



Case Report - Year 2024 - Volume 39 -
Blepharoplasty with canthopexy in a patient with cutis laxa: A case report
Blefaroplastia com cantopexia em paciente portadora de cútis laxa: Um relato de caso
Jose Isnack Ponte de Alencar1* ; José Alberto Guilherme Frota-Júnior1; Guilherme Pinho Cardoso2; Vitor de Vasconcellos Muniz3; Fernando Soares de Alcântara3; Salustiano Gomes de Pinho Pessoa4
; José Alberto Guilherme Frota-Júnior1; Guilherme Pinho Cardoso2; Vitor de Vasconcellos Muniz3; Fernando Soares de Alcântara3; Salustiano Gomes de Pinho Pessoa4
ABSTRACT
Cutis laxa is a rare connective tissue disease characterized by dysfunction of elastic fibers. Individuals affected by this disease complain about their aged appearance. Treatments are based on the use of cosmetics or surgical techniques, with plastic surgery being an extremely relevant tool. Blepharoplasty aims to improve the senile appearance and provide rejuvenation in the area around the eyes, making the look appear more rested and alert. This is a retrospective observational study using medical record data.
Case Report: A female patient, 17 years old, was referred to the Plastic Surgery Service of the Walter Cantídio University Hospital, Fortaleza-CE, for treatment due to dissatisfaction with her appearance. She underwent upper and lower blepharoplasty associated with canthopexy without canthotomy. In the postoperative period, a satisfactory result was observed for the proposed surgery and adequate correction of existing changes.
Conclusion: The importance of facial surgical correction in cases of lax skin is observed, highlighting the relevance of applying appropriate surgical techniques and improving them in this patient profile.
Keywords: Cutis laxa; Blepharoplasty; Case reports; Eyelids; Plastic surgery procedures
RESUMO
Cútis laxa é uma rara doença do tecido conectivo caracterizada pela disfunção das fibras elásticas. Indivíduos acometidos por essa enfermidade queixam-se de sua aparência envelhecida. Os tratamentos se baseiam no uso de cosméticos ou em técnicas cirúrgicas, sendo a cirurgia plástica uma ferramenta de extrema relevância. A blefaroplastia tem o objetivo de melhorar a aparência senil e proporcionar rejuvenescimento na área ao redor dos olhos, fazendo com que o olhar pareça mais descansado e alerta. Trata-se de um estudo observacional retrospectivo utilizando os dados do prontuário.
Relato do Caso: Paciente do sexo feminino, 17 anos, encaminhada ao serviço de Cirurgia Plástica do Hospital Universitário Walter Cantídio, Fortaleza- CE, para tratamento devido à insatisfação com a sua aparência. Submetida a uma blefaroplastia superior e inferior associada a cantopexia sem cantotomia. No período pós-operatório, foi observado resultado satisfatório para a cirurgia proposta e adequada correção das alterações existentes.
Conclusão: Observa-se a importância da correção cirúrgica facial nos casos de cútis laxa, ressaltando a relevância da aplicação de técnicas cirúrgicas adequadas e o aprimoramento das mesmas nesse perfil de paciente.
Palavras-chave: Cútis laxa; Blefaroplastia; Relatos de casos; Pálpebras; Procedimentos de cirúrgia plástica
INTRODUCTION
Cutis laxa is a rare multisystem disease of connective tissue, characterized by dysfunction of elastic fibers, generating inflexible skin with redundant folds and a wrinkled appearance. Thus, individuals affected by this disease complain about their aged appearance, in addition to having aortic aneurysms and pulmonary problems more frequently1-3. This disorder can be acquired or hereditary - dominant or recessive, the latter presenting symmetrical involvement and usually having a worse prognosis.
Elastic fibers are mainly composed of elastin, a protein from the collagen family that enables tissue flexibility and resistance to tension. In lax cutis, loss of elastin was detected, with the fragmentation of elastic fibers in the reticular dermis causing laxity in the skin, vessels, lungs, and other tissues2.
Treatments are based on the use of cosmetics or surgical techniques as a form of relief or correction, with plastic surgery being an extremely important tool for the therapy of these patients4.
Faced with changes in appearance, most notably in the face, neck, armpit and groin region, there is a great desire on the part of patients for surgical corrections, especially those related to facial changes5.
Of the possible surgical procedures, blepharoplasty surgery, both lower and upper, aims to improve the senile appearance and provide rejuvenation in the area around the eyes, thus making the look appear more rested and alert6.
Traditional lower blepharoplasty is a procedure that, in most cases, brings good results, resulting in a barely noticeable subciliary scar7.
Canthopexy is a surgical procedure performed after classic upper blepharoplasty and lower conjunctival blepharoplasty. In the anterior segment, an ellipse of tissue is removed, as well as a strip of preseptal orbicularis muscle. In the lower part, a conjunctival approach is used to excise the pockets of fat. The surgical technique begins by making an incision in the tissue with an approximate diameter of 2 mm, located instantly below the lateral eyelid corner6,8.
OBJECTIVE
This article aims to report the case of a young patient who underwent superoinferior blepharoplasty with canthopexy to correct anatomical and aesthetic periorbital changes resulting from lax cutis.
CASE REPORT
Female patient, 17 years old, referred to the Plastic Surgery Service of the Walter Cantídio University Hospital, Fortaleza-CE, seeking medical help for treatment due to dissatisfaction with her appearance, especially in the orbital region, in addition to difficulty in social integration due to stigmatization.
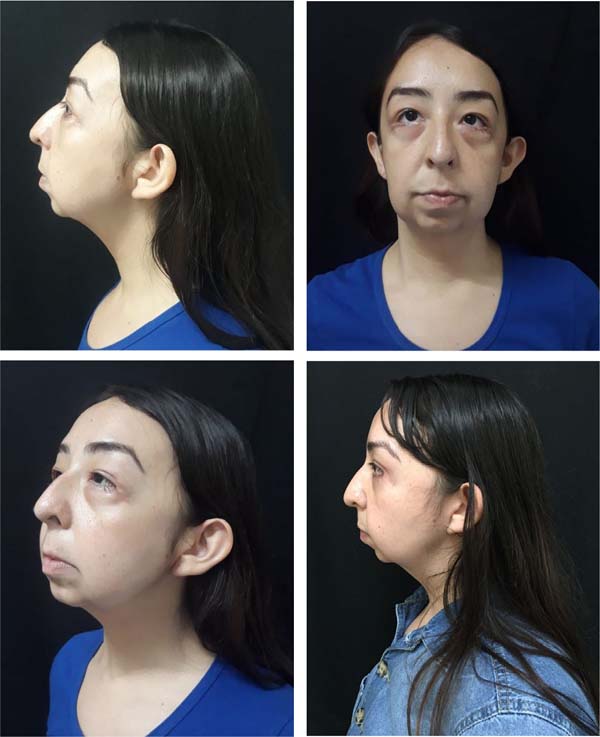
On physical examination, exuberant upper dermatochalasis was evident, with bulging due to herniation of fat pads and bilateral ptosis of the lacrimal glands, contributing to the effect of eyelid pseudoptosis associated with herniation of lower eyelid bags and a rounded corner with a negative canthal angle. (Figure 1). Furthermore, ptosis of the malar tissue was identified with the prominence of the nasolabial fold, increased jowl fat, and retrognathism. Hypertrophy of the upper pole of the ears was also noticed, with slight effacement of the scaphoid fossa associated with turbinate hypertrophy.

During the pre-operative evaluation, complementary tests were carried out looking for cardiopulmonary, respiratory, or large vessel changes relevant to the investigation, which did not demonstrate any changes. During the pre-operative period, the patient signed the Free and Informed Consent Form as approved by the Ethics Committee of the Walter Cantídio University Hospital (CAAE: 50728421.5.0000.5045).
The procedure was carried out on December 15, 2021. Due to the patient’s main complaint regarding her eyelids, we began her treatment with upper and lower blepharoplasty, removing ellipses of skin and fatty pockets, repositioning of the lacrimal glands associated with canthopexy without canthotomy and cantholysis, for better positioning of the canthal angle, refixing the inferior segment of the lateral canthal tendon more internally on the orbital rim close to its insertion.
In the postoperative period, the patient returned to the service’s plastic surgery outpatient clinic on the seventh day to remove stitches from the skin synthesis. Periodic monitoring has been maintained since then. A satisfactory result was observed for the proposed surgery, identifying adequate correction of the existing changes, namely significant dermatochalasis associated with prolapse of the lacrimal glands, as well as the negative canthal angle (Figure 2).


The patient evolved without postoperative complications, being quite satisfied with the result obtained. She continues to be monitored by the Plastic Surgery Service at the Walter Cantídio University Hospital with future proposals for rhytidectomy, chin advancement, or mental prosthesis and otoplasty.
DISCUSSION
Cutis laxa is a genetic disease that causes sagging and redundancy of the skin, leaving an aged appearance in these patients. The changes caused by the disease can lead to social isolation, difficulty interacting, and the worsening of mental illnesses.
Therapeutic planning to correct lesions must be individualized and carried out by surgeons who recognize the dermatological differences of these patients. There are few reports in the literature on the surgical approach to the eyelids in patients with lax skin9,10.
Ozsoy et al.11 described a case of a 20-year-old patient diagnosed with cutis laxa who presented a satisfactory aesthetic result with bilateral upper blepharoplasty without excision of the adipose tissue.
Banks et al.12 reported two cases of patients with lax cutis, one 44 years old and the other 5 years old, who underwent rhytidoplasty with blepharoplasty to correct the aesthetic defects caused by the disease. An acceptable result was observed in the immediate postoperative period, with good healing, but the disease recurred months after the surgical approach due to the chronic defect in collagen metabolism.
CONCLUSION
In view of the above, the importance of facial surgical correction in cases of lax skin is observed, highlighting the importance of applying appropriate surgical techniques and improving them in this patient profile.
Due to the multiplicity of changes, it is still necessary to inform patients that the treatment is not always completed with just one surgical procedure and that other defects are often recommended to be addressed in other operative stages, as proposed for the patient in this case.
REFERENCES
1. Taylor JA. Blueprints plastic surgery. Malden: Blackwell; 2005.
2. Berk DR, Bentley DD, Bayliss SJ, Lind A, Urban Z. Cutis laxa: a review. J Am Acad Dermatol. 2012;66(5):842.e1-17. DOI: 10.1016/j.jaad.2011.01.004
3. Dantas SG, Trope BM, de Magalhães TC, Azulay DR, Quintella DC, Ramos-E-Silva M. Blepharochalasis: A rare presentation of cutis laxa. Actas Dermosifiliogr (Engl Ed). 2019;110(4):327-9. DOI: 10.1016/j.ad.2018.04.006
4. Beighton P, Bull JC, Edgerton MT. Plastic surgery in cutis laxa. Br J Plast Surg. 1970;23(3):285-90. DOI: 10.1016/S0007-1226(70)80057-1
5. Jones AP, Janis JE. Essentials of Plastic Surgery. Q&A Companion. New York: Thieme Medical Publishers; 2016.
6. Lessa S, Sebastiá R, Flores E. Uma Cantopexia Simples. Rev Bras Cir Plást. 1999;14(1):59-70.
7. Cardim VLN, Bazzi K, Silva AS, Silva MG, Santos FM, Salomons RL, et al. Cantopexia e reforço tarsal com retalho de periósteo. Rev Bras Cir Plást. 2013;28(1):36-40.
8. Game J, Morlet N. Lateral canthal fixation using an oblique vertically orientated asymmetric periosteal transposition flap. Clin Exp Ophthalmol. 2007;35(3):204-7. DOI: 10.1111/j.1442-9071.2007.01454.x
9. Misani M, Fontaine S. Cutis Laxa of the face: A case report and review of literature. J Dermatol Res Ther. 2018;4:055. DOI: 10.23937/2469-5750/1510055
10. Xue Y, Chen H, Zeng X, Jiang Y, Sun J. Generalized acquired cutis laxa treated with facial plastic surgery. Eur J Dermatol. 2011;21(1):141-2. DOI: 10.1684/ejd.2011.1206
11. Ozsoy Z, Gozu A, Dayicioglu D, Mete O, Buyukbabani N. Localized cutis laxa and blepharoplasty. Dermatol Surg. 2007;33(12):1510-2; discussion 1512. DOI: 10.1111/j.1524-4725.2007.33326.x
12. Banks ND, Redett RJ, Mofid MZ, Manson PN. Cutis laxa: clinical experience and outcomes. Plast Reconstr Surg. 2003;111(7):2434-42; discussion 2443-4. DOI: 10.1097/01.PRS.0000060800.54979.0C
1. Residente do Serviço de Cirurgia Plástica do
Hospital Universitário Dr. Walter Cantidio - HUWC
2. Universidade Federal do Ceará, Fortaleza, CE,
Brasil
3. Membro Titular SBCP - Staff Serviço de Cirurgia
Plástica do Hospital Universitário Dr. Walter Cantidio - HUWC
4. Membro Titular SBCP - Regente e Chefe do
Servico de Cirurgia Plástica e Microcirurgia Reconstrutiva do Hospital
Universitário Dr. Walter Cantidio - HUWC
Corresponding author: José Isnack Ponte de Alencar Filho Rua Pastor Samuel Munguba, 1290, Rodolfo Teófilo, Fortaleza, CE, Brazil, Zip Code: 60430-372, E-mail: isnack_alencar@yahoo.com
Article received: October 12, 2022.
Article accepted: October 23, 2023.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket