



Original Article - Year 2023 - Volume 38 -
Adherence to the Enhanced Recovery After Surgery (ERAS) protocol in breast reconstruction plastic surgery
Adesão ao protocolo Enhanced Recovery After Surgery (ERAS) em cirurgia plástica de reconstrução mamária
André Gabriel Gruber1* ; Júlia Gonçalves Zandomenico2; Henrique Gioppo Calegari2; Fabiana Schuelter-Trevisol1,2
; Júlia Gonçalves Zandomenico2; Henrique Gioppo Calegari2; Fabiana Schuelter-Trevisol1,2
ABSTRACT
Introduction: The Enhanced Recovery After Surgery Society (ERAS) protocol has revolutionized perioperative care, improving in-hospital management and outcomes for patients undergoing breast reconstruction plastic surgery. This study evaluated adherence to the ERAS protocol recommendations for plastic surgery in two reference hospitals in the country's south.
Method: Cross-sectional study using a medical record database in two hospitals in southern Brazil from 2018 to 2021. The definition of the variables to be evaluated was based on the most recent ERAS protocol proposed by Temple-Oberle and collaborators. The results were analyzed by descriptive epidemiology.
Results: The average rate of compliance with the ERAS protocol per participant was 50.7%. The mean length of stay was 11 hours and 52 minutes. The number of indications with a strong degree of recommendation achieved showed the ability to reduce the length of stay (Spearman ? = -0.397) (p<0.001).
Conclusion: Adherence to perioperative optimization measures in breast reconstruction plastic surgery can reduce patients' hospital stays. However, the average adherence rate per patient is still low, making it evident the need to optimize the care of patients undergoing this surgery.
Keywords: Reconstructive surgical procedures; perioperative care; Enhanced recovery after surgery; Mammaplasty; Anesthesiology; Clinical protocols
RESUMO
Introdução: O protocolo Enhanced Recovery After Surgery Society (ERAS)
revolucionou os cuidados perioperatórios, aprimorando o manejo
intra-hospitalar e melhorando desfechos de pacientes submetidas a cirurgia
plástica de reconstrução mamária. O objetivo deste estudo foi avaliar a
adesão às recomendações do protocolo ERAS para cirurgia plástica em dois
hospitais de referência do Sul do país.
Método: Estudo transversal, utilizando banco de dados de prontuários, em dois
hospitais do Sul do Brasil, nos anos de 2018 a 2021. A definição das
variáveis a serem avaliadas foi baseada no protocolo ERAS mais recente
proposto por Temple-Oberle e colaboradores. Os resultados foram analisados
por epidemiologia descritiva.
Resultados: A taxa média de cumprimento do protocolo ERAS por participante foi de 50,7%.
O tempo médio de internação foi de 11 horas e 52 minutos. A quantidade de
indicações com forte grau de recomendação atingida mostrou capacidade de
diminuir tempo de internação (? de Spearman = -0,397)
(p<0,001).
Conclusão: A adesão a medidas de otimização perioperatória em cirurgia plástica de
reconstrução mamária é capaz de reduzir tempo de internação dos pacientes.
Entretanto, a taxa média de adesão por paciente ainda é baixa, tornando-se
evidente a necessidade de otimizar os cuidados dos pacientes submetidos a
esta cirurgia.
Palavras-chave: Procedimentos cirúrgicos reconstrutivos; Assistência perioperatória; Recuperação pós-cirúrgica melhorada; Mamoplastia; Anestesiologia; Protocolos clínicos
INTRODUCTION
Mastectomy is a procedure that consists of total or partial removal of breast tissue, varying according to the extent of resection of additional tissues (glandular tissue, overlying skin, pectoral muscles, and regional lymph nodes). Its main indications are for treating breast cancer and for prophylaxis in patients at high risk of developing breast cancer (such as patients with mutations in the BRCA1 and BRCA2 genes)1. This surgery constitutes a possible source of psychological stress that hinders the psychosocial functioning of the patient who undergoes it, insofar as he will have to deal with tension and body dysmorphism, in addition to several other related issues2.
Therefore, in recent years, the search for plastic surgeries for post-mastectomy breast reconstruction has been increasing, mainly due to the benefits generated by that procedure, such as the tendency for patients to value quality of life more and to feel more attractive3.
However, performing anesthetic-surgical procedures in patients considered at high perioperative risk can be a challenge, and due to the concern of anesthesiologists and surgeons regarding the safety of the procedure, the current trend is the implementation of protocols that revolutionize perioperative care, improving the in-hospital management of these patients and improving outcomes4.
Among the protocols that aim to improve the recovery of patients after surgery, the systematic review of meta-analyses endorsed by the Enhanced Recovery After Surgery Society (ERAS) stands out. This protocol consists of a consensus of recommendations based on scientific evidence, which aim to promote optimal perioperative care and generate an improved recovery, even after breast reconstruction plastic surgery5.
Through this set of recommendations, it is possible to ensure a safer and more efficient approach to pre-, intra-, and postoperative care. The implementation of the protocol can bring significant benefits, such as patient engagement, mitigation of the physiological stress associated with the surgery, reduction of avoidable postoperative complications (reduction of morbidity and mortality, faster recovery, reduction of hospital stay), resulting in a reduction in hospital costs and decrease in hospital readmission rates within 30 days6.
OBJECTIVE
The present study sought to carry out an analysis of the recommendations of the ERAS protocol in breast reconstruction plastic surgery used in two hospitals in the south of the country, generating strategies for the implementation of a protocol that aligns practice with scientific evidence, promotes institutional leadership and encourages work in a team, engaging all parties involved in patient care, in addition to the other previously mentioned benefits7.
METHOD
Cross-sectional study using a database of physical and electronic medical records. The University of Southern Santa Catarina’s Research Ethics Committee approved the study under opinion 5,570,697, CAAE 59026222.8.0000.5369, on August 9, 2022.
Female patients aged 18 years or older who underwent plastic surgery for post-mastectomy breast reconstruction in two general hospitals in southern Brazil between 2018 and 2021 were evaluated. The sample was of the census type.
Variables related to the patient’s sociodemographic characteristics were collected from the medical records (gender, age, presence of social habits, comorbidities, BMI (Body Mass Index), and the type of procedure to be performed); presence of preoperative advice and guidance, especially regarding smoking cessation, pre-surgery weight loss and alcohol abstinence; performance of pre-surgical computed tomography angiography; preoperative fasting time for clear liquids and solid foods determined by the anesthesiologist; performance of preoperative conditioning with carbohydrates.
Also verified prophylaxis for venous thromboembolism and methods; skin preparation and which substance used; administration of antibiotics before surgery and time of its pre-surgical administration; medications used for postoperative nausea and vomiting (PONV); pre and intraoperative multimodal analgesia; standard anesthetic protocol, containing the type of intraoperative anesthesia used; prevention of intraoperative hypothermia; intraoperatively administered fluids; prescription of postoperative analgesics; time to start oral fluid intake and to walk after surgery; time to hospital discharge. Additionally, we analyzed immediate complications and readmissions.
Categorical variables were presented as absolute frequencies and percentages, and continuous variables as mean and standard deviation (SD). The follow-up rate per patient was calculated by simple arithmetic mean. Spearman’s correlation coefficient was used to assess the statistical dependence between two variables. The adopted statistical significance level was 5% (p<0.05).
RESULTS
During the study period, 99 breast reconstruction procedures were performed, 100% of which were female patients. The median age of patients was 56 years (SD=15.75), ranging from 19 to 81. Mean BMI was 26.97 kg/m2 (SD=4.22). Data related to the study and procedure participants are presented in Table 1.
| Variable | n | % |
|---|---|---|
| Age | ||
| 19-30 years | 15 | 15.2 |
| 31-50 years | 34 | 34.3 |
| > 50 years | 50 | 50.5 |
| Social habits / Comorbidities (pre-admission) | ||
| Smoking | 8 | 8.1 |
| Obesity | 26 | 26.3 |
| Alcoholism | 4 | 4.0 |
| BMI | ||
| < 18.5 | 1 | 1.0 |
| 18.6 - 24.9 | 34 | 34.4 |
| 25.0 - 29.9 | 43 | 43.4 |
| 30.0 - 34.9 | 16 | 16.1 |
| 35.5 - 39.9 | 6 | 5.1 |
| > 40 | - | 0.0 |
| Procedure to be performed | ||
| Prosthesis And/Or Expander | 35 | 35.4 |
| Post-Quadrantectomy Partial Reconstruction | 45 | 45.5 |
| Muscular or myocutaneous flap | 13 | 13.1 |
| Regional Skin Flaps | 6 | 6.1 |
BMI: Body Mass Index.

Of the patients who participated in the study, 100% underwent pre-anesthetic evaluation, receiving information, education, and detailed preoperative counseling, as seen in Figure 1. The data presented are followed by their Level of Evidence (LE).


The optimization of pre-admission - which consists of carrying out, before surgery, one month of abstinence from tobacco for smokers (LE = moderate); one month of abstinence from alcohol for alcoholics (LE = moderate); and weight reduction in obese patients to reach a BMI ≤ 30kg/m2 (LE = high) - was performed by 52.5% of patients. Flap planning, with preoperative mapping of perforating vessels with angiotomography (LE = moderate), was performed by only 1.0% of patients (n=1).
Minimized perioperative fasting was indicated for 84.8% of patients, who were allowed to drink clear liquids up to two hours before surgery (LE = moderate). None of the patients were given preoperative drinks based on maltodextrin in the two hours before the surgery (LE = low).
During the preand intraoperative period, multimodal analgesia to alleviate pain was performed in 100% of patients (LE = moderate). The standard anesthetic protocol with total intravenous anesthesia (TIVA) was not performed on any patient; in contrast, all patients received combined general anesthesia. Preoperative and intraoperative measures to avoid hypothermia, as well as perioperative intravenous fluid management, in an attempt to avoid excessive or insufficient fluid resuscitation (LE = moderate), were indicated in only 2.0% of the medical records (n=2).
Postoperatively, 22.2% of patients were encouraged to take liquids and food orally as soon as possible, preferably within 24 hours after surgery (LE = moderate) (n=22). Frequent monitoring of the flap in the first 72 hours after the operation was indicated by the nursing team in only 2% of the medical records (n=2).
No information was found in the medical records about early mobilization in the first 24 hours after surgery (LE = moderate) and post-discharge home support and physiotherapy (LE = moderate).
The average rate of compliance with the ERAS protocol per participant was 50.7%. Regarding the perioperative procedures performed, as shown in Table 2, surgical management was performed in 99% of patients, all receiving conventional sutures for incisional closure (LE = high) (n=98).
| n | % | |
|---|---|---|
| Wound management | ||
| Conventional suture | 98 | 99.9 |
| NPWT | - | 0.0 |
| Prophylaxis of venous thromboembolism in high-risk patients | ||
| Mechanical prophylaxis | 56 | 56.6 |
| Pharmacological prophylaxis with LMWH | 24 | 24.2 |
| Pharmacological prophylaxis with UFH | 23 | 23.1 |
| Skin preparation | ||
| Chlorhexidine | 90 | 90.9 |
| Antibiotic given within 1 hour before incision | 97 | 98.0 |
| Alcoholism | 4 | 4.0 |
| Medications for VONV | ||
| Dexamethasone | 65 | 65.7 |
| Ondansetron | 67 | 67.7 |
| Metoclopramide | 36 | 36.7 |
| Other | 11 | 11.1 |
| Pre and intraoperative analgesia and sedation | ||
| Opioid | 99 | 100.0 |
| Muscle relaxant | 99 | 100.0 |
| Benzodiazepine | 99 | 100.0 |
| Standard anesthetic protocol | ||
| TIVA | - | 0.0 |
| Balanced general anesthesia | 99 | 100.0 |
| Postoperative analgesia | ||
| Dipyrone | 44 | 44.4 |
| Acetaminophen | 60 | 60.6 |
| INES | 68 | 68.7 |
| Corticosteroid | 36 | 36.4 |
| Weak opioida | 21 | 21.2 |
| Strong opioidb | 29 | 29.3 |
| Other | 8 | 8.1 |

The risk of venous thromboembolism was assessed in 80.8% of patients (n=80), with 56.6% receiving mechanical methods for prophylaxis (n=56); 24.2% received low molecular weight heparin (LMWH) (n=24); and 23.1% received unfractionated heparin (UFH) (n=23) until ambulation or discharge (LE = moderate). Antimicrobial prophylaxis was performed in 99.0% of patients (LE = moderate) (n=98). Of these, 90.9% had their skin prepped with chlorhexidine (n=90), and 98.0% received intravenous antibiotics covering common skin organisms within one hour of incision (n=97).
Preand intraoperative medications to attenuate postoperative nausea and vomiting were administered to 85.9% of patients (LE = moderate) (n=85). Of the drugs used: dexamethasone 65.7% (n=65); ondansetron 67.7% (n=67); metoclopramide 36.7% (n=36); and another 11.1% (n=11). For pain control, 100% of patients received multimodal drug regimens (LE = high).
Of these drugs: dipyrone 44.4% (n=44); acetaminophen 60.6% (n=60); non-steroidal anti-inflammatory drugs (NSAIDs) 68.7% (n=68); corticosteroid 36.4 (n=36); weak opioid (codeine, tramadol, dextropropoxyphene, hydrocodone) 21.2% (n=21); strong opioid (fentanyl, methadone, hydromorphone, morphine, oxycodone) 29.3% (n=29); another 8.1% (n=8).
According to the results shown in Table 3, which represents the postoperative outcomes, all patients were discharged. However, there was a prevalence of 29.3% of cases of complications. The three main causes of complications were pain (15.2%), nausea and vomiting (11.1%), and constipation (3.0%). In addition, 20.2% of patients needed to be readmitted.
| n | % | |
|---|---|---|
| Discharge | 99 | 100.0 |
| Complication | 29 | 29.3 |
| Pain | 15 | 15.2 |
| Nausea and vomiting | 11 | 11.1 |
| Cold | 3 | 3.0 |
| Readmission | 20 | 20.2 |

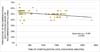
When analyzing the mean length of stay (11 hours and 52 minutes) and its relationship with the number of indications with a strong degree of recommendation achieved, a moderate negative correlation was observed between the variables. Figure 2 shows this statistical dependence as a decreasing monotonic trend; that is, as the number of indications with a strong degree of recommendation achieved increases, the length of stay decreases until the patient is discharged (Spearman ρ = -0.397) (p<0.001).

DISCUSSION
Each element of the ERAS protocol is designed to decrease the physiological stress of the surgical intervention, and there is evidence in the literature that each recommendation is associated with several clinical benefits, including a shorter hospital stay. However, low adherence or implementing only a few recommendations is insufficient to achieve all the expected benefits. Compliance with most items can be crucial to achieving a desired clinical outcome, producing greater clinical benefits than their parts8.
The present study’s results align with a pilot study of ERAS in the National Surgical Quality Improvement Program (PNMQC) of the American College of Surgeons (ACS), which included 16 hospitals that implemented the protocol in more than 1,500 patients. The study found that the mean length of stay increases as adherence to the ERAS protocol decreases (p<0.001), reinforcing the importance of complete adherence to recommendations to achieve the expected clinical benefits8,9.
This information is important, as most patients with breast cancer have a time-dependent disease, which means that the recovery time and the effectiveness of the treatment directly affect the post-mastectomy result; that is, the faster and more effective the recovery, the greater the chance of cure or control of the disease. Furthermore, mastectomy is often followed by additional therapies such as chemotherapy and radiotherapy, which can also have significant adverse effects. Therefore, recovery optimization can help to minimize the total treatment time and reduce the risk of related complications10.
It is known that not all ERAS protocol steps apply to each patient. However, collecting data from medical records about their adherence at an individual level allows providers to identify which protocol components are problematic and target their interventions to improve compliance9.
In this order of ideas, we have, for example, that, during the preoperative evaluation, smoking cessation should be oriented to all patients; however, only half reached this recommendation. Studies point out that the persistence of smoking in the perioperative period results in higher rates of postoperative complications, mainly infection of the incisional wound11. Spontaneous smoking cessation is related to several biopsychosocial factors. Therefore, to achieve this recommendation, it is necessary to implement a multidisciplinary follow-up12.
Preoperative optimization using carbohydrates such as maltodextrin prevents the catabolic state induced by the surgical stress response, reduces postoperative nitrogen and protein losses, helps maintain lean body mass and muscle strength, and decreases insulin resistance. Added to this, it reduces preoperative thirst, hunger, and anxiety13. This recommendation, however, still qualifies as a low level of evidence, and its benefits vary according to the type of surgery and the patient evaluated, which would explain the low adherence in the target sites of the present study14.
In large centers, physiotherapy is still performed in the post-anesthetic recovery room, even with the patient on mechanical ventilation15. This study, however, demonstrated that there was no early mobilization in the patients studied. As a result of the various barriers that are imposed on this recommendation, its implementation requires the efforts and engagement of a multidisciplinary team.
Furthermore, it was noted that the analgesia was administered intravenously, predominantly, which goes against the current literature, which recommends multimodal perioperative analgesia, using combinations of analgesic medications that act in different sites and routes, in an additive or synergistic, to obtain pain relief with minimal or non-existent consumption of opioids16.
A standard anesthetic protocol with TIVA is intended to minimize anesthetic side effects and facilitate rapid awakening and recovery after surgery. However, compared to balanced techniques, the superiority in choosing this anesthetic technique was seen only in some specific situations. Among the main obstacles to its adherence are the high cost, the low availability of equipment, and the need to train professionals who are possibly already used to other techniques, according to the respective anesthesiology service17.
It is known that hypothermia occurs in 70% of patients undergoing operations lasting two or more hours, increasing intraoperative blood loss. It is usually preventable through active warming using a blanket and thermal mattress. The use of dynamic monitors and fluid-responsiveness measurements also guide fluid utilization. However, in small to moderate surgeries with a non-prolonged duration and low risk of bleeding, the cost and availability of these instruments often constitute an obstacle to their use18.
Adherence to the ERAS protocol can be deficient due to several reasons. One of the main barriers is the lack of knowledge of the protocol by health professionals who are part of the surgical team. The difficulty of raising awareness about the need to change habitual behaviors can be hard in this process. Another barrier may be the lack of resources or adequate infrastructure to implement the protocol, especially in smaller hospitals or with fewer available resources19.
To achieve better clinical outcomes, these barriers must be addressed and overcome. Education of surgical teams and training for the ERAS protocol can be essential to improve adherence and understanding of the corresponding benefits. It is also important to provide adequate support and resources for implementing the protocol in hospitals, including the availability of a multidisciplinary team to support its implementation. Continuous monitoring and evaluation of results are essential to ensure that the protocol is being properly implemented and to identify opportunities for improvement20.
Furthermore, the ERAS protocol offers a unique opportunity to leverage existing resources by instituting a standardized approach to anesthesia and surgery-related challenges. This allows growing hospitals to increase their bed capacity and, consequently, the surgical volume, generating a potential increase in gross revenue due to the savings in hospitalization days21.
CONCLUSION
The average rate of compliance with the ERAS protocol per participant was 50.73%. The mean length of stay was 11 hours and 52 minutes. The number of indications with a strong degree of recommendation achieved showed the ability to reduce the time, in minutes, from hospitalization to discharge (Spearman’s ρ = -0.397) (p<0.001). This demonstrates the need for greater protocol adherence to reduce the length of hospital stay.
Study limitations
It is important to consider the inherent limitations of ecological studies that use medical records as a database. One of the main concerns is the quality of the data, which can vary widely between health professionals responsible for completing the records, affecting the accuracy of the results obtained and the validity of the conclusions reached. Another important aspect to be considered is data availability. Medical records do not always contain all the information relevant to a study, which may limit researchers’ ability to explore certain questions. In addition, charts are generally collected from a specific sample of patients in a particular geographic location, which may restrict the generalizability of results to other populations or locations.
1. Universidade do Sul de Santa Catarina, Tubarão,
SC, Brazil
2. Nossa Senhora da Conceição, Tubarão, SC,
Brazil
Corresponding author: André Gabriel Gruber Avenida José Acácio Moreira, 787, Tubarão, SC, Brazil., Zip Code: 88704-900, E-mail: andre.gruber@hotmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket