



Articles - Year 2001 - Volume 16 -
Reconstruction of Fingertip Pulp Loss
Reconstrução de Perdas de Substância Digitais Distais
ABSTRACT
The loss of volar fingertip pulp is frequent in hand trauma. Eighty-six homodigital flaps (22 Tranquilli; 20 Hueston; 40 Single Pedicle Island and 4 Kuttler) were performed from January 1994 to July 1998) to repair volar fingertip substance loss, except for the thumb. The mean age was 28 years (ranging from 18 -58) and the average post-operative follow-up period was 12 months. We analyzed advancements, sensitivity and cold intolerance for each flap used: Tranquilli (0.4 cm / 8 mm / 6); Kuttler (0.3 cm / 10 mm / 3); Hueston (1.0 cm / 9mm / 5); Single Pedicle Island (1.5 cm / 8 mm/ 6). The single pedicle island flap was demonstrated to be clearly better in all aspects analyzed. We consider the utilization of homodigital flaps the first choice alternative for reconstructing fingertips.
Keywords: Hand trauma; fingertip loss; homodigital flaps
RESUMO
As perdas de substâncias digitais distais volares apresentam-se com freqüência nos traumas da mão.
De janeiro de 1994 a julho de 1998, 86 retalhos homodigitais (22 Tranquilli; 20 Hueston; 40 Ilha Unipediculado e 4 Kuttler) foram realizados para reparar perdas de substância distais volares, excluindo o polegar. A idade média foi de 28 anos (extremos 18 - 58) e o tempo de seguimento médio pós-operatório foi de 12 meses.
Analisamos o avançamento obtido, a sensibilidade e a intolerância ao frio de cada retalho utilizado. Tranquilli (0,4 cm/ 8 mm/ 6); Kuttler (0,3 cm/ 10 mm/ 3); Hueston (1,0 cm/ 9mm/ 5); Ilha Unipediculado (1,5 cm/ 8 mm/ 6). O retalho em ilha unipediculado mostrou-se nitidamente superior em todos os aspectos analisados.
Consideramos que a utilização de retalhos homodigitais constitui a alternativa de primeira escolha na reconstrução da extremidade digital.
Palavras-chave: Trauma de mão; perdas digitais distais; retalhos homodigitais
Volar fingertip pulp loss (PL) is frequently observed after hand trauma. These lesions pose a twofold therapeutic problem: the need to offer good quality skin coverage and to restore functional sensitivity. Many types of skin coverage have been described (1,2,3). Surgical indication depends on the finger affected, and the type and extension of the injury.
We analyzed a series of 86 homodigital flaps, from the descriptive and retrospective point of view, for volar fingertip PL, regarding indications, advantages and disadvantages of each technique (Tranquilli-Leali, Hueston, Single Pedicle Island and Kuttler).
METHODS
Between January 1994 and July 1998, 86 homodigital flaps were performed at the Plastic Surgery Service of São Lucas Hospital -PUCRS and the SOS-Hand Clinic in Porto Alegre -RS. The mean patient age was 28 years (ranging from 18-58). The mean postoperative follow-up was 12 months (6-40).
TRANQUILLI-LEALI FLAP (22 cases: 18 men, 4 women. / 8 index; 6 middle; 4 ring; and 2 little fingers).
The method initially described by Tranquilli-Leali in 1935(4), became widely known after Atasoy(1). It is indicated for transversal and oblique distal injuries.
The mean advancement was 0.5 cm. It is a triangular palmar flap on the fingertip, with its vertex at the flexion of the distal interphalangeal (DIP) fold. Dissection is performed by divulsion and advancement, then fixing the flap with a hypodermic needle or non-absorbing sutures.
HUESTON FLAP (20 cases: 10 men, 10 women. / 8 index; 6 middle; 6 ring fingers.) This technique described by Hueston(5) allows covering transversal and oblique PL. It consists of an "L" flap, with a longitudinal incision on the lateral border of the finger, followed by a transversal incision at the flexion fold, that allows rotating and covering of the injury. The triangular donor zone, can be covered with a skin graft or directed scarring.
SINGLE PEDICLE ISLAND FLAP (40 cases: 25 men, 15 women / 15 index; 10 middle; 10 ring; 5 little fingers).
Linler(6) was the first to use a heterodigital, single pedicle flap. Joshi, in 1974(7), described a dorsolateral island flap for reconstructing PL of the fingertip. An island of volar skin proximal and contiguous to the PL is marked. The pedicle is identified and dissected, by means of a Brunner(8) incision, to the proximal fold of the metacarpophalangeal (MP) joint. Up to 2 cm may be gained. The donor area is covered by a partial or total skin graft. The procedure ends by immobilizing the "intrinsic plus" position (MP in 45° to 70° flexion, PIP and DIP extended) (Figs. 1 to 5).
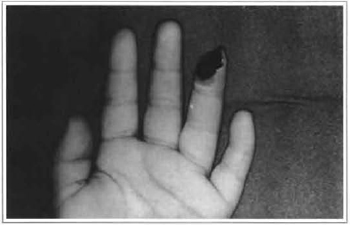
Fig. 1 -Pulp loss, dominant pulp, ring finger, 7 year-old girl.

Fig. 2 -Dissected island flap.

Fig. 3 -Distal island flap.

Fig. 4 -Aesthetic result.
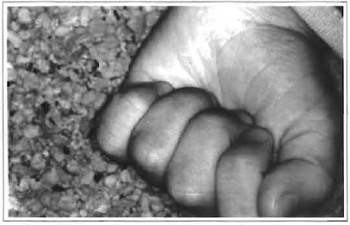
Fig. 5 -Functional result.
KUTTLER FLAP (4 cases: 2 men, 2 women, / 2 ring; 2 little fingers).
The method described in 1947(9), consists of two triangular lateral and symmetrical flaps, sutured at the median line, for transversal amputations. The incision of the flaps should not go beyond the distal flexion fold of the joint DIP. The dislocation with posterior traction advances the flaps over the amputated part, and the suture is performed at the median line. The defect of the donor area is closed bilaterally in "Y".
RESULTS
A descriptive analysis was performed on this series of 86 homodigital flaps. We analyzed three parameters (Table I): advancement in centimeters, including maximum and mean, sensitivity by static discrimination of 2 points (minimum and mean values) and cold intolerance referred by the patient.
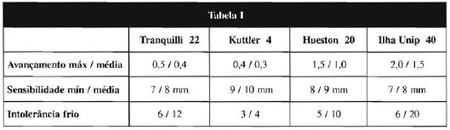
The island flap allowed important advancements, improved sensitivity and led to a smaller percentage of intolerance to cold. On the other hand, the Kuttler flap reached less advancements and the worst sensitivity. No statistically significant difference in relation to age in the sensitivity parameter was observed. Cold intolerance was considered to be more uncomfortable than the usual exposure to cold and referred as functionally significant in 50% of the cases with this complaint (10/20). Patients indicated that their activities were impaired in lower temperatures, a frequent situation in the Southern region of the country. No improvement in this complaint was observed in the average 12-month postoperative follow-up.
DISCUSSION
Due to the importance of fingertip PL, the skin coverage should be adapted to the patient, finger, type and size of the injury.
Many types of skin coverage have been described, from directed healing(10), skin grafting, homo or heterodigital flaps(11) to microsurgery techniques.
Skin grafts should be left to zone 1 PL, in a nondominating pulp. The disadvantages are scar retraction, adherence to subjacent structures and poor sensitivity.
Microsurgical reconstruction demands strict indication criteria.
"Cross finger" or thenar flaps are inconvenient in that they require two surgical procedures and are deficient in terms of discriminatory sensitivity(6). Cronin(l2) has recommended primary neurorrhaphy between a digital pulp sectioned nerve and a sensitive dorsal branch of the donor finger, when cross finger flap for pulp fingertip is used.
Homodigital flaps provide good quality and sensitive skin coverage (11), fundamental aspects for the success of distal volar fingertip loss reconstructions. The flap described by Tranquilli-Leali(4) has the inconvenience of a moderate advancement, limiting its indication. It is preferably indicated for zone 2, either transversal or oblique and asymmetric PL.
The flap proposed by Kuttler(9) has also been indicated for zone 2 PL, but it is impossible to use in asymmetric defects. It has many disadvantages, which justifies the fact that it is seldom used. Partial or total necrosis may be caused by tense suture. Hypersensitivity at the suture line and flap insensitivity have been described(3).
The Hueston flap is indicated to cover small transversal and distal oblique PL. Despite the original description which indicated it for volar loss, its principle may be applied to dorsal PL. Good quality sensitivity is reported, but with a limited rotation arch(5). The secondary triangular defect to flap rotation can be filled in by a total or partial skin graft.
The neurovascular homodigital single pedicle island flap provides sensitivity to the reconstructed pulp. Dorsal skin may be included(7). It can be used for zone 2 or 3 PL. The finger should be immobilized in the "intrinsic plus" position for 10 days (Figs. 6 to 10).

Fig. 6 -Pulp loss, ring finger, 6 year-old boy.

Fig. 7 -Dissected and distally advanced flap.

Fig. 8 -Final aesthetic result.
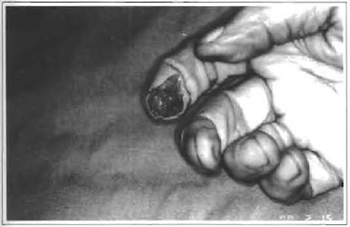
Fig. 9 -Pulp loss, exposure of distal phalange, index finger, dominant hand, 60 year-old man.

Fig. 10 -Final result, compared to contralateral finger.
The indication of a flap depends on the site of injury (dominant pulp, transversal or oblique loss), general health (age and profession) and region (associated injury on the same finger or injury of more than one finger) status.
In conclusion, homodigital flaps are the first choice for covering fingertip injuries.
REFERENCES
1. ATASOY E, IOKIMIDIS E, KASDAN ML, KUTZ JE, KLEINERT HE. Reconstruction of the amputated fingertip with triangular volar flap. J. Bone Joint Surg. 1970;52(A):921-26.
2. BEASLEY R. Reconstruction of amputated finger tips. Plast. Reconstr. Surg. 1969;44(4):349-352.
3. CONOLLY WB, GOULSTON E. Problems of digital amputations : A review of 260 patients and 301 amputations. Australian New Zeland J. Surg. 1973;43:118-23.
4. TRANQUILLI LE. Riconstruzione dell'apice delle falangi ungueali mediante autoplastica volare peduncolata per scorrimento. Infor. Trauma Lavoro. 1935;1:186-93.
5. HUESTON J. Local flap repair of finger tip injuries. Plast. Reconstr. Surg. 1966;37:349-50.
6. LITTLER JW. The neurovascular pedicle method of digital transposition for reconstruction of the hand. Transfer of tissue in reconstructive surgery of the hand. Plast. Reconstr. Surg. 1953;12:303-19.
7. JOSHI BB. A local dorsolateral island flap for restoration on sensation after avulsion injury of fingertip pulp. Plast. Reconstr. Surg. 1974;54(2):175-82.
8. Brunner JM. The zig-zag volar digital incision for flexor tendon surgery. Plast. Reconstr. Surg. 1967;40:571-74.
9. KUTTLER W. A new method for finger tip amputation. JAMA. 1947;133(1):29-30.
10. ALLEN MJ. Conservative management of fingertip injuries in adults. The Hand. 1980;12:257-65.
11. FOUCHER G, SILVA JLB. The use of flaps in treatment of fingertips injuries. World J. Surg. 1991;15:458-62.
12. COHEN BE, CRONIN TD. An innervated cross-finger flap for fingertip reconstruction. Plast. Reconstr. Surg. 1983;72:688-95.
I - Professor of the PUCRS School of Medicine. Certified in Hand Surgery by the Brazilian Medical Association (AMB) and Brazilian Hand Surgery Society Senior Member of the Brazilian Society of Reconstructive Microsurgery.
II - Resident Physician of Plastic Surgery of São Lucas Hospital-PUCRS.
III - Responsible for the Discipline of Plastic Surgery at the PUCRS School of Medicine. Certified in Plastic Surgery by the Brazilian Society of Plastic Surgery.
Address for correspondence:
Jefferson Luis Braga Silva, MD
Av. Ipiranga, 6690
Hospital São Lucas da PUCRS -Centro Clínico -sl. 216
90610-000 -Porto Alegre -RS Brazil
Phone: (55 51) 315-6277
e-mail: jeffmao@zaz.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket