



Articles - Year 2001 - Volume 16 -
The Rhomboid Flap for Immediate Breast Reconstruction Post Quadrantectomy and Axillary Dissection
Retalho Rombóide na Reparação Mamária Imediata Pós-Quadrantectomia e Dissecção Axilar
ABSTRACT
The authors describe their experience in immediate breast reconstruction using the Limberg rhomboid flap post-quadrantectomy and axillary dissection. They report the technique in 200 cases, operated from June 97 to June 2000, describing the methodology used, indication of the best quadrants, results and complications.
Keywords: Rhomboid flap; quadrantectomy; axillary dissection; breast cancer
RESUMO
Os autores apresentam sua experiência com o uso do retalho rombóide de Limberg nas reparações mamárias imediatas pós-quadrantectomia e dissecção axilar. Relatam a utilização em 200 casos operados no período de junho de 97 a junho de 2000, descrevendo a metodologia da técnica utilizada, melhores quadrantes para indicação, resultados e complicações.
Palavras-chave: Retalho rombóide; quadrantectomia; dissecção axilar; câncer de mama
Plastic surgery has become a fundamental part of breast cancer treatment. An interdisciplinary approach provides the patient, undergoing breast reconstruction or repair, an enhanced guality of life(5).
Quadrantectomy, understood as the resection of a breast guadrant, followed by axillary dissection and postoperative radiotherapy, has shown a prognosis similar to mastectomies. Its main objective is maximum local control, with minimum mutilation. It was widely promoted by Veronesi in the eighties and in many cases, its use is clearly indicated(7).
There are frequently three types of breast deformities secondary to quadrantectomies, classified by Berrino as Types I to III: deviation or distortion of the nippleareola complex, tissue deficiency (gland and/or skin) and breast retraction, respectively(1). Various techniques have been recommended for immediate or late repair, from primary suture to skin glandular or myocutaneous flaps(2,3,4,6).
In the present study, the authors present their experience with immediate breast repair with a rhomboid skin flap, compare the latter with previously used methods and describe the extent of the corrections obtained.
PATIENTS AND METHODS
Two hundred patients with an average age of 52 years were submitted to immediate breast repair post quadrantectomy and axillary dissection, from June 97 to Iune 2000. A rhomboid, cutaneous-glandular or cutaneous-fat projected flap, similar to a Limberg flap, was used.
The surgical procedure consists of idemifying the projection of the tumor on the skin, then marking a diamond around the lesion, whose margins are determined by the specialist. Afterwards, the rhomboid flap to be used is also marked (Fig. 1). Skin and subcutaneous tissue are incised to the muscular plane and detachment is performed to allow complete rotation (Fig. 2). Synthesis consists of fixing the flap base to the subcutaneous tissue of the upper margin of the area to be repaired in order to better support the flap and skin suture (Fig. 3).
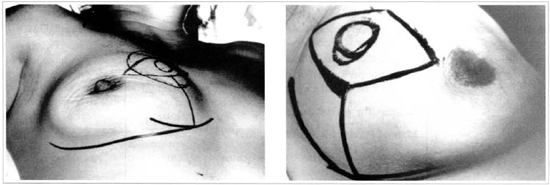
Fig. 1 - Delimitation of the projection of the rumor on the skin, diamond shaped marking around the lesion and the rhomboid flap, with a breast-oriented pedicle.
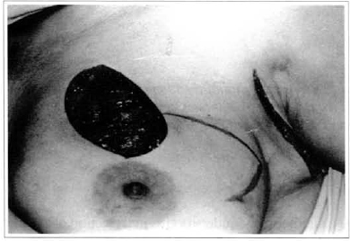
Fig. 2 - Resected tumor and post-quadrantectomy resulting area.
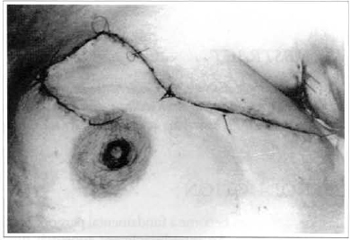
Fig. 3 - Positioned and sutured flap.
The tumors resected were located in the following quadrants: superior external (45%), inferior external (25 %), superior internal (15 %), and inferior internal (15%). Axillary emptying was performed with a single incision in the tumors of external quadrants and with a combined incision in the internal quadrant tumors.
All cases were drained with a continuous aspiration drain, which was leftin for an average period of 8 days.
Patients generally began radiotherapy in the third postoperative week.
RESULTS
The rhomboid flap allows the breast contour to be maintained in practically all cases, attenuating or even avoiding secondary deformities (Fig. 4).
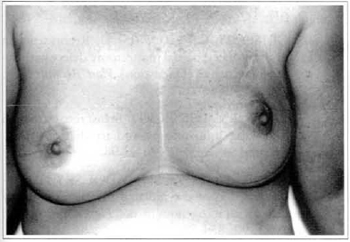
Fig. 4 - Later results, with acceptable symmetry.
The patient's subjective assessment of the aesthetic aspect is always positive.
Tissue redundancy is commonly observed at the anterior axillary line for two reasons: delivery of the latissimus dorsi from the thoracic wall, during surgery, and to late lymphatic edema caused by axillary emptying. The alteration can be attenuated with one of the segments of the rhomboid flap (Fig. 5).
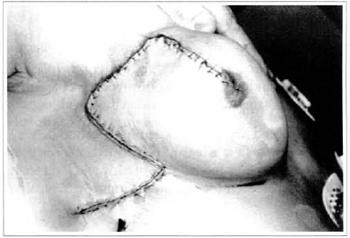
Fig. 5 - Correction of skin redundancy ar the anterior axillary line by rorating one of the flap segments.
Although the scar is large, it is a good quality scar in the long term, possibly due to postoperative radiotherapy (Figs. 6 and 7).
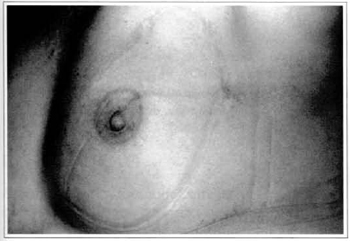
Fig. 6 - Post radiotherapy scar aspect.

Fig. 7 - Scar detail.
The mammary groove is not distorted in the external quadrants, although there is a slight constriction of the groove in relation to the internal inferior quadrant. It can be corrected later, without technical difficulties.
The author prefers to have a contralateral balance at a second stage, as the degree of post radiotherapy mammary reduction is quite variable.
CONCLUSION
Conservative surgery has been increasingly employed and the methods used are aesthetically-oriented(2-6).
The author has had a great deal of experience using procedures such as primary suture, zigzag plastic, gland flaps and muscular and/or myocutaneous latissimus dorsi flaps, as recommended by Slavin(1,6).
The rhomboid flap has been demonstrated to be very versatile because it is easily performed, it preserves the breast contour, and because of early and long term results. It has been the option for immediate repairs.
REFERENCES
1. SACCHINI V, NAVAM, TANA S, et al. Quantitative and qualitative cosmetic evaluation after conservative treatment for breast Cancer. Eur. J. Cancer. 1991; 27: 1395-400.
2. VERONESI U, SACCOZZI R, DELVECCHIO M, et al. Comparing radical mastectomy with quadrantectomy, axillary dissection and radiotherapy in patients with small cancer of breast. N. Engl.J. Med. 1981; 305: 6-11.
3. BERRINO P, CAMPORA E, SANTI P. Postquadrantectomy breast deformities: classification and techniques of surgical correction. Plast.Reconstr. Surg. 1987; 79: 567-80.
4. COOPERMAN AM, DINNER M. The rhomboid flap and partial mastectomy. Surg. Clin. North Am. 1978; 58: 869-71.
5. GRISOTTI A, VERONESI U. Reconstruction of the radiated partial mastectomy defect with autogenous
tissues (Discussion). Plast. Reconstr Surg.1992; 90: 866-76.
6. PEARL RM, WISNICKI J. Breast reconstruction following lumpectomy and irradiation. Plast. Reconstr. Surg. 1985; 76: 83-98.
7. SLAVIN SA, LOVE SM, PADOUSKY NL. Reconstruction of the radiated partial mastectomy defect with autogenous tissues. Plast. Reconstn Surg.1992; 90: 854-73.
I - Senior Member of the Brazilian Society of Plastic Surgery, Professor of Anatomy at the Uberaba University School of Medicine.
II - Senior Member of the Brazilian Society of Plastic Surgery. Responsible for Plastic Surgery Services at FMTM.
III - Member of the Brazilian Society of Mastology.
IV - Senior Member of the Brazilian Society of Plastic Surgery, Associate Professor of Plastic Surgery at FMTM.
Study performed at Associação de Combate ao Câncer do Brasil Central - Hélio Angotti Hospital
Address for correspondence:
Manoel Pereira da Silva Neto, MD
R. Governador Valadares, 619 - Centro
38010-380 - Uberaba - MG Brazil
Phone: (55 34) 312-0692 - Fax: (55 34) 312-9687
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket