



Review Article - Year 2024 - Volume 39 -
Is It Feasible to Use Negative-pressure Wound Therapy to Treat Complex Wounds within the Brazilian Unified Health System?
Há espaço para o uso de terapia por pressão negativa no tratamento de feridas complexas de pacientes do SUS?
Felipe Andrade Lopes1 ; Mariana Fernandes Inácio1; Giovanna Cavalcanti Banov1; Julia Innocenti Dinhane Salum1; Alexandre Venâncio Sousa1; Luis Felipe Maatz Ramos1
; Mariana Fernandes Inácio1; Giovanna Cavalcanti Banov1; Julia Innocenti Dinhane Salum1; Alexandre Venâncio Sousa1; Luis Felipe Maatz Ramos1
ABSTRACT
Objective Complex wounds are difficult-to-manage injuries that generate high patient morbidity and mortality and have shown a significant increase in prevalence. Due to their high institutional cost, there is a search for technologies that can accelerate the healing process. Therefore, negative pressure wound therapy (NPWT) emerges as a treatment option. The present study aimsto review the literature on the use ofNPWT in the treatment of complexwounds, to evaluate its adoption and create a proposal for guidance on how this technique can be applied in the treatment of patients hospitalized in the Brazilian Unified Health System (Sistema Único de Saúde - SUS, in Portuguese).
Materials and Methods The current integrative literature review is characterized by a qualitative focus and an exploratory context. The search was conducted across PubMed, Scientific Electronic Library Online (SciELO), and Academic Google databases. Specific keywords, wounds and injuries, wound closure techniques, negative-pressure wound therapy, and wound healing, were used. Inclusion criteria encompassed original articles and systematic reviews published between 2002 and 2022 in Portuguese, English, or Spanish, focusing on NPWT. Exclusions included unrelated topics, incomplete texts, basic forms of NPWT (without patent), studies from vacuum-assisted closure (VAC) manufacturing industries, and articles in which VAC was not employed for the closure of complex wounds.
Conclusion Despite the significant costs associated with vacuum therapy, this technique has demonstrated effectiveness in reducing healing time, hospitalization length, and consequently alleviating the overall financial burden of treating complex wounds. Simultaneously, it has the potential to significantly improve the quality of life for affected patients.
Keywords: negative-pressure wound therapy; Unified Health System; wound closure techniques; wound healing; wounds and injuries
RESUMO
Objetivo Feridas complexas são lesões que geram uma alta morbimortalidade ao paciente e têm apresentado um aumento significativo de prevalência. Devido ao seu alto custo de tratamento, há busca por tecnologias que acelerem seu processo de cura, destacando-se a terapia por pressão negativa (TPN). O presente estudo objetiva revisar a literatura sobre o uso da TPN no tratamento de feridas complexas, para avaliar sua adoção e criar uma proposta de orientação de como essa técnica pode ser aplicada no tratamento de pacientes hospitalizados no Sistema Único de Saúde (SUS).
Materiais e Métodos Esta revisão integrativa da literatura, de enfoque qualitativo, foi pesquisada nas bases de dados PubMed, Scientific Electronic Library Online (SciELO) e Google Académico. Foram utilizadas as palavras-chave: feridas e lesões, técnicas de fechamento de feridas, terapia por pressão negativa em feridas e cicatrização de feridas. Foram incluídos artigos originais e revisões sistemáticas publicados entre 2002 e 2022 em português, inglês ou espanhol, com foco na terapia de fechamento de feridas por pressão negativa. Foram excluídos tópicos não relacionados, textos incompletos, formas básicas de TPN (sem patente), estudos de indústrias de fabricação do dispositivo e artigos em que a TPN não foi utilizada para o fechamento de feridas complexas.
Conclusão Apesar dos custos significativos, a TPN demonstrou uma eficácia na redução do tempo de cicatrização e de internação, consequentemente, no alívio da carga financeira global do tratamento de feridas complexas. Ao mesmo tempo, ela tem o potencial de melhorar significativamente a qualidade de vida dos pacientes afetados.
Palavras-chave: cicatrização; ferimentos e lesões; Sistema Único de Saúde; técnicas de fechamento de ferimentos; tratamento de ferimentos com pressão negativa
Introduction
The skin is the body's largest organ, composed of the epidermis, dermis, and hypodermis. An average-sized person has ~ 2 m2 of skin with an average thickness of 2 mm. Despite its seemingly simple appearance, numerous important physiological processes occur to maintain its integrity, resulting in a layer that provides protection, immunity, and temperature regulation.1
When the layers of the skin or organs are compromised by various traumas, injuries known as wounds are formed, and may evolve into complex wounds. Treating these wounds poses a significant public health challenge that affects all strata of the population, presenting a significant difficulty for healthcare professionals and the healthcare system itself, which must allocate human, material, and financial resources to address this issue.2
The search for methods that promote wound healing has persisted for thousands of years. In prehistoric times, wounds were treated with herbal dressings to control bleeding and promote healing.3,4 By the late nineteenth and early twentieth centuries, antiseptics were introduced, and in the twentieth century, nurse Florence Nightingale observed that cleansing with pure water, efficient drainage of secretions, and proper lighting could aid in the healing of infected wounds. These methods have since become integral to healthcare practices.5
Currently, dressings are applied using sterile materials, and wound care follows the concept of asepsis, using antiseptics and materials applied directly to wounds to facilitate healing, prevent complications, absorb secretions, provide physical protection to wounds, and enhance patient comfort.1
In 1997, during the American Wound Care Congress, a novel wound care concept was introduced: vacuum-assisted closure (VAC). Its mechanism of action involves applying negative pressure (sub-atmospheric) to the wound to remove excess fluids, enhance vascularization, and reduce bacterial colonization, thereby increasing cellular mitosis and growth factor production.6
While VAC has been shown to reduce hospitalization time and complication risks in patients with complex wounds, there is still limited availability and utilization of this method for complex wound patients within the Brazilian Unified Health System (Sistema Único de Saúde – SUS, in Portuguese).7
Numerous patients endure complex wounds that are challenging to treat, often taking weeks, months, or even years to heal. During this period, patients suffer for various reasons: pain, secondary infections, inability to work, the necessity for frequent wound care appointments, or complications arising from these complex wounds. Therefore, a widespread utilization of vacuum dressings could prove beneficial in reducing the time spent on treatment and hospitalization for patients with complex wounds. Consequently, this could decrease the number of hospital admissions, alleviate the burden on hospitals and professionals managing such wounds, and reduce SUS costs.8 Thus, the question of cost-effectiveness and the feasibility of developing a protocol to facilitate the recommendation for the use of this treatment within SUS, as opposed to conventional dressings, is raised.
Within this framework, the purpose of the present study was to conduct a literature review on the treatment of complex wounds using vacuum-assisted dressings, exploring the cost-effectiveness of this treatment approach. Additionally, the study aimed to propose a protocol to facilitate the recommendation and implementation of vacuum-assisted dressings for patients admitted to public healthcare services under SUS.
Materials and Methods
For this current integrative literature review, an applied and exploratory bibliographic search was conducted using a qualitative approach. Electronic databases were searched, aiming to summarize data to provide a comprehensive understanding of the utilization of vacuum-assisted dressings.
The approach involving the use of vacuum-assisted dressings and a comparison with traditional dressings led to the formulation of a guiding research question: Is there a place for vacuum-assisted dressings in the treatment of complex wounds in SUS patients? This question was derived from the PICO strategy, wherein the theme encompassed four elements: (P) patient – patients with complex wounds; (I) intervention and approach – treatment of complex wounds using vacuumassisted dressings, (C) comparison – treatment of complex wounds using vacuum-assisted dressings compared with conventional treatments for complex wounds; and (0) outcome – treatment effectiveness and cost-benefit analysis.
Data Collection
Data were collected from the PubMed, Scientific Electronic Library Online (SciELO), and Google Scholar databases using the descriptors: wounds and injuries; wound closure techniques; and negative-pressure wound therapy; in Portuguese, English, and Spanish. Original articles, systematic reviews, meta-analyses, book chapters, and case reports published within a 20-year timeframe—from 2002 to 2022—were included if they aligned with the theme and discussed patented vacuum-assisted dressings. Studies not related to the theme, incomplete texts, discussions of simplified vacuum-assisted dressings, industry-authored works, studies not using vacuum-assisted dressings for complex wounds, and studies published before 2002 were excluded.
Data Analysis
To synthesize and interpret results, analyses were performed in a manner that focused on studies meeting the inclusion criteria and those employing approaches encompassing the cost of the treatment material, the patient care infrastructure (medical and nursing staff, hospitalization costs, and potential complications), patient improvement over time, and wellbeing. This selection process grouped and summarized evidence from these publications.
Results
A total of 10 studies were collected (►Fig. 1), all of which addressed the theme.


These studies provided a comprehensive understanding of the topic by presenting a brief historical context, outlining the mechanism of utilization, discussing advantages and disadvantages, and comparing the approach to conventional dressing methods (►Table 1). This information was instrumental in formulating a protocol delineating patient needs in relation to the two types of dressings under consideration.
| TITLE | AUTHOR, YEAR | STUDY DESIGN | OBJECTIVE | MAIN RESULTS |
|---|---|---|---|---|
| Terapia por pressão negativa no tratamento de feridas ("Negative Pressure Therapy in the Treatment of Wounds")7 | Dos Santos et al., 2019 | Review article | Search the literature for evidence on the use of negative-pressure wound therapy in the treatment of wounds. | Negative-pressure wound therapy has revolutionized wound treatment, particularly in the management of complex wounds, by aiding in reducing wound closure time and hospitalization time. |
| Terapia por pressão negativa no tratamento de feridas complexas ("Negative Pressure Therapy in the Treatment of Complex Wounds")9 | Lima et al., 2017 | Review article | Assess the effectiveness of negative- pressure wound therapy in treating complex wounds, with a focus on its mechanisms of action and key therapeutic indications. | Negative-pressure wound therapy should be included in the therapeutic toolkit of surgeons for treating a wide range of complex wounds. |
| Subatmospheric pressure therapy in the treatment of traumatic soft tissue injuries11 | Milcheski et al., 2013 | Descriptive study | To evaluate the use of subatmospheric pressure therapy in the treatment of acute traumatic injuries of the soft tissues, especially in the limbs. | SPT significantly reduced morbidity and healing time of injuries when compared with previously performed dressing treatments. The subatmospheric pressure therapy is a useful method in treating acute traumatic wounds, acting as a bridge between the emergency treatment and the final coverage of the skin lesions, being better when compared with more traditional methods of plastic surgery. |
| Negative pressure wound therapy management of the "open abdomen" following trauma: a prospective study and systematic review8 | Navsaria et al., 2013 | Systematic review | Assess the Effectiveness of Negative-Pressure Wound Therapy in the Closure of Secondary Peritoneostomies Due to Abdominal Trauma | The technique is safe, effective, and provides a high rate of aponeurosis closure with low complication rates in patients with severe abdominal trauma. |
| Terapia Por Pressão Negativa(TPN) versus Terapia Convencional em Ferimentos Complexos ("Negative Pressure Therapy [NPT] versus Conventional Therapy in Complex Wounds")12 | Albuquerque RS, 2017 | Systematic review | Compare cost, effectiveness, and incidence of adverse events between NPWT and conventional therapy. | The studies demonstrate an overall improvement in parameters: Average Hospitalization Time, Time to Complete Wound Closure, Infection Incidence, Granulation Tissue Formation, Average Dressing Change Frequency, as well as Overall Morbidity Reduction. However, the analysis of the studied parameters lacks quantitative data. |
| Single-use negative-pressure wound therapy versus conventional dressings for closed surgical incisions: systematic literature review and metaanalysis14 | Saunders et al., 2021 | Meta-Analysis | Determine whether the prophylactic use of the PICO™NPWT system could reduce the incidence of complications at the surgical site compared with conventional dressings. | The results suggest that sNPWT reduced surgicalsite complications such as: the odds of wound dehiscence (OR 0.70, 0.53 to 0.92; NNT 26), seroma(OR 0.23, 0.11 to 0.45; NNT 13) and necrosis (OR 0.11, 0.03 to 0.39; NNT 12). Mean length of hospital stay was shorter in patients who underwent sNPWT (MD-1.75, 95 per cent c. i.-2.69 to -0.81). |
| An economic evaluation of the use of TNP on full-thickness wounds17 | Mouës et al., 2005 | Descriptive study | Compared the costs of vacuum dressing versus conventional gauze dressing in the treatment of wounds requiring subsequent surgical closure. | The vacuum dressing treatment initially incurred higher costs compared with the conventional gauze dressing. However, this initial expenditure was offset by the reduced number of dressing changes and faster wound preparation for surgical treatment, resulting in an equivalent final cost for both treatments. |
| Tools to compare the cost of NPWT with advanced wound care: an aid to clinical decisionmaking18 | Searle and Milne, 2010 | Descriptive study | Comparative economic analysis of wound treatment using vacuum dressing versus conventional dressings. It delineates and calculates the unit and total costs of each material used for wound coverage, and ultimately compares the final costs for conducting weekly dressings using both methods. | The study suggests that despite the higher initial cost of vacuum dressing, it proved to be more financially effective, as it led to reduced hospitalization time, fewer dressing changes, decreased complications, and fewer surgical interventions. However, it recommends further studies to assess the cost-effectiveness ratio. |
| The clinical efficacy and cost effectiveness of the vacuum- assisted closure technique in the management of acute and chronic wounds: a randomized controlled trial19 | Braakenbur et al., 2006 | Descriptive study | Comparative analysis of vacuum dressing versus current dressings regarding wound treatment, tissue granulation, bacterial clearance, pain, treatment duration, and overall costs across various types of wounds. | The vacuum dressing resulted in faster healing compared with conventional treatment, particularly in diabetic and cardiovascular patients. The overall cost was similar in both treatments, but the vacuum dressing had the advantage of providing greater comfort to both the patient and the healthcare team responsible for dressing changes. |
| Bronquial fistula closure with negative-pressure wound therapy: a feasible and cost-effective treatment13 | Nunes et al., 2016 | Descriptive study | demonstrate the application of NPT as a resource for Bronquial Fistula treatment and comparatively analyze the overall cost of treatment. | The NPT is a viable and cost-effective option for the closure of bronchial fistula after pulmonary lobectomy. |

Discussion
The application of vacuum-assisted wound dressing, or negative-pressure therapy, originated in the 1990s with the primary objective of expediting the healing time of complex wounds in patients and, consequently, reducing the duration of their hospitalization. Commercially introduced in 1997, it was adopted as an adjunctive treatment for wounds, aimed at achieving a reduction in both healthcare and financial expenditures.9
Vacuum-assisted therapy or Negative-Pressure Wound Therapy (NPWT) stands out as one of the most efficient methods for treating complex wounds, expediting the healing process through continuous suction of the secretion generated by the inflammatory response triggered by the injury. This approach can be indicated for the treatment of acute, chronic, traumatic wounds, wound dehiscence, pressure ulcers, diabetic ulcers, flaps, grafts, and selected cases of burns.7
Negative-pressure wound therapy enables wound healing in a moist environment through the application of localized and monitored sub-atmospheric pressure to a material used as an interface (foam or gauze) placed over the entire wound bed, with the aim of continuously removing the present exudate. A suction tube is secured and connected to a reservoir that collects the extracted material, and the entire process is monitored via a preprogrammed computer system.9
Contraindications for its use include wounds suspected of malignancy, fistulas to organs and cavities, untreated osteomyelitis, non-enteric or non-explanted fistulas, expose of vessels, nerves, organs or sites of anastomoses.9,10
According to Navsaria et al., vacuum therapy promotes the healing process by accelerating tissue repair, reducing bacterial colonization, diminishing pain, edema, treatment time, and hospitalization duration, ultimately leading to cost savings in comparison to existing conventional dressings.8
Demonstrating its effectiveness, Milcheski et al. published an article in 2013 describing the use of negative pressure therapy in 178 patients with traumatic wounds. It was concluded that negative pressure wound therapy is a useful method in the treatment of acute traumatic wounds, acting as a bridge between emergency treatment and final skin coverage of these injuries. Compared with more traditional methods of plastic surgery, it has shown satisfactory results, significantly reducing morbidity and the healing time of these injuries.11
When compared with conventional treatment for exuding wounds, NPWTyields a reduction in treatment time of up to 74%, an improvement in lesion extent in 77%, and contributes to exudate control in 96% of patients.12
Comparing cost-effectiveness, Nunes et al. demonstrated that the cost of treating the bronchial fistula after the introduction of NPWT was 6.5 times lower than the cost of conventional treatments previously undertaken. The current study reaffirms the cost-benefit advantage of NPWT, which stems from shorter hospitalization periods and a lower prevalence of complications compared with conventional treatment methods.13
When it comes to patients with high risk of surgical-site complication (SSCs), Sanders et al., in 2021, concluded that the use of a NPWT device reduced the mean length of hospital stay and the incidence of SSCs.14
Despite its significant efficacy, this therapy7 comes with high costs, and its unavailability within SUS limits the number of patients who can access this treatment in Brazil. Over the years, various commercial devices—RENASYS, Smith + Nephew, London, United Kingdom; SIMEX Medizintechnik GmbH, Deisslingen-Lauffen, Germany; VivanoTec, Hartmann, Amtsgericht Ulm, Germany) —have been introduced to the Brazilian market, but this has not led to a reduction in treatment costs, maintaining the limited access for a large portion of patients with complex wounds to this type of treatment (►Table 2).
| MANUFACTURER | MODEL | Cost in United States dollars |
|---|---|---|
| Smith & Nephew (London, United Kingdom) | TPN PICO portable softport | 595.45 |
| Convatec (London, United Kingdom) | Avelle ultraportable | 388.25 |

In 2014, the National Committee for the Incorporation of Technologies in the SUS (Comissão Nacional de Incorporação de Tecnologias, CONITEC, in Portuguese), through ordinance nr. 34, dated September 26, 2014, publicly announced its decision not to incorporate VAC for extensive acute traumatic wounds within the scope of SUS. This decision was based on uncertainty regarding the treatment's effectiveness and its significant budget impact.15 The search was conducted in the primary databases MEDLINE and LILACS, resulting in 8 systematic reviews, 14 clinical trials, and 1 case-control study. After analysis, only two studies met the inclusion criteria. One study demonstrated efficacy with reduced wound closure time using a "homemade" device, reporting to the commission that there is no evidence that commercial devices produce better outcomes. This review contradicts several scientific articles published worldwide, and it lacks a thorough analysis of total costs (dressings, hospitalization, and nursing time) for both conventional and vacuum-assisted dressings for the duration of the treatment of patients with complex wounds.15,16
In 2021, the National Supplementary Health Agency (Agência Nacional de Saúde Suplementar – ANS, in Portuguese) approved NPWT for the treatment of diabetic foot ulcers, which holds significant relevance as a substantial number of diabetic patients with complex wounds could benefit from this treatment.16
Studies comparing, economically, the advantages of VAT to other methods for treating complex wounds are scarce in the literature. However, some authors have attempted to compare the cost of conventional treatment with those of VAT, as seen in the study by Mouës et al., who evaluated the average costs of expenses for 54 patients admitted to the Plastic and Reconstructive Surgery Department. They compared material costs for NPWT and conventional therapy, in addition to nursing expenses. The authors concluded that material expenses were higher with VAT; however, nursing and hospitalization costs were lower due to a shorter period for patients to become eligible for surgical therapy. They did not observe cost differences between the two treatments.17 In light of these results, the patient's wellbeing should be a primary consideration.
Searle and Mirle18 developed simple tools (computer spreadsheets) to compare the weekly cost of treatment with periodic conventional dressings versus vacuum-assisted dressings. This approach yielded direct, easy-to-use, and replicable information. The authors calculated the costs of resources used in conventional dressings (materials, nursing time, and material rental) needed per week of treatment.
They multiplied this by the appropriate unit cost of each material and compared it to the costs of resources used in VAT, considering the frequency of dressing and reservoir changes, pump costs, and the number of weekly visits needed to change dressings. Following this analysis, the authors calculated the total weekly cost of both treatments (including material and nursing costs). This revealed that the cost of VAT (including material and nursing) is lower than that of conventional dressings, even if the unit price of VAT is higher.
Brakenburg et al.19 evaluated 65 patients, with 32 undergoing VAT and 33 receiving modern dressings. Comparing these groups across various types of complex wounds (ranging from acute trauma wounds to chronic wounds such as pressure ulcers and diabetic wounds) with similar characteristics, the authors noted that patients with cardiovascular disease and/or diabetes benefited most from VAT.
Despite their severe wounds, the healing time was shorter due to the mechanical stress applied and stimulation of neoangiogenesis. This study did not reveal significantly higher overall costs, despite the higher costs of VAT materials. The benefit lies in the reduced nursing time compared with conventional dressing treatments that require multiple changes throughout the day. No significant difference was found in the calculated total costs for both treatments. However, the time spent by nurses was significantly higher for conventional treatment, aligning with the result obtained by Searle and Mirle.18
In light of the above, a protocol (►Fig. 2) was developed for the indication of NPWT to a specific group of selected patients, aiming to assist in making decisions regarding the treatment of complex wounds.
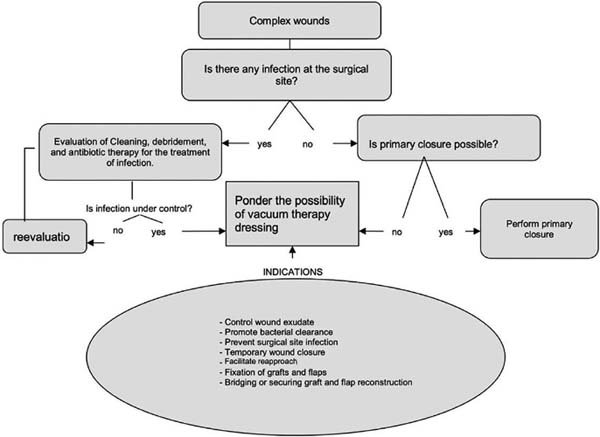

This protocol describes treatment options for patients with complex wounds, advocating the use of NPWT for patients who do not have an active site of infection and do not have the possibility of primary closure. Negative pressure wound therapy acts through the induction of deformation that enables the contraction of the borders and the stimulation of cell division, also promoting angiogenesis and formation of granulation tissue. Furthermore, it enhances continuous debridement in an isolated environment controlling wound exudate, promoting bacterial clearance, preventing surgical site infection, providing temporary wound closure, that facilitates bridging or securing graft and flap reconstruction.
Conclusion
The treatment of complex wounds, which demands increased medical and nursing care, extended hospitalization periods leading to higher hospital costs, and significant patient suffering, should be reconsidered. Vacuum therapy should be regarded as an option, given that in many cases its cost would be comparable to conventional methods, with its benefits outweighing the drawbacks.
For this reason, administrators of the Brazilian public healthcare system, along with stakeholders responsible for health guidelines, should reevaluate how to expand the implementation and utilization of NPWT within SUS to ensure it is widely available and used across the country. This would allow more individuals to access this potent tool, which contributes to faster wound recovery, reduces complications and secondary morbidities, and promotes quicker patient return to normal activities.
As such, a protocol is suggested for the indication of NPWT within a specific group of selected patients, facilitating decision-making for specialized healthcare professionals treating complex wounds and health administrators.
References
1. Irion GL. Feridas: novas abordagens, manejo clínico e atlas em cores. Rio de Janeiro: Guanabara Koogan; 2005
2. Smith GL, Bunker CB, Dinneen MD. Fournier's gangrene. Br J Urol 1998;81(03):347-355
3. Borges. EL. Feridas: Úlceras dos Membros Inferiores. Rio de Janeiro: Guanabara Koogan; 2011
4. Jorge AS. Dantas SRPE. Abordagem multiprofissional dot ratamento de feridas. São Paulo: Atheneu; 2003
5. Nightingale F. Notas sobre enfermagem: o que é e o que não é. Tradução de Amã lia Correa de Carvalho. São Paulo: Cortez; 1989
6. Jimenez CEJ. Terapia de presión negativa: una nueva modalidad terapêutica en e 1 manejo de heridas complejas, experiencia clínica con 87 casos y revisión de la lit eratura. Rev Colomb Cir 2007;22(04):209-224
7. Dos Santos TL, Borges da Silva Ado N, Viana de Sousa MB, et al. Terapia por pressão negativa no tratamento de feridas. Revista Eletrônica Acervo Saúde, n. 31, p. el231, 7 out. 2019
8. Navsaria P, Nicol A, Hudson D, Cockwill J, Smith J. Negative pressure wound therapy management of the "open abdomen" following trauma: a prospective study and systematic review. World J Emerg Surg 2013;8(01):4
9. Lima RVKS, et al. Terapia por pressão negativa no tratamento de feridas complexas. Rev Col Bras Cir 2017;44(01):81-93
10. Smith-nephew. [internet] [acesso em 11 de jan. 2022]. Disponível em: https://www.smith-nephew.com/canada/microsite/negative-pressure-woundtherapy/products/negative-pressure-wound-therapy-dressing-kits/
11. Milcheski DA, Ferreira MC, Nakamoto HA, Pereira DD, Batista BN, Tuma P Jr. Uso da terapia por pressão subatmosférica em feridas traumáticas agudas. Rev Col Bras Cir 2013;40(05):392-397. Doi: 10.1590/S0100-69912013000500008
12. Albuquerque RS. Terapia Por Pressão Negativa (TPN) vs.Terapia Convencional em Ferimentos Complexos-Revisão Sistemática. [Monografia]. Salvador: Universidade Federal Da Bahia; 2017
13. Nunes RB, Müller BF, Cipriano FE, Coltro PS, Farina JA. Bronchial fistula closure with negative pressure wound therapy: a feasible and cost-effective treatment. Rev Col Bras Cir 2016;43(04): 292-294. Doi: 10.1590/0100-69912016004007
14. Saunders C, Nherera LM, Horner A, Trueman P. Single-use negative-pressure wound therapy versus conventional dressings for closed surgical incisions: systematic literature review and meta-analysis. BJS Open 2021;5(01):zraa003. Doi: 10.1093/bjsopen/zraa003
15. Brasil. Ministério da Saúde. Gabinete do Secretário, [internet] Portaria no 34 de 15 de setembro de 2014. Brasília 2014. [acesso em 27 dec 2021]. Disponívelem: http://conitec.gov.br/images/Artigos_Publicacoes/VAC_FINAL.pdf
16. Brasil. Resolução nº 465, de 24 de fevereiro de 2021. Atualiza o Rol de Procedimentos e Eventos em Saúde que estabelece a cobertura assistencial obrigatória a ser garantida nos planos privados de assistência à saúde. Diário Oficial da União [Internet], 24 Fev 2021 [acesso em 07Jul2021]. Disponívelem: https://www.in.gov.br/web/dou/-/resolucao-normativa-rn-n-465-de-24-de-fevereirode-2021-306209339
17. Mouës CM, Van Den Bernd GJCM, Meerding WJ, Hovious SER. An economic evaluation of the use of TNP on full-Thickness Wounds. J Wound Care 2005;14(05):225-227
18. Searle R, Milne J. Tools to compare the cost of NPWT with advanced wound care: na aid to clinical decision-making. Wounds 2010;6(01): 106-109
19. Braakenburg A, Obdeijn MC, Feitz R, van Rooij IA, van Griethuysen AJ, Klinkenbijl JH. The clinical efficacy and cost effectiveness of the vacuum-assisted closure technique in the management of acute and chronic wounds: a randomized controlled trial. Plast Reconstr Surg 2006;118(02):390-397, discussion 398-400
1. Faculdade de Medicina de Jundiaí, Hospital São
Vicente de Paulo, Jundiaí, SP, Brazil
Address for correspondence Felipe Andrade Lopes, Faculdade de Medicina de Jundiaí, Hospital São Vicente de Paulo, Jundiaí, Jundiaí, SP, Brazil (e-mail: felipe.fmj44@gmail.com; gibanovv@gmail.com).
Article received: September 9, 2023.
Article accepted: September 29, 2024.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket