



Original Article - Year 2004 - Volume 19 -
Translation into Portuguese, Cultural Adaptation and Validation of the Rosenberg Self-esteem Scale
Adaptação Cultural e Validação da Versão Brasileira da Escala de Auto-estima de Rosenberg
ABSTRACT
The authors had as objectives: to translate into Portuguese, culturally adapt and validate the Rosenberg self-esteem scale to be used in a population which will be submitted to plastic surgery. Conclusion: The Portuguese version of the Rosenberg Self-Esteem scale (UNIFESP-EPM/Rosenberg) proved reliable and valid and can be used as an instrument to measure the self-esteem of patients who will be undergoing cosmetic surgery.
Keywords: Self-esteem; quality of life; questionnaires; psychological tests; self-image; plastic surgery
RESUMO
Os autores tiveram como objetivos: Traduzir para a língua portuguesa, adaptar ao contexto cultural brasileiro e validar a escala de auto-estima de Rosenberg para uma população de pacientes que irão submeter-se à cirurgia plástica. CONCLUSÃO - A versão para a língua portuguesa da escala de auto-estima de Rosenberg (EPM/Rosenberg) apresentou bons índices de reprodutibilidade e validade no nosso meio, podendo ser usada como instrumento para medir a auto-estima de pacientes brasileiros que irão submeter-se à cirurgia plástica.
Palavras-chave: Auto-estima; qualidade de vida; questionários; testes psicológicos; cirurgia plástica
Plastic Surgeons can alter the appearance of their patients and, in this way, influence self-image and self-esteem. Self-esteem may be defined as the feeling, the appreciation and the consideration which a person feels for him or herself, that is to say, how much that person likes him or herself, how he or she sees him or herself and what he or she thinks about him or herself. Self-image is the subjective life center of the individual, determining thoughts, feelings and behavior.
Pre and post-operative photography is part of the routine of plastic surgery as a means of comparing results. The importance of this documentation for the plastic surgeon has been compared to the importnce of the electrocardiogram for the cardiologist(2). Objective data providing concrete evidence concerning plastic surgery results is scarce. Measuring results in this way is necessary so that evidence is created and data may be compared in a standard manner. How can we, therefore, obtain objective numbers as a result of these measurements?
The analysis and quantification of the self-portrait that a person makes of hin or herself is an objective measurement based on social experiences(1). Some standards of behavior and appearance are determined by society, by the media or by the individual. Self-consciousness about appearance can strongly affect self-confidence and self-esteem.
In recent years, instruments to measure quality of life have been widely used to measure results in medicine in an objective way and on a global scale, including international multi-centric studies. In order to compare results obtained in similar studies with culturally and linguistically distinct populations, it is necessary to standardize the process of translation and cultural adaptation of the instruments used. Validation tests of the measuring properties are also required.
There are no valid instruments adapted to the Brazilian cultural context to measure and evaluate the possible self-esteem alterations in patients who have undergone plastic surgery. The objective of this study was to translate into Portuguese, adapt to the Brazilian cultural context and test the measurement properties (reproducibility and validity) of the Rosenberg self-esteem scale for this measurement.
MATERIAL AND METHODS
Translation and Cultural Adaptation
For the translation and cultural adaptation of the Rosenberg self-esteem scale, we used the methodology proposed by Guillemin; Bombardier; Beaton(3) which consisted of:
1. Initial translation of the original questionnaire into Portuguese by two independent translators who were aware of the study objectives, that is, a conceptual rather than strictly literary translation.
These two translations were then compared by a multi-disciplinary group comprising five doctors (4 plastic surgeons and 1 clinical epidemiologist) and one version of the questionnaire was arrived at by consensus (Portuguese version 1). During the translation of the instruments, semantic, idiomatic, experimental and/or cultural and conceptual equivalence were evaluated.
2. Two new translations into English from Portuguese version 1 were then carried out by two other independent translators, who knew neither the original English version of the questionnaire nor the objectives of this work. This process is called back translation.
Again the multi-disciplinary group met to discuss the differences and discrepancies resulting from the translation process. The result of this meeting was a new version of the questionnaire in Portuguese (version number 2) arrived at by consensus.
3. Cultural adaptation
Thereafter, this version was submitted to a cultural equivalence evaluation denominated pre-test. In this the patients were asked to:
a) Explain the question in their own words,
b) Propose changes if they felt that this would make the meaning of the question clearer
c) Give marks denoting the importance of each of these questions.
The relevance of each question was calculated by means of a relevance index that consisted of multiplying the percentage of individuals who awarded the same performance mark, which varied from 1 to 5.
Questions achieving a score above 3 were considered relevant. The multi-disciplinary team met at each stage of change necessary. The cultural equivalence evaluation was considered complete when a group of 10 consecutive patients correctly understood the meaning of the questions and no additional modifications to the questionnaire were necessary, giving rise to the UNIFESP-EPM/ Rosenberg version of the scale.
Reproducibility was tested by means of three interviews. The EPM/Rosenberg self-esteem scale was applied to a population of 32 individuals aged less than 40 years old, of any race, due to undergo plastic surgery, consecutively selected from the plastic surgery outpatients of the Federal University of São Paulo Escola Paulista de Medecina. These were then interviewed by the same observer at different times (with an interval of 2 weeks between the interviews) and by a second observer with an interval of 3 hours between the interviews. Three groups of results were thus obtained. Using this data, we calculated the intra-class correlation coefficient, thereby determining the inter - and intra - observer reproducibility.
Three types of validity were tested: face validity; content validity and construct validity.
Face and content validity were tested by judgment and construct validity by correlating aspects considered part of self-esteem with the Rosenberg Scale score. To evaluate patient population demographic data, descriptive statistical methods were used (mean and deviation- and frequency). The inter- and intra-observer reproducibility were established calculating the observer number 1 in time 1(O1T1) variance analysis, also O2T1 and O1T2 then from this, the intra-class coefficient. The construction validity was obtained by correlation tests (Pearson and Spearman) and multiple regression, which allows an explanation of how much each aspect contributes to the score obtained with the self-esteem scale.
RESULTS
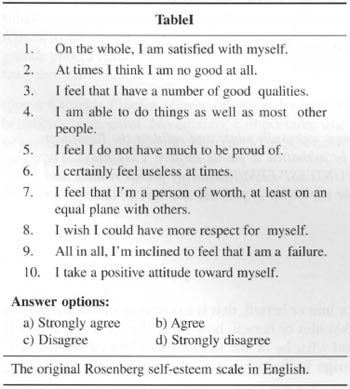
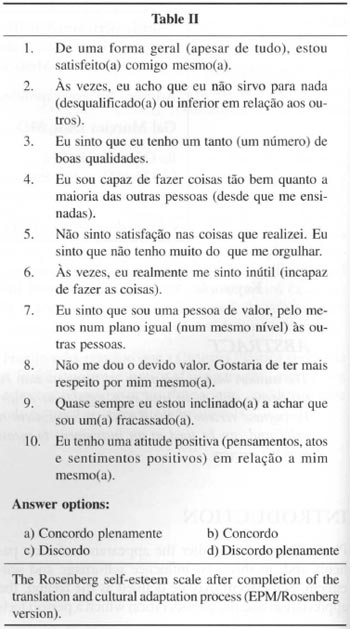
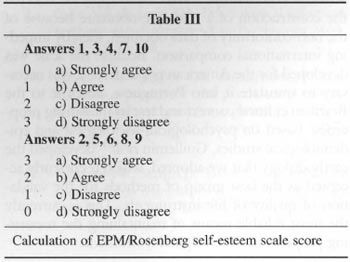
The original Rosenberg self-esteem scale in English and its version after translation and cultural adaptation (EPM/Rosenberg version) are shown in Tables I and II. Table III represents the score of the scale.
The reproducibility between distinct observers after statistical analysis showed a p-value, that is significance lower than 0.516. The reproducibility with the same observer at different times showed a p-value less than 0.5.
In the final regression model the following aspects were included: Emotional aspect, pain, vitality, general state of health and the functional capacity of the quality of life instrument - Short Form 36 and instrument SRQ-20 (Self Reporting Questionnaire).
After calculating the statistics, we were able to observe that instrument SRQ-20 contributed 56.98% to explaining the results obtained with the UNIFESP/EPM/Rosenberg self-esteem scale. The aspect 'general state of the patient' contributed with 19.40%, pain 47.8% and functional capacity 10.32%.
DISCUSSION
After systematic review of the literature to identify all the instruments available for measuring self-esteem directify or indirectly, the Rosenberg scale was chosen as being the one which most closely matched our objectives of being widely accepted in the international scientific community(4.6) and easy to apply. We rejected the construction of a new questionnaire because of the non-conformity of data obtained, thereby impeding international comparison. Because the scale was developed for the American population, it was necessary to translate it into Portuguese, adapt it to the Brazilian cultural context and test its measuring properties. Based on psychological, sociological and epidemiological studies, Guillemin et al(3) developed the methodology that we adopted, which is currently accepted as the best group of methods for the validation of quality of life instruments. This is currently the most reliable means of maintaining the measuring properties of the original instrument.
In the cultural equivalence evaluation or pre-test, we observed great difficulty on the part of the patients in expressing themselves.
The relevance evaluation showed that all the questions were considered applicable to the population studied such that there was no need to annul any of the original tests. This brings the Brazilian version closer to the original. Self-esteem probably has universal significance. During the pre-test we observed great difficulty of the patient in understanding the semantics of the questions. This required greater adjustments and more synonyms to clarify the questions. We argue that this is the result of the high levels of illiteracy, truancy and generally poor school performance in this environment.
Although the sentences may seem redundant (pleonastic), the idea behind the methodology is to use language in the cultural adaptation that can be understood even by a child. In accordance with the guidelines of the adopted methodology, we used short sentences and key words, avoiding the passive voice, pronouns and general terms. This made the scale much more reliable, avoiding the possibility that patients who did not understand the meaning of the phrase would opt for anyone of the alternatives, due to reluctance to ask for clarification.
Having completed the adaptation, we then proceeded to evaluate the reproducibility of the EPM/Rosenberg scale. Liang & Jette(7) reported that reproducibility between the same observer (intra-observer) at different times is important for self-reporting questionnaires, whereas reproducibility among different observers (inter-observer reproducibility) is important for the application of questionnaires through an interviewer. Jenkinson(8) considered that reproducibility is important for all instruments. The scale should have the same or very similar results in two or more applications with the same patient, considering that the patient's clinical state has not changed. The analysis of the scores obtained witil the application of the questionnaire showed high correlation indices between observations from the same researcher, as well as distinct observers.
The theoretical hypothesis that lays down the correlations for construction validity measurement, was based on studies in the literature which clearly show that many plastic surgery patients experience high levels of anxiety, depression and social isolation related to their complaint; during the post operative period these symptoms and self esteem improve(9-16).
In this way, we correlated the EPM/Rosenberg self esteem scale with the anxiety depression questiolnnaire (SRQ-20),the mental components of SF-36 (both translated and validated for the Portuguese language), as well as the numeric scales we developed.
Initially, we analyzed all the results of the dimensions and scales in descriptive form, examining these in terms of distribution, position measurements, dispersion and association. Latterly, an inferential analysis was carried out to establish the associations and effect of these items on the Rosenberg scale. The Pearson correlation is a parametric method, applicable to continuous or occasional variables and the Spearman correlation non-parametric, that is applicable to category variables. In carrying out the regression statistical method, we were able to analyze by what percentage each aspect contributed to self-esteem. We were able to verify that the order of importance for the Rosenberg scale is: the SF-36 General State dimension, SRQ-20, the dimensions Functional Capacity, Pain, Vitality and the SF-36 Emotional Aspect. The reproducibility and validity of the instrument were thus demonstrated, and the instrument is therefore appropriate for the use of the measurement of self-esteem.
A reliable instrument enabling the evaluation of an individual's self-esteem is of great importance. In surgical procedures where there will be alterations to bodily form, it is essential that the physician tries to discover the patient's aspirations and fantasies in respect of the results, and that mental health is evaluated. Great care must be taken with the patient's true complaint, because in many instances what the patient is looking for in the treatment is a solution to relationship conflicts. The most reliable and safest motives are those related to self-esteem and self-image. The hope that the surgery will cause a reaction in someone else is unreasonable and reflects illusions in relation to the treatment(9). The ability to guide these patients adequately comes with experience, surgical maturity and persistent observation(17).
The translation into Portuguese of the Rosenberg self-esteem scale and its adaptation to the cultural and socio-economic context of our population have made this instrument an important complementary tool for evaluating plastic surgery results or for other studies where the evaluation of self-esteem is necessary.
REFERENCES
1. Rosenberg M. Society and the adolescent self image. Princeton: Princetan University Press; 1965.
2. Goldwyn RM. The patient and the plastic surgeon. 2. ed. Bostan: Little, Brown; 1991. 359p.
3. Guillemin F, Bombardier C, Beaton D. Cross-culrural adaptation of the health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol, 1993; 46:1417-32.
4. Faria FS, Guthrie E, Bradbury E, Brain AN. Psy-chosocial outcome and patient satisfaction follow-ing breast reduction surgery. Br J Plast Surg. 1999; 52:448-52.
5. Shakespeare V & Cole RP. Measuring patient based outcomes in a plastic surgery service: breast reduction surgical patients. Br J Plast Surg. 1997; 50:242-8.
6. Ranzijn R, Keeves J, Luszcz M, Feather NT. The role of self perceived usefulness and competence in the self-esteem of elderly adults: Confirmatory factor analyses of the Bachman revision of Rosenberg's self-esteem scale. J Gerontol Psychol Sci. 1998; 53B:96-104.
7. Liang MH & Jette AM. Measuring functional ability in chronic arthritis. Arthritis Rheum. 1981; 24:80-5.
8. Jenkinson C, Coulter A, Wright L. Short form 36 (SF-36) health survey questionnaire: normative data for adults of working age. B M J. 1993; 306:1437-40.
9. Goin MK & Goin JM. Psychological effects of aesthetic facial surgery. Adv Psychosom Med. 1986; 15:84-108.
10. Meyer L & Ringber GA. Augmentation mamma-plasty - psychiatric and psychosocial characteristics and outcome in a group of swedish women. Scand J Plast Reconstr Surg. 1987; 21:199-208.
11. Kilmann PR, Sattler JI, Taylor J. The impact of augmentation manunaplasty: A follow-up study. Plast Reconstr Surg. 1987; 80:374-8.
12. Hong SM & Giannakopoulos E. The relationship of satisfaction with life to personality characteristics. J Psychol. 1994; 128:547-58.
13. Klassen A, J enkinson C, Fittzpatrick R, Goodacre T. Patient's health related quality of life before and after aesthetic surgery. Br J Plast Surg. 1996; 49:439-41.
14. Klassen A, Fittzpatrick R, Jenkinson C, Goodacre T. Should breast reduction surgery be rationed? A comparison of the health status of patients before and after treatment: postal questionnaire survey. Br Med J. 1996; 313:454-7.
15. Klassen A, Jenkinson C, Fittzpatrick R, Goodacre T. Measuring quality of life in cosmetic surgery patients with a condition-specific instrument: the Derriford Scale. Br J Plast Surg. 1998; 51:380-4.
16. Klassen A. Quality of life outcomes after cosmetic surgery. Plast Reconstr Surg. 1999; 104: 1209-10.
17. Baker TJ. Patient selection and psychological evaluation. Clinics in Plast Surg. 1978; 5:03-14.
I - Master of Science in Plastic Surgery (Federal University of São Paulo- Escola Paulista de Medicina, Brazil)
II - Master of Science in Clinical Epidemiology (McMaster University, Canada)
III - Titular and Head of the Division of Plastic Surgery at the Federal University of São Paulo- Escola Paulista de Medicina- Brazil
Sutdy performed at the Plastic Surgery Department of Universidade Federal de São Paulo - Escola Paulista de Medicina - São Paulo - Brazil
Address for correspondence:
Gal Moreira Dini, MD
R. Oscar Freire, 715
01426-000 - São Paulo - SP Brazil
e-mail: dr.gal@uol.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket