



Original Article - Year 2023 - Volume 38 -
Perception of size reduction after non-surgical augmentation rhinoplasty: Retrospective analysis of 116 cases
Percepção da redução do tamanho após rinoplastia de aumento não cirúrgica: Análise retrospectiva de 116 casos
Eduardo Antonio Torres Furlanix1* ; Diego Bomfim Saboia1; Maria Laura Miranda da Costa2; Maria Vitória de Araújo Bezerra2; Wendy Gomes Carneiro2
; Diego Bomfim Saboia1; Maria Laura Miranda da Costa2; Maria Vitória de Araújo Bezerra2; Wendy Gomes Carneiro2
ABSTRACT
Introduction: Traditionally, lowering the dorsum is the only method of hump correction. Rare series point to raising the radix as a possible solution. What explains this massive predominance of the reduction procedure? Ineffectiveness of radix and tip augmentation methods? Big nose perception with augmentation procedures? Our objectives are to determine if the perception of reduction occurs in non-surgical rhinoplasty (NSR), performed exclusively with volume addition, and if the perception of reduction is important in NSR.
Method: Retrospective analysis of 116 consecutive patients undergoing NSR. The patients' images were analyzed by 12 independent observers who evaluated the perceived changes in the nose's size and the correction's quality, giving scores from 1 to 10 for both questions. As for size, 1 represented much smaller than before, 5 same size (neutrality), and 10 much larger than before. The quality of correction was graded from 1 to 10.
Results: 92 cases (79%) were considered size reduction, while 20 cases (17%) were considered enlargement. There was a perception of a reduction in the average size scores (4.71). The mean correction quality was 8.28 on a scale of 1 to 10. Furthermore, our results suggest that there may be an indirect correlation between perceived size and correction quality.
Conclusion: The increase provided by the NSR can cause a perception of a reduction in the size of the nose, and the degree of perceived reduction can be directly related to the degree of perceived quality of the correction.
Keywords: Rhinoplasty; Dermal fillers; Size perception; Reconstructive surgical procedures; Hyaluronic acid
RESUMO
Introdução: Tradicionalmente, o rebaixamento do dorso é o único método de correção da
giba. Raras séries apontam a elevação do radix como possível solução. O que
explica essa maciça predominância do procedimento redutor? Ineficácia dos
métodos de aumento de radix e ponta? Percepção de nariz grande com os
procedimentos de aumento? Nossos objetivos são descobrir se a percepção de
redução ocorre na rinoplastia não cirúrgica (RNC), feita exclusivamente com
adição de volume, e se a percepção de redução é importante na RNC.
Método: Análise retrospectiva de 116 pacientes consecutivos submetidos a RNC. As
imagens dos pacientes foram analisadas por 12 observadores independentes que
avaliaram as mudanças percebidas no tamanho do nariz e a qualidade da
correção, dando notas de 1 a 10 para os dois quesitos. Quanto ao tamanho, 1
representava muito menor que antes, 5 mesmo tamanho (neutralidade) e 10
muito maior que antes. A qualidade da correção foi classificada de 1 a
10.
Resultados: 92 casos (79%) foram percebidos como redução do tamanho, enquanto 20 casos
(17%) foram percebidos como aumento. Houve percepção de redução na média das
pontuações de tamanho (4,71). A média da qualidade da correção foi de 8,28
na escala de 1 a 10. Ademais, nossos resultados sugerem que pode haver
correlação indireta entre a percepção do tamanho e a qualidade da
correção.
Conclusão: O aumento proporcionado pela RNC pode causar percepção de redução do tamanho
do nariz, e o grau da redução percebida pode estar diretamente relacionado
ao grau de qualidade percebida da correção.
Palavras-chave: Rinoplastia; Preenchedores dérmicos; Percepção de tamanho; Procedimentos cirúrgicos reconstrutivos; Ácido hialurônico
INTRODUCTION
Classic aesthetic ideals for surgeons and their patients include straight dorsum and projecting tips1-4. For this, hump reduction has been the most applied method5-8. However, this procedure is not the only one possible9,10, in addition to being able to cause aesthetic and functional impairments, such as internal valve insufficiencies, inverted V, supratip deformities, and other complications11,12.
Despite these potential complications, systematic hump removal to correct dorsal convexity remains the most common practice. What explains this massive predominance of the reduction procedure? Ineffectiveness of radix and tip augmentation methods? Since patients usually request reductions, would surgeons fear perceiving a large nose after augmentation procedures13?
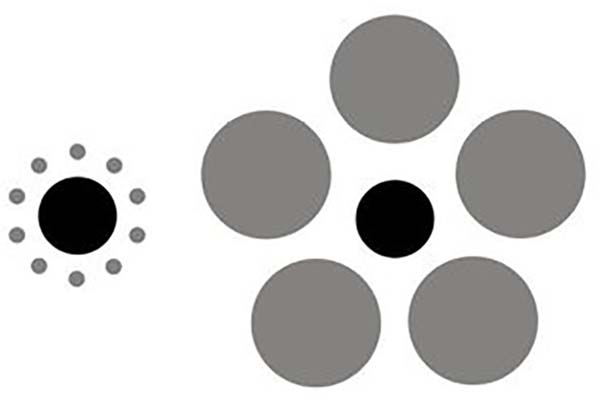
Several authors have investigated the ideas underlying the perception of reduction after augmentation rhinoplasties14-16. For example, Constantian14,15 stated that unbalanced and bottom-heavy noses seem less pleasing and that increasing the radix makes the nose appear smaller. This perception may be due to the phenomenon of the illusion of size contrast, in which the volume of a given structure alters the perception of the volume of adjacent structures, as shown in Figure 117-19.

Our group has previously reported an objective reduction in size perception after radix and tip augmentation20. However, the study had limitations in sample size, which may have weakened the conclusions. To our knowledge, no other study has exclusively investigated the perception of reduction after augmentation procedures.
Although surgical rhinoplasty (SR) has been considered the therapeutic gold standard for individuals who seek to improve the aesthetic appearance of the nose21, exclusive augmentation procedures are often performed by injection of fillers22-25. Early reports of injection molding or non-surgical rhinoplasty (NSR) date back to the mid-1980s. At that time, treatment options were limited to bovine collagen and silicone4,26.
Although the use of dermal fillers in NSR remains an off-label application of hyaluronic acids (HA) and calcium hydroxyapatite (CaHA), its use in the correction of nasal deformities has been widely reported27, and the procedure has been popularly called rhinomodelation.
One of the authors has been practicing NSR for the last five years and observed that, for the primary corrections, the changes are more marked in the profile than in the frontal view. Thus, in these cases of primary correction, it started to indicate the NSR only for patients whose main complaint is in the profile image. Since this procedure has been incorporated into her practice, there have been several opportunities to notice that noses look smaller.
OBJECTIVE
Given the anecdotal evidence of size reduction perceived by patients after NSR, we aimed to assess two questions. Does the perception of reduction occur in the NSR? Is the perception of reduction important in the NSR?
METHOD
The study retrospectively evaluated the perceived size and quality of nose corrections after non-surgical augmentation procedures in a consecutive case series. Primary patients who underwent midline NSR with the main author from February 2015 to October 2018 in Fortaleza - CE were included in the study.
Patients who had undergone surgical or non-surgical nose procedures before the study were excluded. Any nasal filling performed outside the midline was not included. The study was conducted following the principles of the Declaration of Helsinki, and all patients provided informed consent. The Federal University of Ceará Research Ethics Committee approved the study under protocol number 22928719.7.0000.5054.
Image documentation
As the profile view was considered more representative of changes in the nose, only profile images were used in the study. The profile view on the right side was chosen by lot. The images were captured digitally28,29, with a Canon EOS 70D dSLR camera, 20 MPixels (Canon Inc., Tokyo, Japan), and a 135mm lens placed 190cm away from the object. Images were stored in JPEG format. Patients were oriented so that they naturally looked straight ahead30,31.
After photographic documentation, each patient received advice on the possible risks and benefits of the procedure. Only patients who indicated that they wanted to improve their profile view were accepted for treatment. Patients knew their information and photos would be used in the study.
NSR protocol
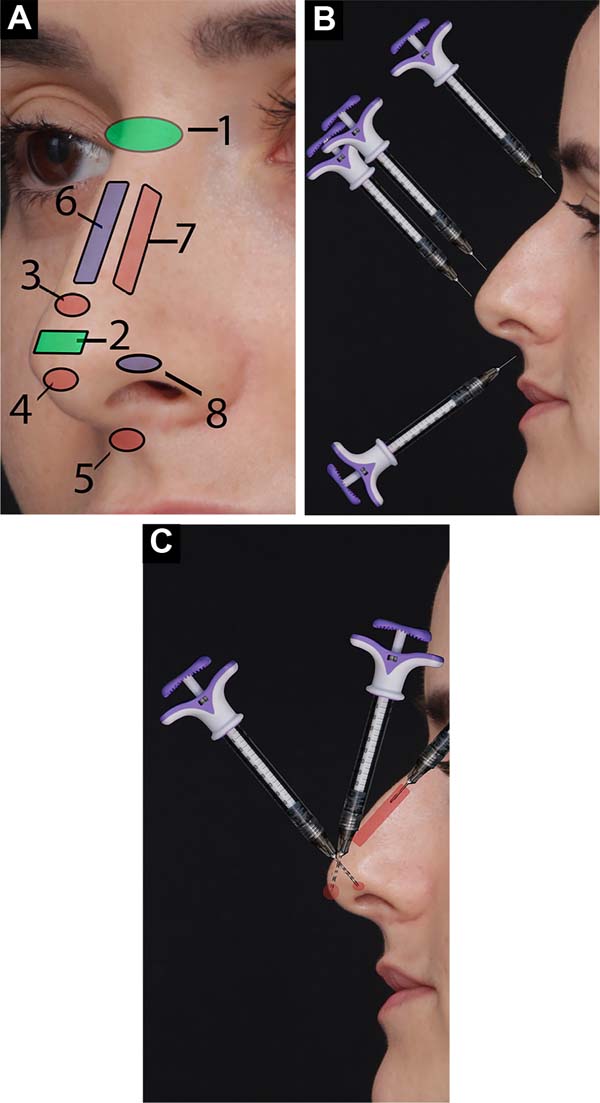
The injection technique followed that described by Wu32-34. Areas to be injected include the radix (nasofrontal angle, just above the periosteum), tip (subcutaneous plane over the domus), supratip (juxtaperichondrial), infratip (subcutaneous), nasal spine (nasolabial fold, subcutaneous), dorsum (anterior aspect of the nasal dorsum in the middle third, juxtaperichondrial). The areas are shown in Figure 2A. After careful aspiration, the injections were made in small boluses (between 0.05cc and 0.1cc) to avoid intravascular injection. A needle was introduced perpendicular to the skin to increase the nasal spine, radix, tip, supratip, and infratip (Figure 2B). To fill the dorsum, a microcannula was used, placed parallel to the skin, deeply (juxtaperichondrial), as in Figure 2C. The Vycross Allergan™ line (Allergan Inc., Irvine, CA, USA).

Photographic documentation was performed immediately after the procedure and at a 6-month follow-up. The physician and staff nurse were available for extra consultations during the follow-up period. During these visits, photographs were taken, and further, HA injections were performed in areas where the injected volume had decreased when necessary. As the study’s objective was to evaluate the perception of the shape/size relationship rather than the longevity of the procedure, only the images obtained after the first procedure were used.
Image preparation and evaluation
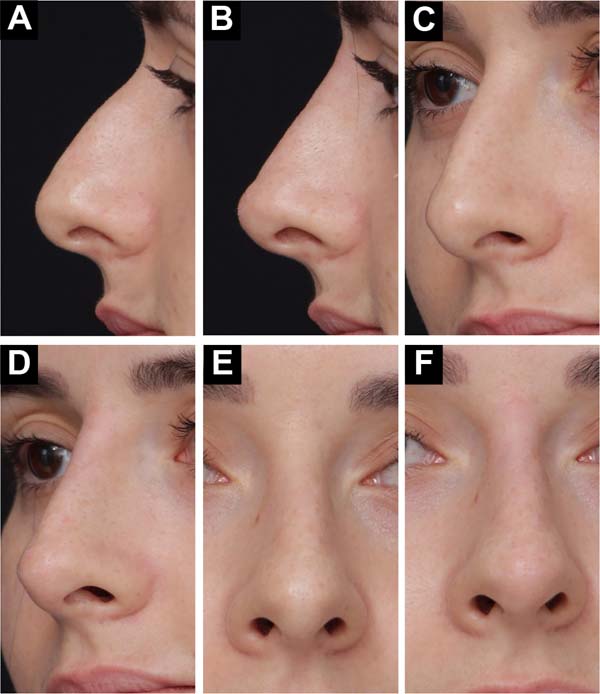
Adobe Photoshop™ software was used to crop the images at the following reference points: superiorly - at the top of the eyebrow; left side - at the most posterior point of the iris; inferiorly - between the upper and lower lip, and; right side - enough to see the background of the image (Figure 3).

The pre-images were placed on the left side, and the post-images on the right side of the screen, with the same size and position. Below each pair of images was a quiz with two questions:
1. Compared to the left image, the right image’s nose is:
1 = much smaller to 10 = much larger. Response:
2. Do you consider this fix:
1 = very bad to 10 = very good.
Response:
All study cases were prepared as described above and entered into a Google form (Google Inc, California, USA). A link was created with the form ready with all the images. The link was sent to the observers through WhatsApp (WhatsApp LLC, Meta, Inc), along with a thank you message for participating in the survey. The evaluation form used in the study can be found at https://forms.gle/xPJmkxM7NFcX2iVD6. Another form with the same content is available in two parts: https://forms.gle/MK4tMCauqUo4zhG2A and https://forms.gle/2aBz8yYrHwiB5x297. The reader is invited to answer the questions.
The evaluators were divided into 3 groups: NSR, SR, and MA. The NSR group consisted of all patients who underwent NSR, in the same service, in the last 3 months, totaling 21. The SR group consisted of all patients who underwent SR in the last 3 months at the same service, totaling 16. The MA group consisted of all patients who underwent breast augmentation in the last 3 months in the same service, totaling 18. All 55 evaluators were unaware of the study objectives. Responses were exported to a Microsoft Excel® spreadsheet (Microsoft Corporation, Redmont, Washington, USA).
RESULTS
One hundred eighty-one consecutive patients underwent NSR between February 2015 and October 2018. Of these, 64 were not included because they had undergone a previous surgical or non-surgical procedure on the nose. Two cases were excluded because post-procedure photographs were not taken.
Therefore, 115 patients were included in the study. They consisted of 14 men (12.06%) and 101 women (87.93%) between 15 and 65 years of age (mean age=35.75 years, standard deviation - SD=10.18). The follow-up period ranged from 174 to 1502 days (mean=550.29 days; SD=227.91).
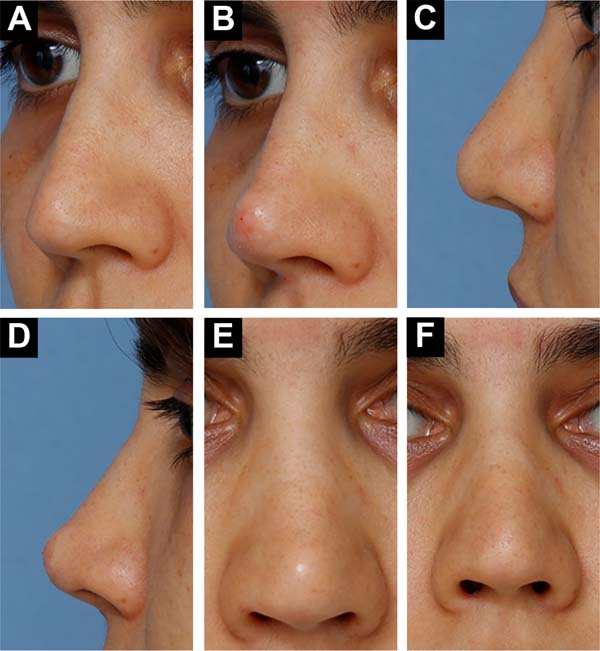
Mild pain and redness for up to 3 days after the procedure were not considered complications. Intermittent redness was also not considered a complication when exposed to low or high temperatures up to 8 weeks after the procedure. One patient (0.85%) was dissatisfied with the result and requested a reversal. She described her nose as having “a ball at the tip” (Figure 4). Hyaluronidase was injected 4 days later, with satisfactory results.

Twelve of the 55 evaluators who received the questionnaire answered it (three from the SR group, five from the NSR group, and four from the MA group). Each rater’s average size perception score was 4.71 (range = 3.08 to 7.00, SD = 0.83). A score of 5.5 was considered neutral. Twenty cases (17%) were perceived as an increase in size, while 92 (79%) were perceived as a reduction in size.
The mean score for correction quality was 8.29 (range=5.83 to 9.58, SD=0.76). Cases that were perceived to be enlarged (size perception score -SPS>5.5) had a mean quality correction score (QCS) of 7.71 (SD=0.7), which was lower than the series mean, from 8.29. Cases perceived as reduced (SPS <5.5) had a mean QSC of 8.41 (SD=0.72), higher than the series mean. The 115 cases were also divided into four groups according to the perceived degree of increase/decrease, as shown in Table 1.
| Group | EMPT* | N** | AQCS*** | SD |
|---|---|---|---|---|
| A | <4 | 19 | 8.68 | 0.88 |
| B | <5 | 77 | 8.55 | 0.7 |
| C | <6 | 107 | 8.32 | 0.68 |
| D | >6 | 8 | 7.82 | 0.68 |
DISCUSSION
Although several augmentation procedures show improvement in contour and respiratory function35, the overwhelming predominance of reduction procedures is still observed7. The surgeon’s reluctance to augmentation procedures can have several causes, such as fear of infection, displacement, visibility, and distortion of grafts35. In addition, patients usually ask to reduce the size of their nose, not to enlarge it36.
In a series by Foda8, there was no increase in the dorsum in any of 500 consecutive cases, despite the hump of the dorsum being the most common diagnosis. Was there no one with a low radix in those 500 cases?
Becker & Pastorek7 raised the radix in 5% to 10% of their cases, while Constantian9,37 found that 38% of their 50 primary cases and 93% of their 150 secondary cases had a low radix or dorsum. Could these authors have a study population so different from Foda8, or is there really a reluctance to perform augmentation rhinoplasty?
Constantian9,14,15,37, who has written extensively on balance concepts, claims that raising the radix of bottom-heavy noses makes them look smaller and prettier. This concept can be very reassuring for surgeons who want to perform augmentation procedures but are concerned about patient reactions.
Unfortunately, the current literature does not provide definitive objective evidence to support this idea. The objective investigation of size perception was carried out in this study to help fill this gap since, as far as we know, only one published article used this approach20.
NSR has proven to be a good testing ground for augmentation rhinoplasty for several reasons. First, there are no concomitant reduction maneuvers. Thus, we guarantee that the reductions do not cause the perception of reduction. Second, it offers immediate results. Third, it is a common procedure that offers wide sampling possibilities. Even so, despite being considered high risk, there is little information about NSR in the medical literature regarding results, technique, and safety. This indicates the urgent need for more studies like the current one.
Although the photographs differ from the real objects, the possible distortions inherent to the method are equally present both in the preand postoperative images, reducing the chance of bias. Digital photography can also be considered valid for this purpose and greatly facilitates everyday life. Therefore, it was chosen as a documentation method29,38,39.
We created one because there is no specific methodology to measure the perception of nose size. For this, we set up a 10-point Likert-type scale40. This new tool was based on the Rhinoplasty Outcome Evaluation questionnaire and a previously published size perception scale of our own20.
The process was also applied to construct the correction quality scale. Although there are some self-assessment tools for quality of life after rhinoplasty, there is no tool to assess the quality of the correction by third parties. As we were trying to assess the influence of shape on the perception of size and correction quality, we believed that external observers would have less bias than patients themselves. Thus, an ordinal numeric ruler was constructed (using a 10-point system from “very poor” to “very good”) to assess correction quality.
Our results showed a mean size perception score (EMPT) of 4.7, which was lower than the neutral point of 5.5. Seventy-nine percent of cases scored below 5.5. This indicates that observers tended to perceive size reduction after augmentation procedures. This is in line with observations by Constantian9,14,15,37, when he suggested that augmentation rhinoplasty may cause a perception of reduction. This is also in line with our results from a previous study20. However, 17% of cases were perceived as enlarged. While this does not suggest a poor correction, the augmentation is not what patients expect. Therefore, these results indicate that further investigations should be carried out to refine the criteria for indicating the procedure.
According to our results, the more perceived reduction, the higher the correction quality score. This may suggest that there is an indirect correlation between these two parameters. Therefore, perception seems to be important in rhinoplasty.
We think non-surgical approaches to correct nose deformities have many limitations and do not replace the surgical approach. NSR can slightly improve appearance in the front view but has almost no effect on wing flair and very little effect on rounded ends. Therefore, we do not indicate the procedure to treat primary patients whose main complaints are focused on frontal vision. Secondary patients who need correction of small irregularities can benefit from NSR, even if the complaint is in the frontal view.
NSR also has limitations for side view corrections. Patients with very low radix often lose part of the treatment effect within a few days. Attempts to correct it with more filler injection may enlarge the area, making the front-view image worse. Patients with a dorsal hump and a radix higher than the supratarsal crease of the upper eyelid have a Roman nose appearance, which may be unpleasant for some. NSR results on very long noses are often disappointing. It is also difficult to achieve good shape in thick-skinned patients, especially in thicker areas such as the tip.
Blindness and skin infarcts have been reported as possible serious complications related to NSR or injection rhinoplasty23. These complications were first reported with HA in 200241. Although we did not experience such complications, our study did not have a large enough sample to attest to the safety of the NSR.
Tansatit et al.42 studied the microscopic soft tissue from the midline from root to tip in 45 cadavers and determined that it was a relatively safe area, with no arteries large enough for cannula embolization. However, compared to other areas, they identified a high-risk area in the subcutaneous plane of the overtip (supratip). The area of the nasal spine has not been studied, but it is known to contain the labial artery and its columellar branch43.
To make the procedure safer, we recommend using cannulas whenever possible. However, when using needles, prefer the juxtaperichondrial or periosteal plane; always aspirate before injecting and do so only in the midline of the nose, avoiding the overlap region. NSR can be a powerful procedure in reaching people who are hesitant to undergo surgery, acting as a bridge to surgical solutions or an end in itself.
CONCLUSION
Enlargement by the NSR may cause a perception of reduced nose size in the profile view. The degree of perceived reduction may be indirectly related to the degree of quality of the correction in the profile view.
1. Clínica Médica Eduardo Furlani, Fortaleza, CE,
Brazil
2. Universidade Federal do Ceará, Faculdade de
Medicina, Fortaleza, CE, Brazil
Corresponding author: Eduardo Antonio Torres Furlani Rua Tibúrcio Cavalcante, 1750, Aldeota, Fortaleza, CE, Brazil., CEP: 60.125-045, E-mail: eduardofurlani@hotmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket