



Review Article - Year 2025 - Volume 40Issue 1
Z-Plasty in Unilateral Cheiloplasty: Evolution and Techniques
Zetaplastia em queiloplastia unilateral: Evolução e técnicas
Isabela Bicalho Zaki1, ; Ana Clara Rosa Coelho-Guimarães1; Marcelo Luiz Peixoto Sobral1; Vinchenzo Alberto de-Genaro1
; Ana Clara Rosa Coelho-Guimarães1; Marcelo Luiz Peixoto Sobral1; Vinchenzo Alberto de-Genaro1
ABSTRACT
Introduction: Cleft lip and palate is the most common congenital deformity among craniofacial malformations. The treatment of cleft lip patients has crucial stages, with several surgical techniques, among which the most used is the Millard I. Initially, Zplasty involved creating Z-shaped incisions along the edges of the cleft lip, but, eventually, more precise suturing techniques and absorbable suture materials started to be used in order to reduce tissue tension and enhance healing. The development of thesemodifications to the Z-plasty technique has led to better aesthetic and functional outcomes in unilateral cleft lip repair. Z-plasty has been extensively employed in unilateral cleft lips to achieve satisfactory aesthetic and functional results. The present study examines the most significant advances in Z-plasty technology and their impact on enhanced lip aesthetics and functionality.
Objective: The current study aimed to investigate the Z-plasty evolution in cheiloplasty, analyzing the technical developments achieved over time, focusing on improving aesthetic outcomes and restoring functionality in repaired unilateral cleft lips.
Materials and Methods: The article is a narrative summary from selected specific studies investigating the development of Z-plasty in cheiloplasty using electronic databases such as PubMed, LILACS, Scielo, and articles from the Brazilian Journal of Plastic Surgery (RBCP), and research on technical developments and the pros and cons of Z-plasty. Results Z-plasty is an effective and adaptable surgical technique, easily tailored to the demands of contemporary plastic surgery. Its remarkable evolution over the years demonstrates significant advances in aesthetic and functional outcomes, and new technical approaches are increasingly frequent to enhance the natural appearance of repaired lips.
Conclusion: Z-plasty has shown significant aesthetic and functional advancements in correcting unilateral cleft lips. Its adaptations improved symmetry and reduced the need for secondary surgeries. The technique selection must be careful, and a multidisciplinary approach is essential for optimal outcomes.
Keywords: cheiloplasty; cheilozetaplasty; cleft lip surgery; unilateral cleft lip; Z-plasty
RESUMO
Introdução: A fissura labiopalatina é a deformidade congênita mais frequente dentre as malformações craniofaciais. O tratamento do paciente portador da fenda labial temcomo etapas fundamentais, as cirurgias que possuem diversas técnicas e dentre elas, a de Millard ainda é a mais utilizada. Originalmente, a zetaplastia envolvia a criação de incisões em forma de Z nas bordas da fenda labial, mas também pode envolver o uso de técnicas de sutura mais precisas e materiais de sutura absorvíveis passou a ser usado para reduzir a tensão nos tecidos e melhorar a cicatrização. Essas modificações na técnica da zetaplastia foramdesenvolvidas para obter resultados estéticos e funcionais mais favoráveis no reparo de fenda labial unilateral. A zetaplastia tem sido amplamente utilizada nas fissuras labiais unilaterais com o objetivo de alcançar resultados estéticos e funcionais satisfatórios. Neste estudo, examinamos os avanços mais importantes na tecnologia da zetaplastia e seu impacto na estética e funcionalidade do lábio melhorado.
Objetivos: Investigar a evolução da zetaplastia na queiloplastia, analisando a evolução técnica alcançada ao longo do tempo, com foco na melhoria dos resultados estéticos e na restauração da funcionalidade do lábio reparado em fissura labial unilateral.
Materiais e Métodos: Revisão narrativa, com análise qualitativa e de natureza exploratória que utilizou como base de dados a EBSCO, SciELO e PubMed, valendose de fontes primárias e secundárias dos últimos cinco anos com acesso livre.
Resultados: A zetaplastia mostrou-se uma técnica cirúrgica efetiva e complacente, facilmente adaptada às demandas da cirurgia plástica contemporânea. Sua notável evolução ao longo de anos demonstra avanços significativos nos resultados estéticos e funcionais, e novas abordagens técnicas são cada vez mais frequentes para melhorar o aspecto natural do lábio reparado.
Conclusão: A zetaplastia tem avançado significativamente em termos estéticos e funcionais na correção de fissuras labiais unilaterais, com adaptações que melhoram a simetria e reduzem a necessidade de reoperações. A escolha da técnica deve ser cuidadosa, e uma abordagem multidisciplinar é crucial para resultados ideais.
Palavras-chave: cirurgia lábio leporino; fenda labial unilateral; zetaplastia; queiloplastia; queilozetaplastia
Introduction
Cleft lip and palate is the most common congenital craniofacial deformity. It presents in several forms and causes anatomical distortions in the upper lip, nose, and palate. It accounts for approximately 65% of malformations in the craniofacial region. Cleft lip patients require multidisciplinary treatment involving different surgical techniques as fundamental steps.1
The search for effective surgical procedures to correct facial deformities has been a constant throughout the history of medicine and plastic surgery. Among these procedures, Z-plasty emerged as a fundamental technique in treating unilateral cleft lips. The history of Z-plasty, often intrinsically linked to unilateral cheiloplasty, reflects the evolution of plastic surgery and the relentless pursuit of improving the quality of life of patients affected by this condition.2
Z-plasty is a versatile technique with potential application in several plastic surgery areas, including scar and facial deformity corrections, orthopedic repairs, breast reconstructions, cervicoplasties, and unilateral cleft lip corrections.3-9 Its geometric approach, versatility, and positive results make it a significant choice for plastic surgeons seeking to restore the appearance and function of facial structures. Z-plasty represents a critical advance in correcting facial deformities, providing visible and tangible improvements in the quality of life of affected patients.3
By exploring the practical application, benefits, and limitations of Z-plasty in unilateral cheiloplasty, including the variations introduced by renowned surgeons and different techniques, the present study aimed to shed light on how these methods contributed to unilateral cleft lip correction and improved the quality of life of affected patients.
Objective
The current study aimed to assess the evolution of Z-plasty techniques in unilateral cleft lip correction and their advantages and disadvantages.
Materials and Methods
This narrative review assessed the evolution and techniques used in Z-plasty applied to unilateral cheiloplasty. The methodology had the following steps:
1. Definition and objective: We selected the topic of Z-plasty in unilateral cheiloplasty due to its relevance in reconstructive plastic surgery, seeking to understand the evolution of the techniques and their clinical applications. The primary objective was to describe and critically analyze the main techniques and innovations in Z-plasty over the years.
2. Inclusion and exclusion criteria: We included articles, books, theses, and reviews published in Portuguese, English, and Spanish addressing Z-plasty applied to unilateral cheiloplasty. There was no restriction regarding the publication period, allowing a comprehensive analysis of the historical and contemporary evolution of the technique.
3. Search strategy: We performed the literature search in the electronic databases PubMed, Scielo, Lilacs, and Google Scholar. The descriptors included combinations of keywords such as zetaplasty, unilateral cleft lip, evolution of surgical techniques, reconstructive plastic surgery, Z-plasty, cheiloplasty, cleft lip, unilateral, and cleft lip surgery. We used Boolean search strategies to increase the sensitivity and specificity of the results.
4. Study selection: Initially, we evaluated titles and abstracts to verify the relevance to the topic, such as articles published and indexed over the years focusing on the history and evolution of Z-plasty, surgical treatment for unilateral cleft lip, new techniques associated with cheilozetaplasty, literature reviews, and case reports. Then, we read the full texts of potentially eligible studies to confirm their inclusion in the review-we analyzed 38 articles, and we excluded 15 because they meet the criteria, selecting 10 to compose ►Table 1 (see below). We excluded studies not directly addressing Z-plasty in unilateral cheiloplasties, such as those reviewing techniques associated with rhinoplasty or not presenting sufficient data for critical analysis. The research notes were in English and Portuguese, and the articles were available in full.
5. Data analysis: The selected studies underwent a qualitative analysis. We performed a narrative synthesis, grouping the information by historical periods and specific Z-plasty techniques. We discussed the evolution of the procedures concerning functional and aesthetic improvements and the technical challenges faced by surgeons.
This methodology allowed a comprehensive understanding of the development of Z-plasty techniques applied to unilateral cheiloplasty, offering a critical view of surgical practices and their clinical implications.
Results
The analysis of the selected studies revealed that Z-plasty has evolved significantly over the years, adapting to the contemporary needs of reconstructive plastic surgery. New technical approaches improved lip symmetry and functionality, reducing the need for reoperations.
We selected seven articles based on their relevance to the technical evolution and clinical practice of Z-plasty, seeking to highlight studies discussing:
Innovations in surgical technique;
Specific applications in the context of unilateral cleft lip repair;
Comparisons between different technical approaches;
Aesthetic and functional outcomes, including success rates and need for secondary surgeries.
Table 1 details each selected article, specifying its objectives and main findings to allow a clear understanding of the impact of Z-plasty on the evolution of unilateral cleft lip repair.
| Author (year) | Objectives | Results |
|---|---|---|
| Carreirão et al.11 (2021) | Clarify and disseminate the history of cheilozetaplasty in unilateral cleft lip and palate treatment. | The study emphasized principles such as cupid’s bow preservation, adequate alignment of the cutaneous-mucosal line, minimal lip tissue resection, and healing with no retraction tendency. |
| Anger and Sertorio3 (2006) | Characterize the effectiveness of the lengthening obtained through Z-plasty and muscle reconstruction in patients with unilateral cleft lip and palate. | The study revealed an actual gain after muscle treatment compared with initial measurements and a new effective gain after Z- plasty. |
| Lopes et al.14 (2017) | Evaluate the Millard technique associated with a mucosal Z-plasty, which is appropriate if the number of secondary surgeries (reoperations) is low. | The study showed that 15% of cases had “unsatisfactory outcomes” and underwent reoperation due to lip notch or enlarged scar. Meanwhile, 85% of the remaining patients did not require secondary surgery and had “satisfactory outcomes.” |
| Worley et al.13> (2018) | Clarify and disseminate cleft palate and cleft lip, their surgical management, and the conduct. | The study revealed a high risk of hearing complications and speech disorders requiring a multidisciplinary team after orofacial cleft correction. |
| Rossell-Perry12 (2020) | Clarify and demonstrate an innovative technique for unilateral cleft lip with severe soft tissue deficiency surgical correction. | The study showed that this method allowed the surgeon to obtain adequate upper lip symmetry. The surgical technique proposed by the author led to a low revision rate (14.88%) over 13 years. |
| Sales et al.19 (2016) | Report a clinical case of unilateral cheiloplasty using the Fisher technique. | The Fisher technique demonstrated favorable aesthetic outcomes, with scars on the philtrum crest, and good functional outcomes if the positioning of the orbicularis or cupid’s bow muscles is correct. |
| Rossel-Perry2 (2016) | Compare the surgical outcomes of different surgical techniques for unilateral cleft lip repair. | The study revealed the lack of differences in outcomes between the Millard and Reichert-
Millard techniques for unilateral incomplete cleft lip. For complete unilateral cleft
lip and lower tissue deficiency, lip symmetry was better using superior rotation advancement
plus double unilimb Z-plasty than the Reichert-Millard technique. For complete unilateral
cleft lip and higher tissue deficiency, lip symmetry was better after triple unilimb Z-plasty than superior rotation advancement plus double unilimb Z-plasty. |
| Tse16 (2012) | Explore surgical principles and management techniques for unilateral cleft lip correction, highlighting methods such as the Millard and Fisher techniques. | The article emphasized that the Millard technique, based on rotation and advancement, preserves the structure of the philtrum but may present aesthetic limitations in wider clefts. In contrast, the Fisher technique uses anatomical subunit approximation, providing less visible scars and better aesthetic symmetry, and is effective even in complex cases. The study also highlighted the importance of preoperative molding and continuous reassessment for better long-term outcomes. |
| Adetayo et al.17 (2019) | Compare the surgical outcomes of two techniques for repairing unilateral cleft lips, i.e., Tennison-Randall and Millard, based on the qualitative outcome evaluation performed by patients, guardians, and professionals. | The study showed that both techniques are effective but present different aesthetic challenges. Patients undergoing the Tennison-Randall technique were more dissatisfied with lower lip scars, while those treated with the Millard technique reported greater dissatisfaction with scars near the nose. The Millard technique led to more asymmetrical noses and deviated columellae, but there was a consensus that both techniques need improvements to reduce scars and optimize aesthetic and functional outcomes. |
| ElMaghraby et al.18 (2021) | Compare the Fisher technique of anatomical subunits approximation with the Millard technique of rotation and advancement in unilateral cleft lip repair, evaluating the aesthetic and functional outcomes using Steffensen criteria. | The comparison showed that the Fisher technique offers better aesthetic results, with more discreet scars and better symmetry of the cupid’s bow and alar base. Although there was no significant difference in anthropometric measurements (lip height, width, etc.), the scar appearance was superior with the Fisher technique, leading the authors to recommend its use in unilateral cleft lips. |

These studies highlighted Z-plasty as an essential and effective technique in unilateral cleft lip repair, particularly due to innovations such as double and triple unilimb Z-plasty. These variations have improved the symmetry of the upper lip and reduced the need for reoperations. Rossell- Perry2 (2016) suggested adapting the choice of technique to the cleft complexity and tissue availability. In contrast, Carreirão et al.11 (2021) emphasized sparing the cupid’s bow and aligning the cutaneous-mucosal line to minimize retractions and optimize aesthetic results.
Worley et al.13 (2018) highlighted the importance of a multidisciplinary approach due to the complexity of cleft lip and palate and the complication risk. Comparing different techniques, Tse16(2012) noted that although the Millard technique effectively spares the philtrum, it faces aesthetic limitations in more severe cases. On the other hand, the Fisher technique, which focuses on approximating the anatomical subunits, resulted in smaller scars and better symmetry.ElMaghrabyetal.18 (2021)reinforcedthese advantages, recommending the Fisher technique for its aesthetic superiority even in complex situations. Adetayo et al.17 (2019) also pointed out specific challenges of the Tennison-Randall and Millard techniques, highlighting the variation in patient satisfaction based on the scar appearance and location.
Discussion
Congenital cleft lip is a deformity resulting from genetic or environmental factors during the early development of the jaw and palate. The non-syndromic form has a multifactorial etiology, potentially linked to maternal exposure to teratogens, such as tobacco. It accounts for 65% of craniofacial malformations, and its treatment is multidisciplinary, involving several surgical techniques to restore feeding abilities, speech development, and facial aesthetics to avoid future complications.10
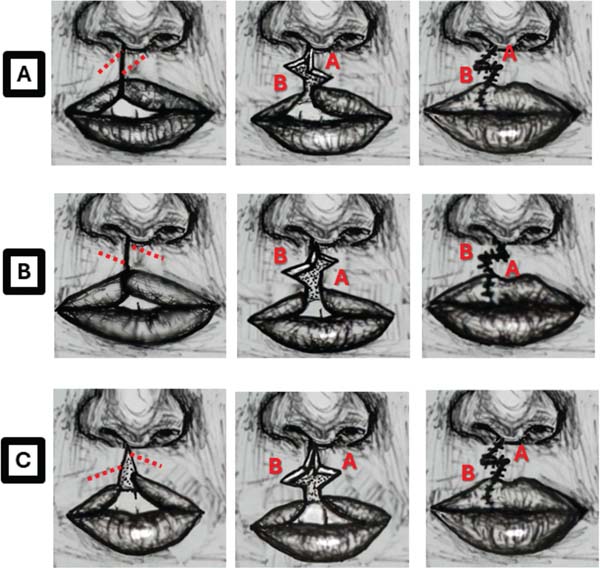
Z-plasty dates back to the 19th century with Horner (1837), followed by Denonvilliers (1863) and Berger (1904), who expanded its use. McCurdy (1913) formalized the term, and, in 1956, Perseu Castro de Lemos improved the technique, focusing on preserving the cupid’s bow and avoiding scar retractions. Lemos became a reference in Brazil and received international recognition in 1967. Z-plasty remains essential in reconstructive surgery11 (►Fig. 1).

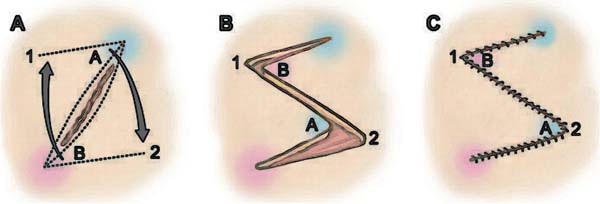
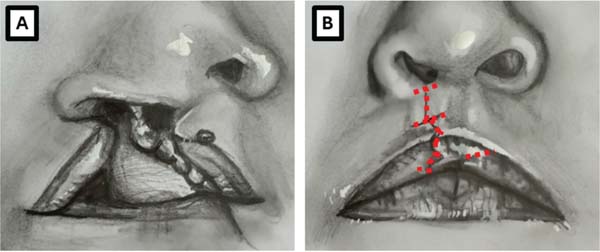
Z-plasty is a surgical technique to correct facial deformities by creating “Z” or “zig-zag” shaped flaps to reorganize and reconstruct soft tissues. It relies on geometric principles and aims to improve the aesthetics and functionality of the treated area11 (►Fig. 2).

Its versatility allows its application to the upper, middle, or lower thirds of the lip, adapting to the anatomy and needs of the patient. In addition, it minimizes tissue removal, resulting in smaller scars and aesthetic symmetry. Compared with more complex techniques, it is relatively easy to perform, offering good aesthetic and functional outcomes.12,13 It is possible to adapt and associate the Z-plasty technique with other surgical approaches, such as the Fischer or Millard techniques, allowing greater procedural customization according to each patient’s specific requirement.14
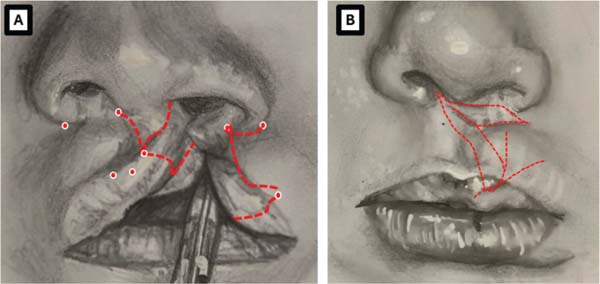
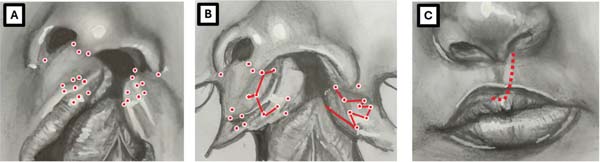
Millard originally introduced the rotation-advancement approach, which involves creating a rotation flap in the medial portion of the sulcus and an advancement flap starting at the lateral portion of the sulcus. The advantages of this technique include the formation of suture lines to restore the fissure philtrum, the potential to access the tip cartilage for nasal reconstruction, and the flexibility for intraoperative adjustments. The disadvantages include the potential for nasal stenosis and suture-related issues (►Figs. 3-5).



The main advantages of this innovative technique are sparing the lip tissue, improving the lateral segment deficiency, and using similar tissue for lip and nasal repair. The main disadvantage is the difficulty of secondary repair due to multiple scars.12
The Millard technique, commonly used for unilateral cleft lip correction, involves rotation and advancement to spare the philtrum and minimize tissue resection. However, its effectiveness decreases in wider clefts, which may result in subtle asymmetry or lip shortening. The Mohler modification improves this approach by extending the incision to the columella, increasing rotation, and promoting better lip symmetry. The Fisher technique, focused on anatomical precision with detailed markings, provides less visible scars and superior aesthetic outcomes even in complex cases.16
In addition to the Millard variations, the Mohler technique optimizes lip and nasal symmetry and extends the incision to allow better rotation. Muscle release is essential for correct tissue positioning and facilitate lip functionality. This threedimensional approach reduces tension and improves lip and nose reconstruction. Preoperative preparation is crucial, especially in complex unilateral clefts with nasal involvement.17
Comparison between the Fisher and Millard techniques shows that the Fisher anatomical subunit approach has advantages, such as better-positioned scars and lower visibility. The Fisher technique offers better lip symmetry and a lower risk of future deformities, especially at the alar base and vermilion. Although anthropometric measurements are similar in both methods, the Fisher technique receives superior aesthetic evaluations due to the better alignment of the cupid’s bow and a more natural scar appearance.18
Conclusion
Z-plasty, widely used in unilateral lip repair, has shown significant aesthetic and functional advances throughout its evolution. The study highlights the importance of adaptations, such as double and triple unilimb Z-plasty, which improve lip symmetry and reduce the need for secondary interventions. Comparisons between techniques, such as Millard and Fisher, show that the surgical choice should consider the cleft complexity and the amount of tissue available, with the Fisher technique showing superiority in symmetry and aesthetic healing. Cupid’s bow preservation and adequate alignment are essential to minimize retractions. A multidisciplinary approach is essential due to the risk of complications, such as nasal deformities and oral dysfunctions. Thus, Z-plasty remains a pillar in reconstructive plastic surgery, with continuous refinements seeking excellence in outcomes for patients with unilateral cleft lips.
REFERENCES
1. Spencer LSDB, Buzzo CL. Tratamento primário da deformidade labial e nasal nas fissuras labiais e labiopalatinas unilaterais. Rev Bras Cir Plást 2017;32(01):37-45 10.5935/2177-1235.2017RBCP0006
2. Rossell-Perry P. A 20-year experience in unilateral cleft lip repair: From Millard to the triple unilimb Z-plasty technique. Indian J Plast Surg 2016;49(03):340-349. Doi: 10.4103/0970-0358.197226
3. Anger J, Sertorio CB. Avaliação das Medidas do Alongamento do Lábio nas Queiloplastias com Plástica em Z no Tratamento das Fissuras Labiopalatinas Unilaterais. Rev Bras Cir Plást 2006;21(03):133-139
4. Barreiros H, Goulão J. Z-Plasty: useful uses in dermatologic surgery. An Bras Dermatol 2014;89(01):187-188. Doi: 10.1590/abd1806-4841.20142298 PubMed
5. Chen B, Song H. The Modification of Five-Flap Z-Plasty for Web Contracture. Aesthetic Plast Surg 2015;39(06):922-926. Doi: 10.1007/s00266-015-0548-y PubMed
6. Bae DS. Z-plasties for the Pediatric Orthopaedic Surgeon. Journal of the Pediatric Orthopaedic Society of North America 2023;5(3): 700, ISSN 2768-2765, . Doi: 10.55275/JPOSNA-2023-700
7. Garg S, Dahiya N, Gupta S. Surgical scar revision: an overview. J Cutan Aesthet Surg 2014;7(01):3-13. Doi: 10.4103/0974-2077.129959 PubMed
8. Koc MN, Orbay H, Uysal AC, Unlü RE, Sensöz O. Z plasty closure of lower lip defects after tumor excision. J Craniofac Surg 2007;18(05):1120-1124. Doi: 10.1097/scs.0b013e3180-de615d PubMed
9. Moraes MARd, Ramos RR, Ferreira LM. Z-plasty in axillary retraction: techniques and strategies to facilitate learning by medical residents. Rev Bras Cir Plást 2017;32(02):241-244 10.5935/2177-1235.2017RBCP0038
10. Shkoukani MA, Chen, M, Vong A. Cleft lip - a comprehensive review. Front Pediatr 2013;1(53):•••. Doi: 10.3389/fped.2013.00053 PubMed
11. Carreirão S, Azem LL, Menezes RS, Zraik LB. Plástica em Z no tratamento da fissura labial unilateral: revisão de sua história. Rev Bras Cir Plást 2021; 36(4):490-495. Doi: 10.5935/2177-1235.2021RBCP0029
12. Rossell-Perry P. The Triple Unilimb Z Plasty Technique for Severe Forms of Unilateral Cleft Lip Repair. Plast Reconstr Surg Glob Open 2020;8(10):e3213. Doi: 10.1097/GOX.0000000000003213
13. Worley ML, Patel KG, Kilpatrick LA. Cleft Lip and Palate. Clin Perinatol 2018;45(04):661-678. Doi: 10.1016/j.clp.2018.07.006 PubMed
14. Lopes DdC, Cano AFC, Gobetti L, Menegazzo MR, Saldanha O. Avaliação da técnica de Millard associada à zetaplastia no tratamento de portadores de fenda labial unilateral. Rev Bras Cir Plást 2018;33(1) 82-88 10.5935/2177-1235.2018RBCP0012
15. Miachon MD e Leme PLS. Tratamento operatório das fendas labiais. Rev Col Bras Cir 2014;41(3): 208-214,. ISSN 1809-4546. Doi: 10.1590/S0100-69912014000300013 PubMed
16. Tse R. Exploring Surgical Principles and Management Techniques for Unilateral Cleft Lip Repair: Highlighting Millard and Fisher Methods. . J Craniofac Surg 2012
17. Adetayo AM, Adetayo MO, Adeyemo WL, James OO, Adeyemi MO. Comparison of Surgical Outcomes Between Tennison-Randall and Millard Techniques for Unilateral Cleft Lip Repair: Qualitative Assessment by Patients and Professionals. J Craniofac Surg 2019; 45(03):1128999
18. ElMaghraby MF, Ghozlan NA, Ashry MH, Abouarab MH, Farouk A. Comparative study between fisher anatomical subunit approximation technique and millard rotation-advancement technique in unilateral cleft lip repair. Alex J Med 2021;57(1):92-102 10.1080/20905068.2021.1885954
19. Sales PHdH Rocha SSd, Albuquerque AFM, Cunha Filho JFd. Queiloplastia primária unilateral através da técnica de Fisher. Rev. Odontol. Univ. Cid. São Paulo 2016;28(2): 148-154 10.26843/ro_unicid.v28i2.225
1. School of Medicine, Centro Universitário das Américas (FAM), São Paulo, SP, Brazil
Address for correspondence Isabela Bicalho Zaki, Faculdade de Medicina, Centro Universitário das Américas (FAM), Medicina, São Paulo, SP, 01304-001, Brazil (e-mail: isabicalhozaki@gmail.com).
Article received: April 09, 2024.
Article accepted: February 06, 2025.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket