 2019, 5.9% in 2020, 41.2% in 2021, and 17.6% in 2022).
In the study patients, the treated lesions were in several locations: 29.4% in the inframammary fold, 17.6% in the abdominal region (lower quadrants and umbilical region), 11.8% in the anterior chest, 11.8% in the face, 11.8% in the limbs, 11.8% in the auricular region, and 5.9% in the anterior cervical region.
In our sample, none of the patients was an active smoker. Most participants (82.4%) said they never smoked, while 17.6% were former smokers, having quit before starting their respective treatments.
Of the 17 patients, 41.3% completed the treatment. Among the remaining subjects, 11.8% of participants underwent a single TCN application, 11.8% had 4 to 5, 5.9% had 2, and 5.9% underwent 8 applications. Most participants (52.9%) underwent 3 applications.
After the 1st treatment, 47.1% of patients reported no change in the scar. Another 41.2% reported an improvement in the appearance of the keloid, characterizing the outcome as good, and 11.8% said it was excellent. Of the patients who completed the full treatment (41.3% of the sample), 1 subject noticed no difference in the outcome. Two patients categorized the outcome as good and four as excellent.
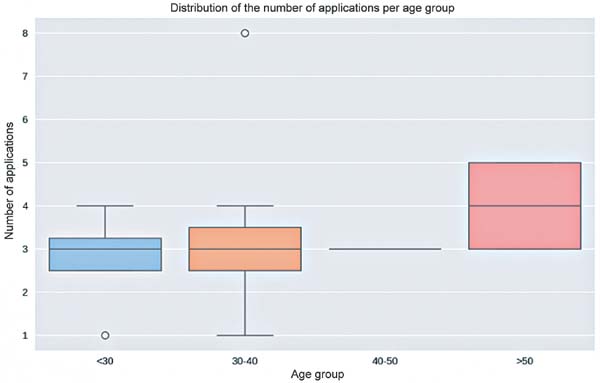
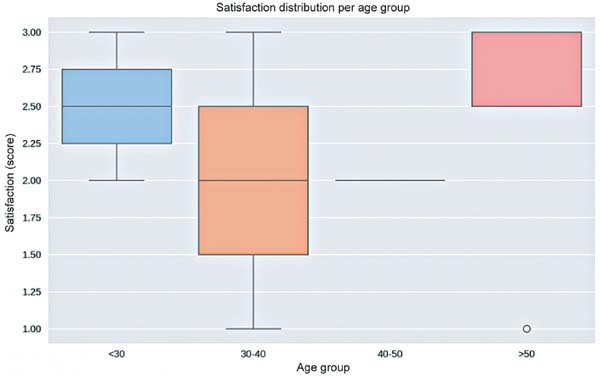
In our study, patients over 50 years old received more applications (mean: 4.0) (►Fig. 2). Patient satisfaction with the outcome was greater in the age groups under 30 and over 50 years of age (mean: 2.5) (►Fig. 3).


Discussion
The SICPHI is a reference center in a large city, serving patients from SUS. Although the population sample of SICPHI is heterogeneous, the epidemiological profile of the patients treated is consistent with data found in the literature, with more than 80% of subjects identifying as Black or Brown.
Our study demonstrated the predominance of women7 and Black/Brown subjects6,7 among the patients treated with TCN, reinforcing previous observations on the influence of ethnicity and gender factors on the predisposition to keloids. In this context, the work of Hochman et al. (2015)9 provided valuable insights. For instance, in 2015, these authors9 highlighted that the Black population has a higher density of fibroblasts and proliferative activity in the dermis, which could explain not only the higher incidence of keloids but also the variable response to treatments such as TCN. This biological perspective complements the epidemiological data presented here, suggesting that the association between ethnicity and keloids goes beyond environmental factors, involving intrinsic cellular mechanisms.
Moreover, Hochman et al. (2018)10 emphasized the importance of therapeutic strategies adapted to higher-risk groups, such as young women, who often report significant psychosocial impact due to the location of lesions in exposed areas. This finding corroborates the need for personalized treatment, as discussed in the current study. The need for tailored treatments is especially true considering that 88.2% of the sample consisted of women, many presenting with keloids in regions such as the inframammary fold and anterior chest. The integration of multimodal approaches, such as combining TCN with cryotherapy or laser therapy, as reported by Hochman et al. (2020)11 in relapsing cases, could enhance outcomes in populations with a high recurrence rate, such as the one analyzed here.
Regarding smoking, although some studies associate it with a risk factor for keloid development, our study did not observe that it increases the incidence of the condition.
Although its pathophysiology remains unclarified, research shows that keloids are more common in areas with greater skin tension. In our study, approximately 40% of the sample presented keloids in the thoracic region (anterior chest and inframammary fold).
In addition to the epidemiological findings, it is worth highlighting that the current guidelines for keloid treatment emphasize a multimodal approach, aiming to optimize outcomes and reduce recurrence. Although TCN is the first-line therapy, recent studies recommend its combination with other modalities, such as cryotherapy, laser therapy, pressure therapy, or 5-fluorouracil injections, especially in recalcitrant or high-risk cases.
The literature also indicates benefits in combining TCN with verapamil or surgical interventions, followed by adjuvant radiotherapy, for extensive keloids.4 Personalizing treatment, considering factors such as anatomical location, patient characteristics (including ethnicity and gender), and initial response to therapy, is crucial, as specific groups, such as female and Black/Brown patients, predominant in this sample, may be more predisposed to recurrence. Future studies with larger sample sizes could explore combined protocols by integrating epidemiological and therapeutic data to establish more robust and individualized strategies.
Although less than half of the sample completed the TCN treatment, it is noteworthy that no patient reported dissatisfaction with the outcome, and more than half of the participants noticed some improvement after the first application.
Conclusion
The epidemiological profile evaluated in the present study is consistent with data previously described in the literature. The main limitation of this study is its small sample size, even in a referral center in Brazil’s largest city.
For some authors, TCN is the first-line treatment for keloids. However, incorporating additional therapeutic references into future treatment protocols not only enhances engagement with the international literature but also emphasizes the importance of local studies. These studies can guide clinical protocols in specific contexts, such as within SUS, where accessibility and treatment adherence are significant challenges.
Although the current study did not aim to assess satisfaction rates or treatment responses, the epidemiological profile of patients did not appear to influence the success rates. Future research needs larger sample sizes to achieve more accurate assessments and stronger associations.
References
1. Liu R, Xiao H, Wang R, et al. Risk factors associated with the progression from keloids to severe keloids. Chin Med J (Engl) 2022;135(07):828-836. Doi: 10.1097/CM9.0000000000002093
2. Berman B, Maderal A, Raphael B. Keloids and Hypertrophic Scars: Pathophysiology, Classification, and Treatment. Dermatol Surg 2017;43(Suppl 1):S3-S18. Doi: 10.1097/DSS.0000000000000819
3. Lee HJ, Jang YJ. Recent understandings of biology, prophylaxis and treatment strategies for hypertrophic scars and keloids. Int J Mol Sci 2018;19(03):711. Doi: 10.3390/ijms19030711
4. Klomparens K, Simman R. Treatment of Keloids: A Meta-analysis of Intralesional Triamcinolone, Verapamil, and Their Combination. Plast Reconstr Surg Glob Open 2022;10(01):e4075. Doi: 10.1097/GOX.0000000000004075
5. Andrews JP, Marttala J, Macarak E, Rosenbloom J, Uitto J. Keloids: The paradigm of skin fibrosis - Pathomechanisms and treatment. Matrix Biology 2016;51:37-46. Doi: 10.1016/j.matbio.2016.01.013. PubMed
6. Téot L, Mustoe TA, Middelkoop Eet al. , (editors). Textbook on Scar Management: State of the Art Management and Emerging Technologies [Internet]. Cham (CH): Springer; 2020. Huang C, Wu Z, Du Y, Ogawa RChapter 4 - The Epidemiology of Keloids.
7. Robles DT, Berg D. Abnormal wound healing: keloids. Clin Dermatol 2007;25(01):26-32. Doi: 10.1016/j.clindermatol.2006.09.009
8. Reish RG, Eriksson E. Scar treatments: preclinical and clinical studies. J Am Coll Surg 2008;206(04):719-730. Doi: 10.1016/j. jamcollsurg.2007.11.022
9. Hochman B, et al. Keloid pathogenesis: A review with emphasis on immune system, collagen synthesis and apoptosis. An Bras Dermatol 2015;90(04):485-492
10. ”. J Eur Acad Dermatol Venereol 2018;32(12):e436-e438
11. Hochman B, et al. Combined therapy with intralesional triamcinolone and cryotherapy for recurrent keloids: A randomized controlled trial. Dermatol Surg 2020;46(12):1535-1541
1. Plastic Surgery Service, Hospital Ipiranga, São Paulo, SP, Brazil
Address for correspondence Gabriella Ueharo Pereira, Avenida Nazaré, 28, São Paulo, SP, CEP 04262-000, Brazil (e-mail: gabiueharo@gmail.com).
Artigo submetido: 20/01/2025.
Artigo aceito: 14/07/2025.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket