



Original Article - Year 2023 - Volume 38 -
Squamous cell carcinoma of the lower lip: Excision and reconstruction with nasolabial flap
Carcinoma de células escamosas de lábio inferior: Excisão e reconstrução com retalho nasolabial
Emiliano José Canton1 ; Marcelo Lima Pupo Nogueira2,*; Rafael Resende Pereira2; Denilson Marcos Cúrcio3
; Marcelo Lima Pupo Nogueira2,*; Rafael Resende Pereira2; Denilson Marcos Cúrcio3
ABSTRACT
Introduction: Squamous cell carcinoma is the most common malignant tumor of the lips and mainly affects the lower lip. Adequate treatment of this neoplasm must be early and radical, as metastases can occur. Considering that the lips are extremely important in the dynamics and motricity of the face, lip reconstruction after major resections in this region is a challenge for the surgeon in the search for good aesthetic and functional results. This study seeks to present an already established and reliable technique for reconstructing the lower lip after tumor resection, the Karapandizic flap.
Method: In this case review, 4 patients with lower lips reconstructed using the Karapandzic technique in 2013-2022 are retrospectively evaluated.
Results: The most frequently observed complications were hypertrophic scar, lip vermilion suture dehiscence, and microstomia (reduction of oral opening). The cleft lip (microstomia) reduction was partially corrected through dental orthoses, with no need for commissuroplasty in any of the cases. Another contribution of this work is the use of preoperative color echoDoppler, which allows flap planning by checking the viability of the vascular pedicle and the actual positioning of this pedicle, reducing the chances of inadvertent injury to the vessels during surgery.
Conclusion: Even though microstomy is a limitation of this flap, we conclude that this technique meets the need for lower lip reconstruction in large resections, as it can provide satisfactory results in oncological, functional, and aesthetic terms.
Keywords: Surgical flaps; Carcinoma. Reconstructive surgical procedures; Lip; Carcinoma, squamous cell.
RESUMO
Introdução: O carcinoma de células escamosas é o tumor maligno mais frequente dos lábios e acomete principalmente o lábio inferior. O tratamento adequado desta neoplasia deve ser precoce e radical, pois metástases podem ocorrer. Considerando que os lábios têm extrema relevância na dinâmica e motricidade da face, a reconstrução labial após grandes ressecções nesta região é um desafio para o cirurgião na busca de bons resultados estéticos e funcionais. Este estudo busca apresentar uma técnica já consagrada e confiável para a reconstrução do lábio inferior após ressecções tumorais, o retalho de Karapandizic.
Método: Nesta revisão de casos são avaliados, retrospectivamente, 4 pacientes que tiveram o lábio inferior reconstruído por meio da técnica de Karapandzic no período de 2013-2022.
Resultados: As complicações mais frequentemente observadas foram cicatriz hipertrófica, deiscência de sutura em vermelhão de lábio e microstomia (redução da abertura oral). A redução da fenda labial (microstomia) foi corrigida parcialmente através do uso de órteses odontológicas, não havendo necessidade de indicação de comissuroplastia em nenhum dos casos. Outra colaboração deste trabalho refere-se à utilização do ecoDoppler colorido pré-operatório, que permite o planejamento do retalho verificando a viabilidade do pedículo vascular e o real posicionamento deste pedículo, reduzindo as chances de lesão inadvertida dos vasos durante a cirurgia.
Conclusão: Mesmo sendo a microstomia uma limitação deste retalho, concluímos que esta técnica atende à necessidade de reconstrução de lábio inferior em grandes ressecções, uma vez que é capaz de proporcionar resultados satisfatórios em termos oncológicos, funcionais e estéticos.
Palavras-chave: Retalhos cirúrgicos; Carcinoma; Procedimentos cirúrgicos reconstrutivos; Lábio; Carcinoma de células escamosas.
INTRODUCTION
Lips play a fundamental role in people’s daily lives, performing motor functions (facial mimicry, speech articulation, and swallowing) and aesthetic importance, as they represent one of the dynamic centers of the face and significantly impact an individual’s self-esteem and quality of life1.
The main causes of lip deformities result from congenital malformations (cleft lip), trauma, or loss of substance after resection of tumors in this region2.
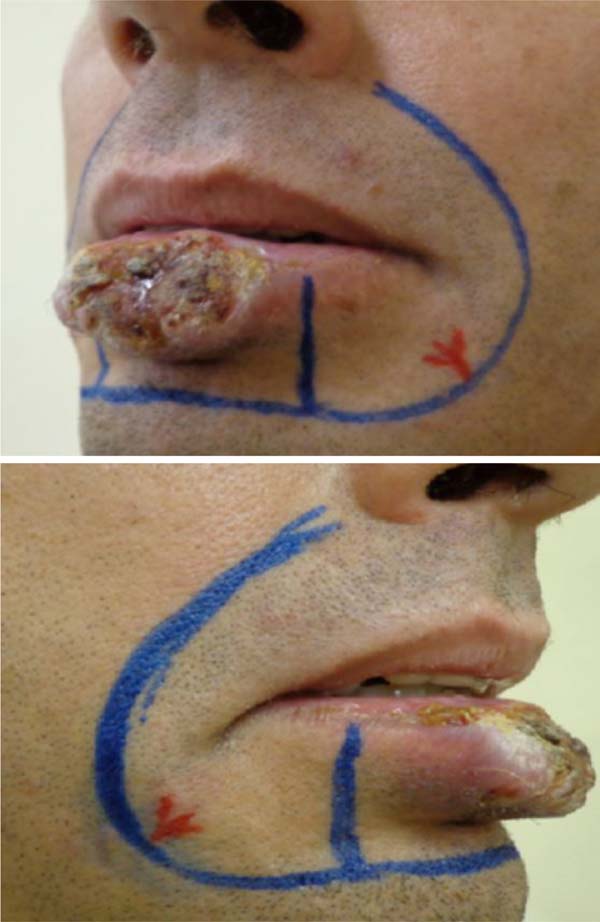
Squamous cell carcinoma (SCC) is the most common malignant tumor of the lips, being most diagnosed on the lower lip3 (Figure 1), and accounts for approximately 25% to 30% of all types of oral cancer. The initial clinical manifestations are atrophy, dryness, and fissures of the lip’s vermilion with an undefined margin between the vermilion and the skin.


They mainly affect patients between 50 and 70 years of age, with males being preferential compared to females4. This fact can be explained because men carry out outdoor activities (mainly outdoor workers) and are more exposed to factors predisposing to lip cancer. It is known that a large part of the male public, compared to the female, tends not to be concerned about protecting themselves against solar radiation, such as lip balm5,6. SCC of the lips has some harmful practices as its main risk factors, such as long-term sun exposure, alcohol consumption, smoking, and genetic predisposition5.
Adequate treatment of this neoplasm must be early and radical, as metastases can occur. The doctor must always be prepared to conduct a meticulous intra and extraoral examination, evaluating any change in normality. Once diagnosed and treated in its initial stage, the progression of the injury can be prevented, establishing immediate treatment and seeking to improve quality of life7. Traditional methods of cancer treatment are surgery, radiotherapy, and chemotherapy. The treatment to be established will depend on the location, degree of malignancy, tumor staging, and the individual’s health condition8.
Lip reconstruction aims to recover the functional aspect while maintaining the sphincter component, seeking maximum preservation of sensitivity and oral opening with a satisfactory aesthetic result. In order to obtain a good result in reconstruction, the following principles must be respected: prioritize function over aesthetics, have local tissue as the first option, reconstitute all damaged planes, and respect aesthetic units1.
Surgical resection with safe margins is the treatment of choice, whenever possible, in the initial approach to SCC of the lower lip. In this context, Gillies was one of the first to describe a technique, in 1920, to transpose the skin and nasolabial mucosa to the lower lip through what he called a fan flap8,9.
This technique was later improved by Gillies and Millard in 195710, and again in 1974, with the description of the Karapandzic11 technique, which is a neurovascular myocutaneous flap that preserves labial vascularization and innervation, requiring careful dissection that does not section the structures vascular and nervous structures, preserving the sensation and motricity of the reconstructed lip. The advantage of this technique is that it is a single-stage surgery, unlike the Abbe flap12, with the ability to preserve both functionality and lip aesthetics.
The Karapandzic flap is an easy-to-perform technique that provides excellent results: a lip with sensation and orbicularis function preserved from the first postoperative day. Oral stoma reduction rarely causes significant problems, and the aesthetic result is excellent because the scars are well positioned, the mouth is symmetrical, and the nasolabial folds do not change. There is no evidence of flap bulging, and long-term results reveal little chance of surgical reintervention; this is where the highlight of this procedure lies, followed closely by the ease with which it is performed7.
Microstomia stands out among the Karapandzic technique’s main disadvantages, especially when reconstructing larger defects13,14. Any injury that directly or indirectly affects the corners of the lips can lead to microstomies (reduction in mouth opening), sometimes serious, with aesthetic and functional impairments (eating, speech, and oral hygiene). Depending on the severity, they require surgical and/or multidisciplinary treatment (dentist, speech therapist)15.
Anatomical considerations
Knowledge of the anatomy of the lip was necessary to indicate the appropriate technique for reconstruction. The circular or semicircular fibers of the orbicularis oris muscle and mentalis muscle represent the labial sphincter component (closure). The dilator component (opening) is formed by the radial fibers of the facial muscles: levator labii superioris and ala nasi, levator labii superioris, zygomaticus major, buccinator, depressor anguli oris, depressor labii inferior, levator anguli oris. Irrigation is provided by the superior and inferior labial arteries, branches of the facial artery. Lymph drains into the submandibular and submental lymph nodes. The infraorbital nerve provides the sensory innervation of the upper lip, the lower lip through the mental nerve, and the motor through the facial nerve16.
Surgical technique
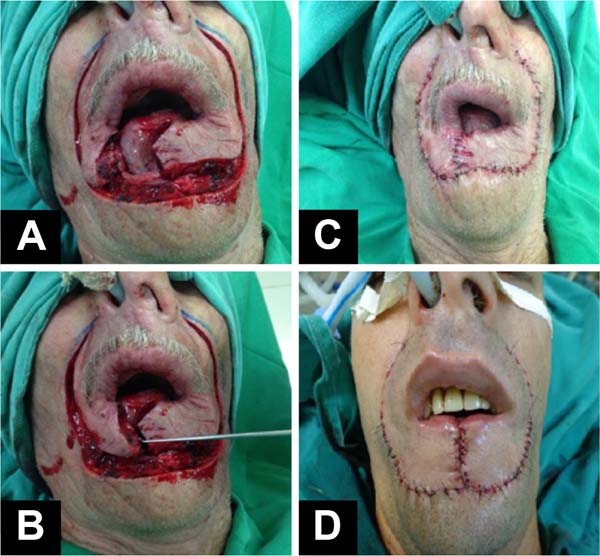
Patients were positioned in the supine position. Markings were made of the tumor area to be resected, the flap lines, and the location of the neurovascular pedicle with the aid of a portable echoDoppler (Figure 2). Subjected to general anesthesia and nasotracheal intubation, antisepsis with 4% chlorhexidine digluconate and asepsis. Local anesthetic infiltration was performed with a 0.5% bupivacaine solution containing vasoconstrictor - adrenaline at 1:200,000. The squamous cell carcinoma was resected with minimum surgical margins of 4mm and hemostasis (Figure 3).



The creation of the flaps was the next step: incision in the right and left nasolabial line, careful dissection of the orbicularis muscle, identification, and preservation of the arterial and venous (upper and lower labial) and nervous branches, obtaining two myocutaneous flaps: right and left. Revision of hemostasis with a bipolar electric scalpel and rotation of the flaps towards the midline. Synthesis of the muscles and mucosa with simple, separate, and inverted sutures with absorbable 4.0 poliglecaprone suture and suture of the skin with 5.0 and 6.0 monofilament nylon threads (Figure 4). Sterile adhesive dressing (Opsite®) was applied to the wound for the first 48 hours. No drains were used.

OBJECTIVE
To demonstrate a reliable and safe option for lower lip reconstruction after excision of squamous cell carcinoma using the Karapandzic technique.
METHOD
A cross-sectional, retrospective, descriptive, and observational study was carried out on patients evaluated and operated on by the main author in the city of Barbacena-MG from June 2013 to January 2022.
The study was approved by the Medical Ethics Committee of the service where it was carried out (CEP approval number: 0001-2022), and the patients signed an Informed Consent Form, including authorization for the dissemination of images for academic purposes. Data was collected by analyzing the electronic medical records of patients operated on by the same plastic surgeon and in the same service. The medical records with “Lower Lip Reconstruction” or “Karapandzic Flap” were collected.
The inclusion criteria for this study were complete medical records, good-quality photographic records, and patients with a minimum postoperative follow-up of 3 months. Exclusion criteria include incomplete medical records, poor quality or missing photographs, patients who did not receive proper postoperative follow-up, and/or patients operated on by another surgeon.
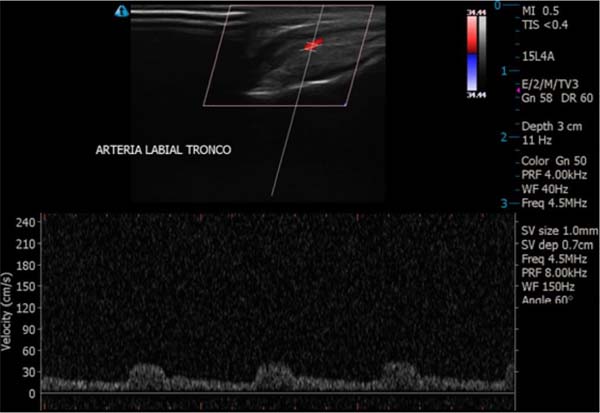
During the period above, 4 patients underwent surgery. All males and evaluated preoperatively with physical and laboratory examinations associated with lip Doppler ultrasound. To identify the superior and inferior labial arteriovenous pedicles, a Mindray M7 portable color Doppler was used by the imaging specialist (Figure 5).


The images analyzed on the device screen in the immediate preoperative period, in the operating room, attest to the viability of the pedicle bilaterally and the location of this pedicle (Figure 6). In addition to checking the viability of the pedicle, marking the correspondence of the arteriovenous bundle on the skin reduces the chances of partial or total perioperative injury to this pedicle.

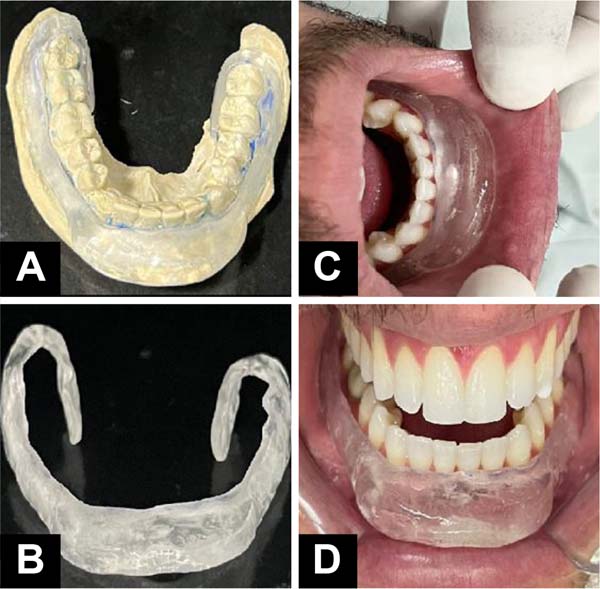
Patients who presented postoperative microstomia were referred to the orthodontist, who created a static orthosis for nighttime use and of an individualized size and specific for tissue expansion. The orthosis used was produced from an alginate mold, then cast in type 2 stone plaster and sent to the dentistry laboratory, which makes the orthosis using an acrylic plate and a metal base supported on the vestibular region of the lower anterior teeth (Figure 7). Expansion sessions begin 60 days after surgery and are performed every 21 or 30 days, adding more polymerizable acrylic to the acrylic plate (Figure 8).


The evolution and results were analyzed through regular postoperative follow-up consultations.
RESULTS
Four patients studied, all male, aged between 35 and 77 years, underwent lower lip reconstruction using the Karapandzic technique, as described in the previous session, after SCC excision and operated between 2013 and 2022. Three patients who did not meet the inclusion criteria were excluded from the study.
The most common risk factors for SCC were smoking, alcohol consumption, fair skin, and chronic sun exposure. The preoperative biopsy (paraffin pathology) confirmed a diagnosis of well or moderately differentiated SCC, obviously with compromised margins. Histopathological analysis (in paraffin) of the piece removed after surgery revealed infiltrating SCC, with depth varying from 3 to 7mm and minimum free surgical margins of 4mm for all cases (Table 1).
| Name | JPPH | JCQ | SPF | MDS |
|---|---|---|---|---|
| Age (years) | 69 | 39 | 77 | 35 |
| Sex | Masculine | Masculine | Masculine | Masculine |
| Risk factors | Smoking and alcoholism | Skin phototype I by Fitzpatrick17 | Smoking, alcohol consumption, and chronic sun exposure | Chronic sun exposure and phototype I skin Fitzpatrick17 |
| Preoperative biopsy (in paraffin) | Well-differentiated infiltrating SCC | SCC moderately differentiated and invasive |
SCC | SCC |
| Surgical margins postoperative | Free | Free and broad | Free | Free |
| Depth | 3mm | 7mm | 6mm | 5mm |
| Postoperative pathology (in paraffin) | Well-differentiated SCC and infiltrating |
Well-differentiated SCC and infiltrating | Well-differentiated SCC and infiltrating |
Well-differentiated SCC and infiltrating |
| Postoperative complications | - | Hypertrophic scar | Partial dehiscence and microstomia |
Microstomia |
| Follow-up time | 3 months and 6 days | 3 months and 14 days | 7 months and 23 days | 6 months and 18 days |
SCC: squamous cell carcinoma.

No frozen section biopsies were performed in any of these cases.
The complications and complications detected in this study were considered mild. We found one case of mild hypertrophic scarring and another case of small vermilion dehiscence of the lip. Microstomia occurred in two of the four operated cases. Severe complications such as infection, necrosis, and thromboembolic phenomena, among others, did not occur in this study.
DISCUSSION
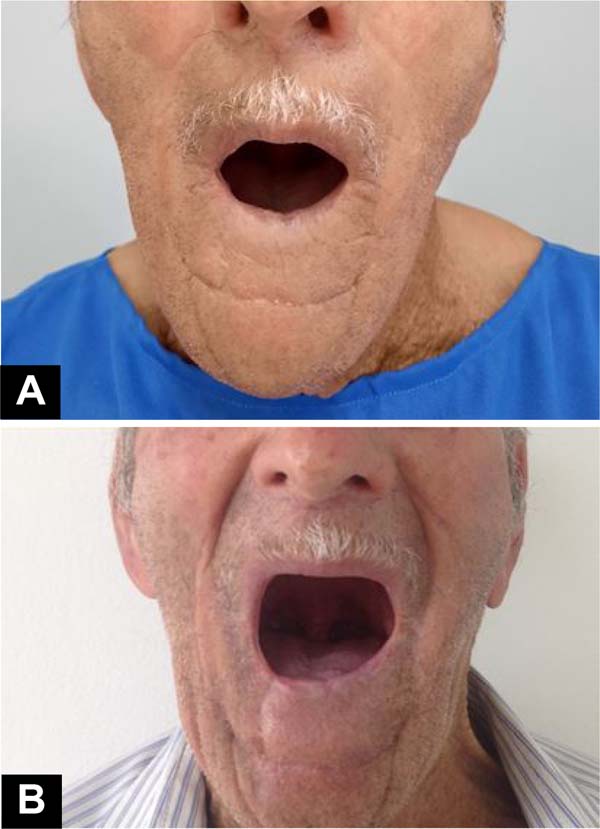
In our study series, there were few complications in patients undergoing the Karapandzic flap, corroborating the idea that this technique meets the needs for lip reconstruction through large resections, bringing good results, both functional and aesthetic (Figures 9 and 10).




Azevedo et al.13 published a case report of two patients who underwent lower lip reconstruction using the Karapandzic technique. One of the patients presented lip dehiscence at the junction of the flaps and required a complementary procedure to refine the aesthetic result, and the other patient had a good aesthetic and functional result without complications.
Matos da Fonseca & Gómez García3 and Guimarães et al.1 published reports on this technique and described the case report of a patient who underwent reconstruction of the lower lip using the Karapandzic technique with good evolution, preserving facial mimicry and lip sensitivity, no functional deficit.
Another study, published by Mendes-Abreu et al.16, reported the case of a patient who underwent the Karapandzic flap due to advanced squamous cell carcinoma of the lower lip, the result of which showed scars filling the physiological grooves, the maintenance of oral continence, lip sensitivity, and mobility, although with slight asymmetry and microstomia without functional impact.
The possible intercurrences and/or complications we report follow the available literature. The published studies do not present a case series with many cases and focus on reporting the flap creation technique and its complications or postoperative complications. Although it is important to highlight that most of these authors considered the final result satisfactory, the most commonly cited complications were lip dehiscence at the junction of the flaps14, slight asymmetry, and microstomia (reduction of the lip cleft) without functional impact7.
The flap described by Karapandzic in 1974 is one of the options for the reconstruction of large lip defects and is based on the anatomical preservation of the facial vascular-nervous pedicles, which maintains the future irrigation and functionality of the lip, with the advantage of being done in a single step18,19. We confirmed all these characteristics with our case study and found that this flap is truly suitable for correcting defects that occupy 40 to 75% of the length of the lower lip and can be applied inverted to reconstruct the upper lip.
The Karapandzic flap preserves the mobility and sensitivity of the lower lip and oral continence. Its biggest drawback is microstomia, described by several authors and which also occurs with other myocutaneous flap techniques, to a greater or lesser extent, used to reconstruct full-thickness surgical defects13,20.
Regarding microstomia, we observed that there were no reports of serious cases, including in our study, and we must consider that microstomia is inherent to this technique and can be described in varying degrees. We chose to improve postoperative results by complementing the treatment with tissue expansion, seeking to obtain skin of the same color, texture, and sensitivity without causing damage to the donor area21.
An expansion prosthesis or orthosis to lengthen commissures and fibrotic muscles may be essential for patients recovering from extensive labral resections. Triad resin prosthesis and pressure regulating screw have already been described with good results22. The microstomia referred to in the present study (Figure 6) was partially corrected with conservative treatments through dental orthoses specially made for each case. Devices made of metal and acrylic for temporary, nighttime use and that promoted tissue expansion of the lower lip.
The advent of controlled expansion had its first clinical use by Neumann23 in 1957 in the reconstruction of the upper pole of the ear and then, in the 1970s, with Radovan24 in work on breast reconstruction, later supported by Austad & Rose25 in 1982, beginning a new era in reconstructive surgery. Tissue expansion makes it possible to obtain skin of the same color, texture, and sensitivity without causing damage to the donor area26.
Another collaboration of this work refers to the use of preoperative color Doppler ultrasound, which allows flap planning by checking the viability of the vascular pedicle and the actual positioning of this pedicle, reducing the chances of inadvertent injury to the vessels during surgery, which could result in total or partial loss of a flap in a very important area of the face. Furthermore, it is known that smoking is a frequent risk factor for SCC and has a significant influence on changes in the flow of regional dermal circulation on the face21.
Therefore, even though it is not absolutely necessary, prior marking of the vascular pedicle with echoDoppler is a complement that can increase the safety of the flap. If the unilateral or bilateral viability of the vascular bundle cannot be identified, as in cases of previous trauma, the possibility of ischemia of this flap must be considered, and other surgical techniques must be considered.
CONCLUSION
Reconstruction of the lower lip after resection of extensive squamous cell carcinoma using the Karapandzic technique has proven to be a reliable, safe, and affordable procedure and can be performed in a single procedure and quickly. Furthermore, the technique keeps the vascular-nervous pedicle intact, providing good functional and aesthetic results. Its biggest drawback is the production of microstomia in the early stages, which gradually improves over time and/or the adoption of special tissue expansion measures.
1. Hospital São Francisco de Barbacena, Barbacena, MG, Brazil
2. Hospital Universitário Ciências Médicas de Minas Gerais, Belo Horizonte, MG, Brazil
3. Hospital Municipal Odilon Behrens,Belo Horizonte, MG, Brazil
Corresponding author: Marcelo Lima Pupo Nogueira Rua Capitão Aviador Corteleti, 351, Centro, Barbacena, MG, Brazil, Zip Code: 36200-720, E-mail: marcelolimapn@hotmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket