



Articles - Year 2001 - Volume 16 -
Reconstruction of the Mandibular Condyle using a Costochondral Graft after Osteosynthesis in Fracture Dislocations
Reconstrução de Côndilo Mandibular com Enxerto Costocondral após Osteossíntese para Fratura com Deslocamento
ABSTRACT
The treatment of mandibular condylar fractures is a controversial issue among surgeons. Complete resorption of the condylar process after a fracture treated surgically using internal fixation has been described in the literature. The present study of a 14 year-old female patient aims to describe a case of resorption of the mandibular condyle due to a condylar fracture with displacement, which had been previously treated by surgical reduction and osteosynthesis with steel sutures. Treatment consisted of a costochondral graft fixed with two 2.0 mm diameter screws that provided adequate long-term functional and aesthetic results.
Keywords: Condylar fracture; condylar reconstruction; costochondral graft
RESUMO
O tratamento das fraturas do côndilo mandibular é alvo de muita divergência entre os cirurgiões. Há casos relatados na literatura de reabsorção completa do processo condilar após fratura tratada cirurgicamente com fixação interna.
O presente trabalho tem como objetivo relatar um caso clínico de reabsorção do côndilo mandibular decorrente de fratura condilar com deslocamento que havia sido tratada por redução cruenta e osteossíntese a fio de aço em uma paciente do sexo feminino de 14 anos de idade. Para a reconstrução foi utilizado enxerto costocondral fixado com dois parafusos de 2.0 mm de diâmetro. Esse tratamento possibilitou um bom resultado funcional e estético a longo prazo.
Palavras-chave: Fratura condilar; reconstrução condilar; enxerto costocondral
There is still much controversy concerning mandibular condylar fractures. Becker(1) (1952) and Schwipper & Keutken(2) (1985) recommend open reduction with condylar osteosynthesis in fracture dislocations. Other professionals do not recommend surgery and only perform rigid maxillomandibular immobilization for a week, followed by rubber bands physiotherapy based on occlusion (Melmed(3), 1972).
The indication for surgery must be based on clinical rather than radiographic aspects. Inadequate occlusion associated with an open bite and limited mandibular movement are the most important indications for surgery. Mandibular condylar fractures without occlusion impairment are frequently observed (Markowitz(4) et al., 1989).
Temperomandibular joint reconstruction is indicated for condylar resorption or for internal degenerative alterations of the joint. The objective of this study is to present the clinical case of a patient submitted to open reduction of a condylar fracture with dislocation that evolved with total resorption of the condyle. Treatment consisted of reconstruction with a costochondral graft.
CLINICAL REPORT
A 14 year-old female patient who fell and hit her chin on the floor. The patient arrived at the Oral and Maxillofacial Surgery section of Irmandade da Santa Casa de Misericórdia of São Paulo Hospital with a six-day history of pain in the left pre-auricular region and inadequate occlusion. An X-ray showed a left condylar fracture with medial dislocation of the proximal stub. (Fig.1). The condyle was adhered to the lateral pterygoid muscle, and did not maintain contact with the remaining mandible.

Fig. 1 -Towne radiographic view in which a left extra-capsular condylar fracture, with medial dislocation of the proximal segment(arrow) is observed.
The patient was submitted to open reduction surgery and condyle fixation through pre-auricular access. Condyle fixation was performed with double steel sutures (Fig. 2), followed by a rigid maxillomandibular immobilization for 3 weeks.
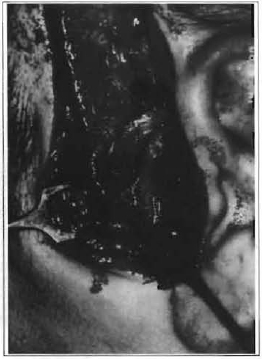
Fig. 2 -Double steel suture fixing the condyle after reduction.
The patient began a physiotherapy program after removal of the maxillomandibular immobilization. Four months after surgery the patient presented a mandibular deviation towards the affected side, along with inadequate occlusion due to shortening of the left mandibular branch (Fig. 3). The patient was referred to an orthodontist to correct occlusion impairment. After 6 months of orthodontic treatment, proper occlusion was not obtained. (Fig.4). The x-ray at the time showed complete resorption of the condyle (Fig.5).

Fig. 3 -Front view of a patient with left mandibular deviation due to shortening of the ipsilateral mandibular branch.
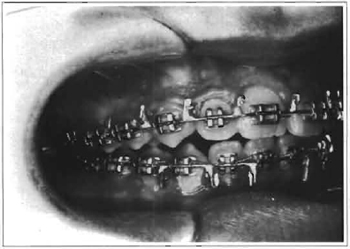
Fig. 4 -Right open bite after trying to solve occlusion impairment with an orthodontic method.
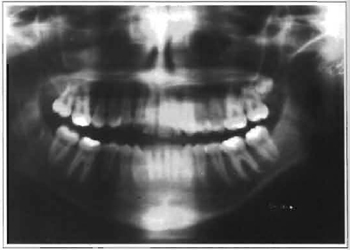
Fig. 5 -Panoramic x-ray of the mandible in which a steel suture and an already reabsorbed condyle may be observed.
One year after the fracture and the first surgery, the patient was operated again. Surgery involved reconstruction of the temporomandibular joint with a costochondral graft and fixation with two 2 mm diameter titanium screws through submandibular access,(Figs. 6A and 6B), along with rotation of a temporalmuscle flap between the graft and the articular fossa.The patient then began rubber bands physiotherapy for 30 days after reconstruction to reestablish occlusion(Fig. 7). Facial symmetry was corrected simultaneously during this period (Fig. 8).

Fig. 6a -Costochondral graft removed to reconstruct the temporomandibular joint.

Fig. 6b -CT-scan showing the fixation of the graft with two 2.0 mm diameter titanium screws.
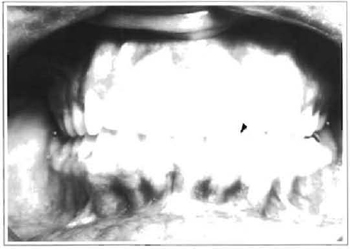
Fig. 7 -Occlusion 30 days after the reconstruction of the left temporomandibular joint and rubber physiotherapy.
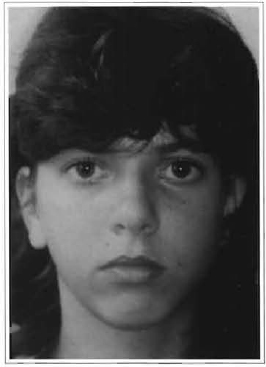
Fig. 8 -Frontal view of the patient 30 days after reconstruction in which the reestablishment of the symmetry of the lower third of the face can be observed.
DISCUSSION
The discussion on the treatment of condylar fractures began 40 years ago with Becker(1) (1952), who indicated surgery, and Thoma(5) (1955), who recommended conservative treatment. Twenty years ago, Melmed(3) (1972) emphasized conservative treatment for these fractures, although Messer(6) (1972) claimed surgery to be the best treatment. Shwipper & Keutken(2) (1985) compared results after clinical or
surgical treatment of condylar fracture dislocations and concluded that stability with miniplates is more efficient than the maxillomandibular immobilization.
We believe surgery should be indicated in cases with major occlusion impairment and condylar dislocation. Some patients present condylar fractures and dislocation without associated occlusion impairment(7).
Cases of condylar resorption after osteosynthesis have been reported in the literature (Iiza & Lindquist(8),1991). Boyne(9) (1989) published a free grafting tech nique of the mandibular condyle; that is, in order to attain reduction, the condyle was removed and fixed afterwards in 35 patients, with no post-operative resorption.
Chen(10) et al. (1997) indicate costochondral grafts in acute condylar fractures whose condyle is severely comminuted.
Prosthetic reconstruction of mandibular condyles has been performed using a variety of materials(Gottlieb(11), 1956; Hartwell & Hall(12), 1974). Markowitz(4) et al. (1989) designed a sliding osteotomy to reposition the condyle. According to these authors, the graft may be reabsorbed or present unpredictable growth. Simpson(13) (1985) reported successful reconstruction of the temporomandibular joint in a series of 11 patients, using a costochondral graft.
Costochondral grafts are indicated to reconstruct condyles and to correct occlusion impairment due to resorption in the area, the temporal muscle being an adequate substitute for the joint disk. We, however, only recommend costochondral grafts in patients who may still potentially grow, as it is believed that the cartilage zone contributes to mandibular growth. The external cortex of the skullcap should be preferable in adult patients, since the mandible will not grow and it is an essentially cortical bone, and therefore, more resistant to resorption than the rib.
REFERENCES
1. BECKER AB. Condylar Fractures. Oral Surg. Oral Med. Oral. Pathol. 1952;5:1282-6.
2. SCHWIPPER V & KEUTKEN K. Conservative or surgical treatment of fractures of the condyle in adults. Proceedings from the 8th International Conference on Oral and Maxillofacial Surgery. Edited by E. Hjorting-Hansen. Quintessence Publ. Co. 1985,179-86.
3. MELMED EP. Fractures of the mandible. Ann. Roy. Coll. Surgeons England. 1972;50:371-81.
4. MARKOWITZ NR, ALLAN PG, DUFFY MT. Reconstruction of the mandibular condyle using ramus osteotomies. J. Oral Maxillofac. Surg. 1989,47:367-77.
5. THOMA KH. Displacement of condyle in fracture-dislocations of the mandible. Oral Surg. Oral Med. Oral Pathol. 1955;8:774-82.
6. MESSER EJ. A simplified method for fixation of the fractured mandibular condyle. J. Oral Maxillofac. Surg.1972;30:442-3.
7. MANGANELLO-SOUZA LC, VITA J, FISCHMAN R, SILVEIRA ME. Estudo de 32 casos de fraturas do côndilo mandibular. Rev. A Folha Médica. 1982;85(1):825-30.
8. IIZA T & LINDQUIST C. Severe bone resorption after miniplate fixation of high condylar fractures. Oral Surg. Oral Med. Oral. Pathol. 1991;72:400-3.
9. BOYNE PJ. Free grafting of traumatically dispaced or resected mandibular condyles. J. Oral Maxillofac. Surg. 1989;47:228-32.
10. CHEN C, LAI J, CHEN Y. Costochondral graft in acute mandibular condylar fracture. Plast. Reconstr. Surg. 1997;100:1234-9.
11. GOTTLIEB O. Temporomandibular arthroplasty. Oral Surg. 1956;9:362-6.
12. HARTWELL SW & HALL MD. Mandibular condylectomy with silicone rubber replacement. Plast. Reconstr. Surg. 1974;53:440-4.
13. SIMPSON W. The costocondral graft. Proceedings from the 8th International Conference on Oral and Maxillofacial Surgery. Edited by E. Hjorting-Hansen. Quintessence Publ. Co. 1985;531-6.
I. Scientific Coordinator of the Sector of Oral and Maxillofacial Surgery of the Department of surgery of Santa Casa de São Paulo Hospital.
II. Oral and Maxillofacial Surgery Resident at Santa Casa de São Paulo Hospital.
Address for correspondence:
Luiz Carlos Manganello-Souza, MD
Rua Itapeva, 500 -1º andar Cj.l
01332-000 -São Paulo -SP Brazil
Fone: (55 11) 288-7168
Study performed at Santa Casa de Misericórdia of the São Paulo Medical School.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket