



Original Article - Year 2024 - Volume 39 -
Relationship between Muscle Strength Pattern, Classification of Facial Wrinkles, and Dose of Botulinum Toxin Serotype A
Relação entre o padrão de força muscular, a classificação de rugas faciais e a dose de toxina botulínica sorotipo A
João Vitor Moraes Pithon-Napoli1 ; Gabriela Ducioni Matos1; Rubia Carniato Casagrande1; Mariana Pedrazzi Moretti1
; Gabriela Ducioni Matos1; Rubia Carniato Casagrande1; Mariana Pedrazzi Moretti1
ABSTRACT
Introduction The primary action of botulinum toxin type A (BoNT-A) is to inhibit acetylcholine release from the presynaptic terminal, resulting in reversible chemical muscle paralysis. It is a widely accepted treatment for improving the appearance of glabellar expression lines resulting from muscle contraction.
Materials and Methods We evaluated the glabellar force patterns, facial wrinkle classification, and the number of BoNT-A units used in the corrugator and procerus muscles.
Results Themean total BoNT-A units used were 7.2 IU in the corrugator muscle (7.1 IU in women and 7.4 IU in men) and 3.9 IU in the procerus muscle (3.9 IU in women and 4.1 IU in men), with a positive correlation between the number of units and the age of the 58 participants. Regardingmuscle strength pattern,more units were needed in the corrugator muscle with a strong or moderate pattern and facial wrinkle classification ranging from 3 to 4 (8 IU and 8.5 IU, respectively). The procerus muscle required more units in subjects with strong force patterns and wrinkles classified as 3 to 4 (5 IU). Wrinkles with a 3-to-5 classification required the highest number of BoNT-A units.
Conclusion The number of BoNT-A units used is directly proportional to the strength pattern and classification of facial wrinkles, with more units required for strong force patterns and deep wrinkle classifications.
Keywords: botulinum toxins, type A; dermatology; facial muscles; rosacea; skin aging
RESUMO
Introdução A toxina botulínica A (BoNT-A) atua inibindo a liberação de acetilcolina do terminal présináptico, resultando em paralisia química reversível dos músculos. É um tratamento amplamente aceito para melhorar a aparência das linhas de expressão glabelares que se desenvolvem devido à contração muscular.
Materiais e Métodos Foram avaliados os padrões de forças glabelares; classificação de rugas faciais; e quantidade de unidades de BoNT-A utilizadas nos músculos corrugador e prócero.
Resultados A média total de unidades de BoNT-A utilizadas foi de 7,2 UI no músculo corrugador (mulheres 7,1 UI e homens 7,4 UI) e de 3,9 U no prócero (mulheres 3,9 UI e homens 4,1 UI), com correlação positiva entre o número de unidades utilizadas e a idade dos 58 participantes. Quanto ao padrão de forças, utilizou-se mais unidades no músculo corrugador com padrão forte e classificação de rugas faciais de 3 a 4, e moderado com a mesma classificação de rugas faciais (8 UI e 8,5 UI, respectivamente), no músculo prócero foram utilizadas mais unidades no padrão de força forte comrugas classificadas em 3 a 4 (5 UI). Sendo as rugas classificadas de 3 a 5 as que mais necessitaram de unidades de BoNT-A.
Conclusão A quantidade de unidades de BoNT-A utilizadas é diretamente proporcional ao padrão de força e classificação das rugas faciais, sendo necessária a utilização de mais unidades quando observado o padrão de força forte e classificação de rugas profundas.
Palavras-chave: dermatologia; envelhecimento da pele; músculos faciais; rosácea; toxinas botulínicas tipo A
Introduction
German physician Justinus Kerner wrote the first report in history of botulinum toxin (BoNT) in the 18th century following his discovery of botulism from observing deaths in Germany after ingesting contaminated blood sausages, a traditional preserved food from the region.1,2 In 1897, Van Ermengem, using histological sections, isolated and described Clostridium botulinum, the anaerobic bacterium causing botulism. From then on, investigations attempted to understand the relationship between the disease and the toxin and to describe the toxin’s structure and mechanism of action.3,4
Botulinum toxin has a light chain (50 kDa) and a heavy chain (100kDa) joined by disulfide bonds and surrounded by hemagglutinins.5,6 It causes muscle paralysis when the hemagglutinin contacts the terminal axon, causing the heavy chain to connect with the axonal receptor to facilitate the passage and entry of the molecule into the nerve cell. Next, the chains disconnect, and the light chain cleaves the soluble N-ethylmaleimide sensitive factor attachment protein receptor (SNARE) complex to remove part of its structure, soluble N-ethylmaleimide sensitive factor attachment protein-25 (SNAP-25). Therefore, the SNARE complex, which would be responsible for acetylcholine entry into the synaptic cleft, cannot function, preventing cell membrane depolarization, calcium influx, and sodium efflux, stopping muscle contraction of actin and myosin fibers.5,6,7
Ophthalmologist Alan B. Scott, from the Eye Research Institute, in San Francisco, California (1920), described the medicinal use of BoNT in patients with ocular misalignment resulting from strabismus.3,4 Botulinum toxin injection reduced the muscle activity through chemical denervation.8 Since then, other indications have included treating dynamic wrinkles, axillary hyperhidrosis, and blepharospasm.9,10 The Food and Drug Administration (FDA) only approved BoNT in 1989, to treat muscle disorders, and, in 2002, for aesthetic purposes.5,7
Glabellar region expression lines result from the synergistic contraction of the corrugator muscle, depressor muscle of the superciliary muscle, procerus muscle, or both, leading to “frontal furrows,” particularly between the eyebrows, evidencing aging. The constant contraction of the glabellar muscle complex forms dynamic wrinkles which evolve into static wrinkles, more pronounced and noticeable at rest. Their presence can often be perceived as a sign of aging and mistakenly give the impression of emotions such as anger or sadness.11
Botulinum toxin type A (BoNT-A) is a widely accepted treatment for improving the appearance of glabellar lines.12 In addition, it generates great patient satisfaction since the aesthetics of glabellar lines impact psychological wellbeing, self-confidence, and quality of life.13,14 However, BoNT-A has some contraindications, such as keloids, neuromuscular diseases, body dysmorphic disorders, and allergies to some of its components.14,15
Objective
The current study aimed to establish the relationship between muscle strength, facial wrinkle classification, and the number of BoNT-A units to obtain satisfactory outcomes in treating glabellar expression lines.
Materials and Methods
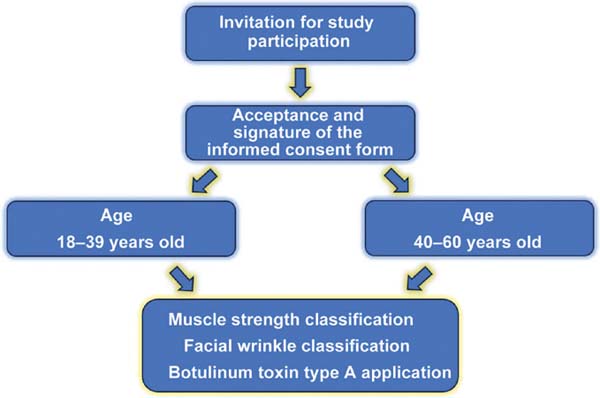
The Research Ethics Committee of the Institute for the Health and Wellbeing of Women (Instituto de Saúde e Bem-estar da Mulher – ISBEM, in Portuguese) (CEP 6.849.192) approved the protocol, materials, and all the procedures of the present study. We randomly invited 58 patients to participate in the study, which occurred at Clínica de Estética Pithon Napoli, in São Paulo, SP, Brazil, from December 2023 to April 2024. All patients received information about the procedures and guidance regarding this study from the team’s physicians, who also answered any questions from the subjects. Next, participants signed an informed consent form. We excluded all patients who did not agree to participate in the study, refused to sign the informed consent form, received tetanus shots or any chemical peel in the 6 months prior to the invitation, had undergone procedures potentially affecting the forehead and glabellar regions within 12 months, with autoimmune diseases or under current use of medications acting on neuromuscular junctions. The study included male and female patients who sought the clinic to undergo a glabellar line-filling procedure using BoNT-A. The participants were divided into 2 groups according to their age range: from 20 to 39 (36 participants) and from 40 to 60 years old (21 participants). We assessed the following parameters: glabellar force pattern, facial wrinkle classification, and number of BoNT-A units used in the corrugator and procerus muscles (study design – ►Fig. 1).

Muscle strength classification
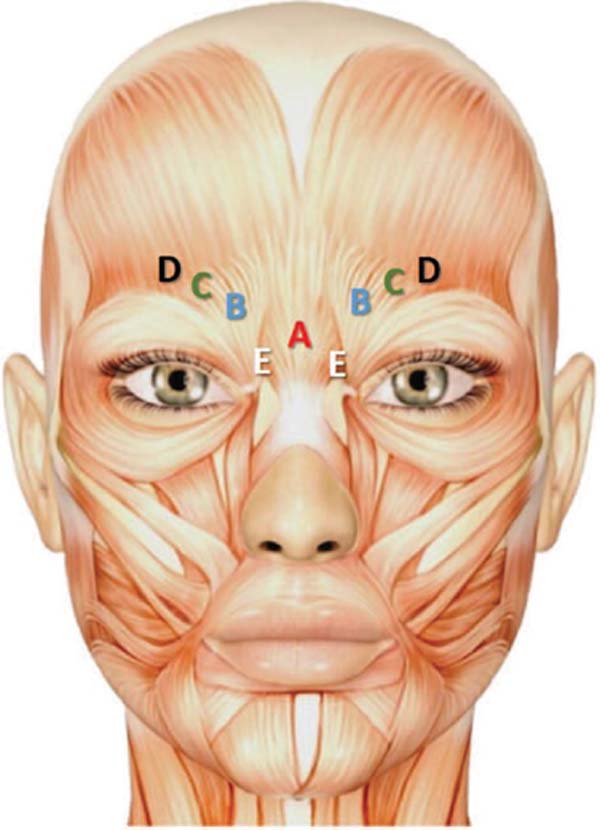
For muscle strength classification (corrugator and procerus muscles), the authors asked the participant to make an “angry face” (►Fig. 2), which was classified into three strength levels: strong pattern, in which the corrugator and procerus muscles were well defined and presented a medial formation of very evident dermal fractures; moderate pattern, in which the muscles were well defined, with less central force and, as a result, with less evident dermal fractures; and weak pattern, in which the limits of the glabellar muscles, mainly the corrugators, were not observed, with less formation of intense dermal fractures and expression lines.


Facial wrinkle classification
Wrinkle determination occurred according to Lemperle,11 using a six-point photonumeric classification scale in which the wrinkle degree in the reference photographs was compared with the wrinkles on the participant’s face. All participants were photographed (iPhone 12 Pro [Apple Inc., Cupertino, CA, USA] and QuantifiCare camera [QUANTIFICARE S.A., Biot, France]) for photographic documentation and evaluation. ►Table 1 shows the Lemperle classification.
| Score | Description |
|---|---|
| 0 | No wrinkles |
| 1 | Perceptible wrinkles |
| 2 | Shallow wrinkles |
| 3 | Moderately deep wrinkles |
| 4 | Deep wrinkles |
| 5 | Very deep wrinkles |

BoNT-A application
The procedure used 50 or 30 intertnational units (IU) of BoNT-A - Botulift (Bergamo Farmacêutica - Medytox Inc, Cheongwongu, South Korea), applied intramuscularly with a BD pediatric syringe (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) in the glabellar line region. ►Table 2 shows the maximum number of BoNT-A units for safe application in each muscle. ►Fig. 3 is the visual representation of each muscle. The number of units applied followed the assessment of the strength classification and facial wrinkles. Botulift application occurred on day 0, with reassessment 15 to 30 days post-application. The procedure did not require anesthesia. The physician instructed the participant to use analgesic medication, either dipyrone, 1g, or paracetamol, 725 mg, every 6 hours, in case of pain. We did not recommend antiinflammatories or corticosteroids for discomfort/pain in the application region. The effect of Botulift begins approximately 48 to 72hours after application, and its maximum effect occurs around 1 to 4 weeks after application. The application effect (muscle relaxation and reduction of excessive contraction) often lasts 3 to 4 months.
| Glabellar lines | Angle, needle plane, and Botulift units |
|---|---|
| Corrugator head | Application at 90°, deep plane, 1–5 units |
| Corrugator body | Application at 45°, medium plane, 0–5 units |
| Corrugator tail | Application at 45°, medium plane, 0–5 units |
| Procerus | Application at 90°, deep plane, 1–5 units |
| Depressor supercilii | Application at 90° towards the medial glabellar region (supraperiosteal), deep plane, 1–3 units |


Data analysis
Categorical variables were expressed as absolute counts and proportions, and these were compared using the Chi-squared (Χ2) test. Continuous variables were presented as medians and interquartile ranges, and group comparison used the Mann-Whitney test. Pearson’s correlation investigated the relationships between the frontalis (corrugator and procerus) muscles and the administered BoNT-A doses. The analyses were performed with the IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA) statistical software. Values were considered statistically significant when p ≤ 0.05 and were expressed as mean ± standard deviation (SD).
Results
On average, the age at first injection was 35 years for both men and women. Twenty-eight percent of the participants were male and 72% were female, with an average age of 38. In men, the average age was 36 (27-54), and approximately 80% of patients were under 40. In women, the average age was 38 (23-68), and 70% were under 40.
The average number of BoNT-A units used was 7.2 in the corrugator and 3.9 in the procerus muscles. When separated by gender, the average number applied in the corrugator was 7.1 for females and 7.4 for males. In the procerus, the average number was 3.9 for females and 4.1 for males. Linear regressions revealed a positive association between the number of units and the age of the patients both in the corrugator (r2 = 0.30; p < 0.05; ►Fig. 4A) and in the procerus (r2 = 0.30; p < 0.05; ►Fig. 4B) muscles. This suggests that the higher the degree of facial wrinkle classification, the more units are required for greater paralysis and, consequently, better outcomes.
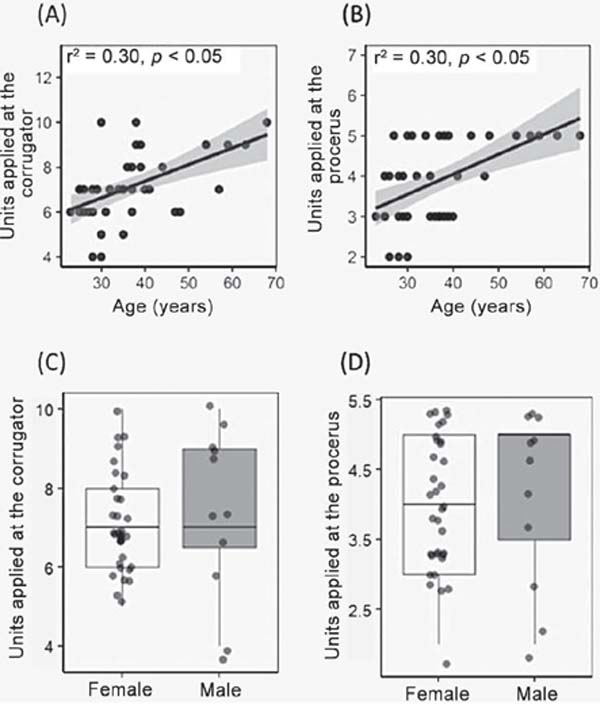

When analyzing the number of BoNT-A units applied regarding gender, there was no difference between men and women in the corrugator (p = 0.42; ►Fig. 4C) or procerus muscle (p = 0.51; ►Fig. 4D).
Weak corrugator strength, with facial wrinkle classification ranging from 1 to 2, required, on average, 6IU. An average of 3.5 IU was applied in the head, 0.5IU in the body, and 2IU in the tail of the corrugator. Moderate corrugator strength, with facial wrinkle classification ranging from 0 to 2, required an average of 7IU, including 3.75 IU in the head, 0.9IU in the body, and 2.3IU in the tail of the corrugator. Moderate strength patterns with facial wrinkle classification ranging from 3 to 4 required an average of 8 IU, with 4.7 IU applied in the head, 1 IU in the body, and 2.33 IU in the tail of the corrugator. Strong corrugator strength pattern with facial wrinkle classification ranging from 1 to 2, required an average of 7.2IU, with 4IU applied in the head, 1.1 IU in the body, and 2.1 IU in the tail of the corrugator. The same strong strength pattern with facial wrinkle classification ranging from 3 to 4 required an average of 8.5IU, with 4.5 IU applied in the head, 0.75IU in the body, and 3.25 IU in the tail of the corrugator. Weak procerus strength pattern with facial wrinkle classification ranging from 0 to2 required an average of 3.37IU. The same pattern with a facial wrinkle classification of 3 required 4IU. Moderate strength patterns with facial wrinkle classification ranging from 0 to 2 required, on average, 3.5IU. A moderate pattern with facial wrinkle classification ranging from 3 to 4 required the application of, on average, 4.25 IU. Strong procerus strength pattern with facial wrinkle classification ranging from 1 to 2 required an average of 4.9IU and with facial wrinkle classification ranging from 3 to 5, 5IU.
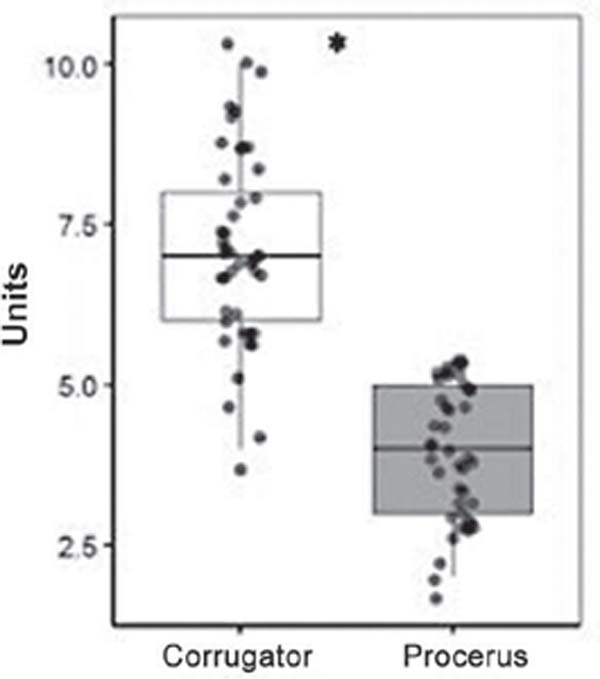
When comparing the number of BoNT-A units required in the corrugator and procerus muscles, we found a significant difference, with more units required in the corrugator than in the procerus (p < 0.01; ►Fig. 5).

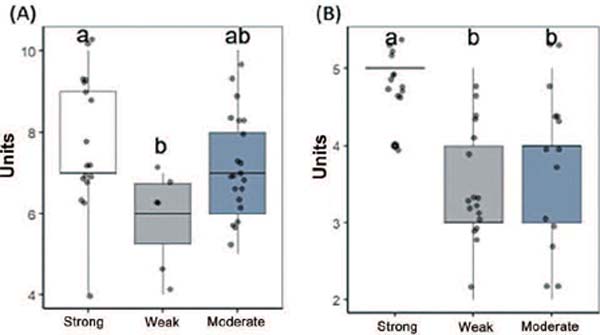
In the corrugator, there was a significant difference in the number of units per different strength patterns (F2,42 = 4.11; p = 0.02). The Tukey test revealed a significant difference between the “strong” and “weak” groups, with more units required in the “strong” group (p < 0.05; ►Fig. 6A). In addition, there were significant differences in the procerus when the groups were compared together (χ2 = 20.04; degree of freedom [df] = 2; p < 0.05; ►Fig. 6B). Separately, the “strong” group differed both from the “weak” and the “moderate” strength pattern (p < 0.05).

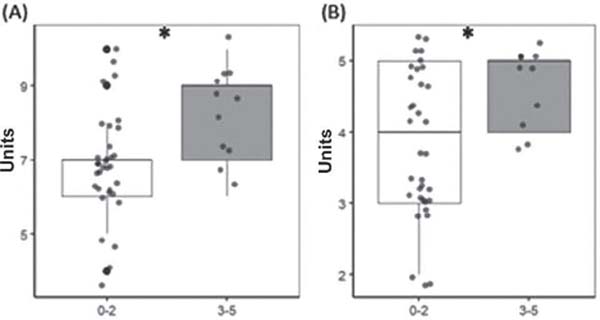
We observed a significant difference between groups with facial wrinkle scores from 0 to 2 and 3 to 5 regarding the number of BoNT-A units used in the 2 muscles. In both muscles, the group with facial wrinkle scores from 3 to 5 required more BoNT-A units when compared with the group with facial wrinkle scores from 0 to 2 (corrugator: t = –2.72; df = 42; p < 0.05; ►Fig. 7A; procerus: p < 0.05; ►Fig. 7B).

Discussion
Age at the first BoNT-A application was 35 years old both in men and women. Women sought the procedure twice as often as men but usually required fewer BoNT-A units than men. The number of units used in the corrugator muscle was higher than in the procerus muscle. The amounts in both muscles increased proportionally to the age of the participants. A “strong pattern” of corrugator and procerus strength was the most common, requiring more BoNT-A units. The facial wrinkle classification requiring most BoNT-A units in the corrugator and procerus muscles ranged from 3 to 5.
The glabella is the first area noted in facial expression. Its contraction is associated with negative emotions, such as impatience, anger, and fatigue, which the subject often expresses unawarely.16 The main muscles forming the glabellar complex include the corrugator and orbicularis oculi (eyebrows approximation and depression), the procerus and depressor muscles (eyebrow depression), and the inferior fibers of the frontalis muscle (eyebrow elevation). Muscle activity causes hyperkinetic lines perpendicular to the muscle contraction direction, forming unwanted horizontal, vertical, and oblique wrinkles.17
Some studies report that glabellar lines act similarly in most subjects, with some differences regarding gender18,19,20 (since men present heavier muscles and thicker skin), age, ethnicity,21,22 sun exposure, and physical activity-related differences.23,24 In our study, we observed a greater demand for the procedure among women, with a wide age range, from the young to those over 60. Younger participants are encouraged to use BoNT-A preventively, while older participants use it to correct and maintain features acquired over time. Due to the period of muscle paralysis and relaxation, the skin (epidermis and dermis) regenerates, giving it a better appearance than before the application, leading to progressive muscle reduction and re-education, improving skin texture in the long term.
Botulinum toxin type A is administered in IU. The estimated median lethal dose ranges from 2,500 to 3,000 IU for a 70-kg adult. Although the exact dose of the BoNT-A known to cause toxicity is unknown, it is often accepted that single BoNT-A doses should not exceed 500 IU.25 The number of points and units varies according to each patient’s requirements. For longer duration and higher patient satisfaction with the outcomes of upper face treatment, the suggested ideal standard plan for BoNT application uses a total of 64 IU, combining the standard glabella treatment in a “U” shape (ranging from 12-40 IU), frontal muscle treatment - total pattern (ranging from 8-25 IU), and periorbital lines (ranging from 6-15 IU on each side). Although this standard dosage remains commonly used and can serve as a guide for new professionals, many clinicians have begun to tailor injection sites and dosages to each patient. The selection of dose and injection patterns must consider muscle strength, anatomy (rhytids pattern), basal asymmetries, and the patient’s desires.26
Some studies suggest the treatment of glabellar frown lines with multiple injections of BoNT-A in high doses of low volumes, allowing its precise placement with little spread to non-target areas. Two double-blind, multicenter, controlled studies used 4IU of BoNT-A at 5 injection sites: one in the procerus and 2 in each corrugator, bilaterally. These injections had good outcomes in most patients, with rare transient adverse effects.27,28,29 Our study, consistent with the literature, demonstrates that the muscle requiring more units is the corrugator. Our methodology showed that these quantities depend on the strength and facial wrinkle classification. Patients with greater strength had larger and deeper frontal lines in response to regional muscle movement. Therefore, it is necessary to address the regions with the largest number of units and distribution points for total or partial paralysis to obtain a natural effect in the target region. Our team suggests a wet BoNT-A dilution, that is, diluting 200IU in 4mL of saline solution, allowing its distribution in more points and, as a result, better influencing the force vectors at the orbital forehead.
Recent publications report individualized treatments. De Sanctis Pecora et al.30 performed a blind study to evaluate 130 women with moderate or severe glabellar wrinkles, using the standard therapy with 5 injection points (4IU per point) and the One21 technique with an individualized and customized approach regarding point distribution and dosage. They observed that incobotulinumtoxin A effectively reduced dynamic glabellar lines in all participants. Notably, individualized assessment and treatment with the One21 technique improved the performance, achieving significantly higher efficacy rates than the standard 5-point treatment in mild, moderate, and severe glabellar wrinkles, especially for asymmetrical glabellar lines or involvement of muscle groups other than the procerus and corrugator.30 In our individualized experience, we have observed that a larger number of distribution points and smaller amounts of BoNT-A per point can produce more natural results, sustaining movement but preventing line appearance without losing the time of action of BoNT-A in the regions. Our patients report satisfactory and long-lasting outcomes four months after this technique.
Knowledge of the target regional anatomy, followed by a precise injection technique with adequate dose and injection depth, is essential to improve outcomes and avoid complications.30 Botulinum toxin type A injection requires a proper understanding of the anatomical shape and attachment of the facial muscles to guide objective muscle identification, resulting in a more effective approach. Our team is constantly updated and dedicated to scientific studies to bring the most modern and effective techniques to improve our techniques and deliver the best outcomes to our patients.
Our findings reinforce the significance of an individualized assessment with efficient methodologies to achieve the best outcomes during BoNT-A injection for glabellar wrinkle treatment. A limitation of our study is the scarce use of technology. The market currently offers cameras with three-dimensional technology software allowing better image evaluation, potentially improving the assessment of the relationship and direction of the muscle force vectors before and after BoNT-A applications. In our next studies, image evaluation will be more objective.
Conclusion
The required number of BoNT-A units is directly proportional to the strength pattern and facial wrinkle classification; more BoNT-A units are necessary for strong strength patterns and deep wrinkles to ensure customer satisfaction with the methodology. Botulinum toxin type A is an excellent ally in treating wrinkles. In addition, it plays a significant role in preventing wrinkle evolution from shallow to deep and static and aging.
REFERENCES
1. Guerra Neto P. Toxina botulínica tipo A: ações farmacológicas e riscos do uso nos procedimentos estéticos faciais. Recife: Instituto Nacional de Ensino Superior e Pesquisa, Centro de Capacitação Educaional; 2016
2. Colhado OC, Boeing M, Ortega LB. Botulinum toxin in pain treatment. Rev Bras Anestesiol 2009;59(03):366–381
3. Costa FHR. A toxina botulínica: histórico, fisiopatologia e indicações. Rio de Janeiro2020
4. Dressler D, Roggenkaemper P. A brief history of neurological botulinum toxin therapy in Germany. J Neural Transm (Vienna) 2017;124(10):1217–1221
5. de Oliveira CCA, Fernandes EC, Medeiros KDO, Maia MCB, Seabra EJG, Santos PC. Toxina botulínica: contexto histórico, molecular e de aplicação prática na área da saúde. Revista Brasileira De Educação E Saúde 2020;10:1–10
6. Drinovac-Vlah V, Bach-Rojecky L. Botulinum toxin type A: Basic pharmacological profile and therapeutic application. Arh Farm (Belgr) 2020;70:10–19
7. Sposito MMdM. Toxina Botulínica doTipo A: mecanismo de ação. Acta Fisiatr 2009;16:25–37
8. Gouveia BN, Ferreira LdLP, Rocha Sobrinho HM. O uso da toxina botulínica em procedimentos estéticos. REVISTA BRASILEIRA MILITAR DE CIÊNCIAS 2020;6:56–66
9. Costa, Adilson,Talarico Filho S, Arruda LH, de Sanctis-Pecora, Carla, et al. Estudo clínico multicêntrico, prospectivo, comparativo, randomizado e duplo cego, entre duas formulações de toxina botulínica tipo A registradas no Brasil para otratamento das rugas da glabela. Surg Cosmet Dermatol 2016;8:33–40
10. Gimenez R. Pinto. Análise retrospectiva das alterações da dinâmica facial após aplicações seriadas de toxina botulínica tipo A. São Paulo: Universidade São Paulo; 2007
11. Lemperle G, Holmes RE, Cohen SR, Lemperle SM. A classification of facial wrinkles. Plast Reconstr Surg 2001;108(06):1735–1750, discussion 1751–1752
12. Kaufman-Janette J, Cox SE, Dayan S, Joseph J. Botulinum Toxin Type A for Glabellar Frown Lines: What Impact of Higher Doses on Outcomes? Toxins (Basel) 2021;13(07):494
13. Benedetto AV. The cosmetic uses of Botulinum toxin type A. Int J Dermatol 1999;38(09):641–655
14. Allergan-BOTOX. Bula paciente. 2023. Available from: https://www.allerganaesthetics.com.br/marcas/botox
15. Small R. Botulinum toxin injection for facial wrinkles. Am Fam Physician 2014;90(03):168–175
16. Lewis MB, Bowler PJ. Botulinum toxin cosmetic therapy correlates with a more positive mood. J Cosmet Dermatol 2009;8(01): 24–26
17. Borba A, Matayoshi S, Rodrigues M. Avoiding Complications on the Upper Face Treatment With Botulinum Toxin: A Practical Guide. Aesthetic Plast Surg 2022;46(01):385–394
18. Carruthers J, Fagien S, Matarasso SL, Group BCBotox Consensus Group. Consensus recommendations on the use of botulinum toxin type a in facial aesthetics. Plast Reconstr Surg 2004;114; (6, Suppl)1S–22S
19. Draelos ZD. The shrinking world: skin considerations in a global community. J Cosmet Dermatol 2006;5(01):1–2
20. Flynn TC. Botox in men. Dermatol Ther 2007;20(06):407–413
21. Porter JP, Lee JI. Facial analysis: maintaining ethnic balance. Facial Plast Surg Clin North Am 2002;10(04):343–349
22. Monheit G, Carruthers A, Brandt F, Rand R. A randomized, doubleblind, placebo-controlled study of botulinum toxin type A for the treatment of glabellar lines: determination of optimal dose. Dermatol Surg 2007;33(1 Spec No.):S51–S59
23. Rexbye H, Petersen I, Johansens M, Klitkou L, Jeune B, Christensen K. Influence of environmental factors on facial ageing. Age Ageing 2006;35(02):110–115
24. de Almeida AR, da Costa Marques ER, Banegas R, Kadunc BV. Glabellar contraction patterns: a tool tooptimize botulinum toxin treatment. Dermatol Surg 2012;38(09):1506–1515
25. Sorensen EP, Urman C. Cosmetic complications: rare and serious events following botulinum toxin and soft tissue filler administration. J Drugs Dermatol 2015;14(05):486–491
26. Borba A, Matayoshi S. Facial rejuvenation techniques: botulinum toxin and MD Codes TM. 1st ed. São Paulo - Brasil: Buzz Editor Ltda; 2018
27. Carruthers A, Carruthers J. Botulinum toxin type A: history and current cosmetic use in the upper face. Semin Cutan Med Surg 2001;20(02):71–84
28. Carruthers JD, Lowe NJ, Menter MA, Gibson J, Eadie N, Group BGLISBotox Glabellar Lines II StudyGroup. Double-blind, placebo-controlled studyof the safetyand efficacyof botulinum toxintype A for patients with glabellar lines. Plast Reconstr Surg 2003;112 (04):1089–1098
29. Carruthers JA, Lowe NJ, Menter MA, et al; BOTOX Glabellar Lines I Study Group. A multicenter, double-blind, randomized, placebo-controlled studyof the efficacy andsafetyof botulinum toxin type A in the treatment of glabellar lines. J Am Acad Dermatol 2002;46 (06):840–849
30. de Sanctis Pecora C, Pinheiro MVB, Ventura Ferreira K,Jacobino de Barros Nunes G, Miot HA. The One21 Technique: An Individualized Treatment for Glabellar Lines Based on Clinical and Anatomical Landmarks. Clin Cosmet Investig Dermatol 2021;14:97–105
1. Clínica de Estética Pithon Napoli, São Paulo,
SP, Brazil
Address for correspondence João Vitor Moraes Pithon-Napoli, Clínica de Estética Pithon Napoli, São Paulo, SP, Brazil (e-mail: joaovitorpithon@gmail.com; francinealmeida@alumni.usp.br).
Article received: June 07, 2024.
Article accepted: November 16, 2024.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket