



Articles - Year 1997 - Volume 12 -
External Approach in Rhinoseptoplasty
Abordagem Externa nas Rinosseptoplastias
ABSTRACT
The authors address the issue of the external approach in rhinoseptoplasty, discuss its main features, indications, surgical technique and the controversies about the columellar scar. They believe that the direct vision ofthe nasal structures facilitates both diagnosis and treatment of the esthetic-functional deformities of the nose.
Keywords: Rhinoplasty, External Approach, Open Structure Rhinoplasty
RESUMO
Os autores apresentam os principais aspectos relacionados à abordagem externa nas rinosseptoplastias. Discutem as indicações do método, bem como a técnica cirúrgica aplicada, além da polêmica em relação à cicatriz columelar. Consideram que a visão direta das estruturas facilita o diagnóstico e tratamento das deformidades estético-funcionais nasais.
Palavras-chave: Rinoplastia, Abordagem Externa, Rinoplastia a Céu Aberto
Among all esthetic surgery, rhinoplasty is considered the most difficult one to perfonn, the highest stage in the acquisition of skills by the plastic surgeon. This is mainly due to the fact that most of the work is done almost "blindly", with a very limited view of the anatomical structures and it relies mainly on the tactile sensations rather than visual ones. Also, severe functional and esthetic problems may occur when the endonasal incisions are not sufficient for the precise diagnosis and proper treatment of the existing deformities.
Aware ofthese difficulties, in an attempt to overcome them, we have been perfonning the external approach to rhinoplasty.
According to the Sushruta Samhita (approx. 600 BC), external incisions for nasal repairs were already performed in India at that time(30). In 1920, Gillies described the "elephant trunk" incision as an approach for the treatment of the nose tip(1,30). In 1929 and 1931, Rethi(25) presented his classical transcollumelar incision. Sercer, in 1956(27), extended Rethi's exposure to work on the dorsum of the nose, call ing it "nasal decortication". In this same year, Hauberisser published a modification of Rethi's technique in wich the vestibular incision extended lateral and externally, contouring the asa(30). In 1966, Padovan(22,23) recommended the use of the same technique for treating the nasal septum, calling it "open sky rhinoplasty" for the first time.
Since then, there have been many papers defending this approach for different purposes. In Brasil, Ribeiro(26) had a paper on "open sky rhinoplasty" on the XXII Brasilian Congress of Plastic Surgery, in 1985, and, more recently, Sperly(31) has been defending the method, which he named "Exorhinoplasty".
Patient and Methods
The external approacb is indicated for those patients with sequelae from trauma and significant deviation of the nasal bridge and septum(5,6,12,16,17), proeminent, bulbous or bifid nasal tips (1,2,4,5,14,17), valvar disfunctions, septal perforations(20), negroid and leporino noses(4,7), congenital deformities (1,7,18), as a route for trans-septal sphenoidectomies (19,21), or in secondary rhinoplasti es (1,2,5,11,12,17).
Currently we have been using the external approach for all our cases ofrhinoplasty, both primary and secondary, with rewarding results, not recommend it only when the patient does not accept an external scar, in minor rhinoplasties or when there are scars that could affect the viability of the collumelar flap.
Anesthesia and local infiltration - Both general endotracheal or local anesthesia can be used to perfornl the method. The nose is infiltred with approximately 7-8 ml of a solution containing: 20 ml of 0,5% Marcaine without vasoconstrictor plus 20 ml of saline solution plus 0,5 ml of adrenaline 1/1000. We prefer marcainc due to the prolonged analgesia, giving extra comfort to the patient in the immediate post-operative period. We start infiltrating the dorsum downward, followed by the collumela, nasal spine and vestibulum. If necessary, a subpericondrial infiltration ofthe septum is done.Immediately before performing the lateral fractures we do the infiltrating of these areas.
External approach - A transverse medio-collumelar incision (Fig. I) associatcd to bilateral marginal alar incisions is the way to start this approach. The transverse medio-collumelar incision is broken by an inverted "V" wich prevents future retractions(17) (Fig. 2a).

Fig. 1 - Trans-operative view oftransverse media-collumelar incision. It must be broken by an inverted "V" in order to prevent future retractions in this area.
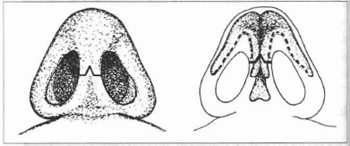
Fig. 2a) - Schematic representation af the transverse medio-collumelar incision. b) - The marginal incisions should be placed alongside the caudal edge ofthe lateral crura, domus and medial crura where they meet with the media-collumelar incision at right angles.
The marginal incisions should be placed alongside the caudal edge ofthe lateral crura, domus and medial crura where they meet at rightangles with the medio-collumelar incision on either side of the collumela (Fig. 2b). It is important to emphasize that the incision should be marginal to the caudal edge ofthe alar cartilages and not to the nostrils, avoiding thus retractions ofthe borders of the nostrils(1,5,17).
Through careful dissection, the elevation of the cutaneous flap of the medial crura is started, caring not to damage it. The dissection is continued upward over the lateral crura and the osteo-cartilagineous dorsum. If performed correctly (right above the pericondrium) the dissection plane is, for all practical purposes, avascular. Occasional bleeding can be controlled by bipolar coagulation.
This way, the structures of the dorsum and the tip of the nose are widely exposed (Fig. 3). This should be the moment to assess the different problems and review the surgical plane.

Fig. 3 - Trans-operative view of the wide exposition of the structures of the dorsum and the tip.
Treatment of the deformities of the dorsum - The treatment of the osteocartilaginous hump is performed under wide direct vision according to the surgeon's preference.
One can do it with rasps, scissors or chisel (17,32). Bony or cartilagineous grafts can be included and placed over the dorsum to correct depressions, assymetries or saddling.
Treatment of the deformities of the tip - The choice of treatment mcthod will depend on the defonnities found and on the surgical plan. The external approach allows a precise assessment ofsymmetry and harmony, as well as remodelling of the nose tip with the exclusion or inclusion of elements(3,4,10,13,18,24,28,29) with fixation or repositioning as needed.
Fractures - It is the only step in which the structures that are being treated are not visualized directly. The lateral fractures can be done both endonasally or externally depending on the surgeon's experience(8,17,34).
Treatment of the nasal septum deformities - This approach allows the execution of any correction procedure for septal deformities or deviations as well as harvesting septal samples to be used as grafts(6,16,17).
Starting by the upper approach, after lowering the dorsum, it is possible to perform a broad submucoperichondrial detachment ofthe entire septum, exposing existing deviations, fractures or spurs (Fig. 4).

Fig. 4 - The external approach allaws any correction procedure on the septum.
Closure and immobilization - The collumelar incision is meticulously closed with non-absorbable 6-0 sutures and the vestibular one with absorbable 5-0 sutures.
Immobilization is done with surgical tape and cast.
Nasal packing is used when procedures involving the septum are performed.
Discussion
The external approach for rhinoplasty has been the subject of a great deal of controversy, especially in regard to the columellar scar. We have observed, however, that if the technique is well performed and the suture of the columella is carefully done, the scar will become imperceptible with time. Less conspicuous than the ones from the classical and universally accepted perialar incisions.
In respect to the more pronounced edema ofthe nasal tip, it is our impression that it is related reather to an exaggerated tissue manipulation and prolonged surgery time than to the technique itself. There is no question that it is a technique that takes longer to perform. Would this be areal disadvantage compared to the obtained refinement? If we compare closed and open techniques, the difference in undermined areas is minimal, envolving a segment of approximately 0,5 cm2 from the coumella(16) (Fig. 5).

Fig. 5 - Comparing clased and open techniques, the difference in undermined areas is minimal (approx. 0,5 cm2).
We did not see necrosis of the columellar flap in any of the operated cases. The main cause of this complication is the elevation of this flap in a very superficial plane. With appropriate technique, carefully dissecting out the flap just over the pericondrium, the circulation is maintened. Ofcourse, in the secondary cases, extra-care should be taken, due to tissue fibrosis.

Fig. 6a - Preoperativefront view ofa patient with important rhinoseptal deviationfrom trauma.

Fig. 6b - Post-cperative front view after correction by extental approach and complete rhinoseptoplasty.

Fig. 6c - Preoperative perfil view of the same case.

Fig. 6d - Postoperative view after correction.

Fig. 7a - Preoperative front view ofa patient with sequelae ofprevious rhinoplasty. Notice misalignement of nasal pyramide and asymetric bulbous tip.

Fig. 7b - Post-operative view after correction through an open approach.

Fig. 7c - Basal view. Important asymetria is noticed.

Fig. 7d - Basal post-operative view ofthe result achieved. lnconspicous scar in the collumela.

Fig. 7e - Perfil preoperative view of the same case.

Fig. 7f- Post-operative view.

Fig. 8a - Preoperative aspect of a patient with discret dorsal hump. broad tip and septal deviation in zone 2.

Fig. 8b - Post-operative aspect after rhinoseptoplasty by external approach.

Fig. 8c - Perfil preoperative view of the same patient.

Fig. 8d - Post-operative view.
Conclusions
This approach, aside from the already mentioned indications and the irrefutable advantage of the direct vision, has brought also new perspectives for the teach· ing of rhinoplastyu6.(1,16,17,35), making all the steps of the procedure clearer to understand. On the other hand, it is not a technique for those with little experience or for "begginers". As reviewed, it facilitates the treatment of the nasal structures, but it does not warrant better results.
In order to achieve the proposed preoperative goals, an esthetic perception and knowledge of anatomy and surgical technique along with the surgical refmement of rhinoplasty are required.
References
1. ADAMSON PA. Open rhinoplasty. Otolaryngol CUn N Am 20: 837-52, 1987.
2 ANDERSON JR, JOHNSON CM Jr, ADAMSON PA. Open rhinoplasty: an assessment. Otolaryngol Head Neck Surg 90: 272-4, 1982.
3. BRENNAN HG. Domc splitting technique in rhinoplasty with overlay of lateral crura. Arch Otolaryngol 109: 586-92, 1983.
4. BRlANT TOR: Management of the nasal tip in the external approach rhinoplasty. J Otolaryngol 7: 18-23, 1978.
5. BURGESS LP, QUTLUGAN JJ, VAN SANT TE Jr: The external (combination) rhinoplasty approach for the problem nose. J Otolaryngol 14: 113-119,1985.
6. CONRAD K: Correction of the croocked noses by external rhinoplasty. J Otolaryngol 7:32-42, 1978.
7. ECKER HA. Adirect approach to the morc sevcrely deformed clcft lip nose. Plast Reconstr Surg 67: 369-374, 198 I.
8. FARRIOR RT: Thc osteotomy in rhinoplasty. Laryngoscope 88: 1449-59, 1978.
9. FENTON RS: Extcrnal scptorhinoplasty - Why the fuss? J Otolaryngol 7:3-5, 1978.
10. GOLDMAN IB: New tcchnique for corrective surgery of nasal tip. Arch Otolaryngol 70: 183213, 1963.
11. GOODMAN WS: The external approach to rhinoplasty. Can J Otolaryngol2: 207- 10,1973.
12. GOODMAN WS: Rcccnt advances in extcrnal rhinoplasty.J Otolaryngol 10: 433-9, 198 I.
13. GOODMAN WS: Septo-rhinoplasty: surgcry ofthe nasal tip by extcrnal rhinoplasty. J Laryngol Otol 94: 485-94, 1980.
14. GOODMAN WS, CHARLES DA: Tcchnique of extcrnal rhinoplasty.J Otolaryngol7: 13- I7, 1978.
15. GOODMAN WS, GILBERT RW: Thc anatomy of cxternal rhinoplasty. Otolaryngol Clin N Am 20: 641-52,1987.
16. GRUBER RP: Opcn rhinoplasty. Clin Plast Surg 15: 95-114,1988.
17. JOHNSON CM Jr & TORIUMI OM: Open Structure Rhinoplasty, Philadelphia, W.B. Sawlders, 1990.
18. KAMER FM, CHURUKlAN MM: Shield graft for the nasal tip. Arch Otolaryngol I 10:608-10, 1984.
19. KOLTAI PJ, GOLDSTEIN JC, PARNES SM: External rhinoplasty approach to trans-sphenoidal hypophysectomy. Arch Otolaryngol ( Stockh) 3:456-8, 1985.
20. KRIDEL RWJ-I. APPLING WD, WRIGHT WK: Septal perforation closure utilizing the external septorhinoplasty approach. Arch Otolaryngol (Stockh) 112: 168-72, 1986.
21. McCURDY JA, VANSANTTE, YIMDWS:Transseptal, trans-sphenoidal hypophysectomy via the external rhinoplasty approach J. Otolaryngol 7:29-31, 1978.
22. PADOVAN T. External approach in rhinoplasty (decortication).Symp 0 R L 3/4: 354-360, 1966.
23. PADOVAN IV: External approach in rhinoplasty (decortication). In CONLEY J & DICKINSON JT (Eds): Plastic and Reconstructive Surgery of the Face and Neck. New York, Grune& Stratton, 1972, p. 143-6.
24. PECK G C: The onlay graft for nasal tip projection. Plast Recoostr Surg. 71:27-39,1983.
25. RETHI A: Operation to shorten an excessively long nose. Rev Chir Plast 2:85, 1934.
26. RIBEIRO L: Rinoplastia a ceu aberto. In: Anais do XXII Congresso Brasileiro de Cirurgia Phistica. Porto Alegre, Aplub, 1985. p. 255-7.
27. SERCERA: Dekortication dernose.Chir Maxillofac Plast (Zagreb) I:49, 1958.
28. SHEEN J H: Aesthetic Rhinoplasty. ST Louis, CV Mosby Co, 1978.
29. SIMONS R L: Vertical dome division in rhinoplasty. Otolaryngol Clin N Am 20: 785-96, 1987.
30. SNELL GED: History of external rhynoplasty. J Otolaryngol7:6-8, 1978.
31. SPERLI A: Exo-rinoplastia. Rev Soc Bras Cir Plast 3:126-137,1988.
32. SULLIVAN M J & KRAUSE C J: Surgery of the bony and cartilaginous dorsum.Otolaryogol Clio N Am 20:825-35, 1987.
33. VOGT T : Tip rhinoplastic operations using a transverse collumelar incision. Aest Plast Surg 7: 13-19, 1983.
34. WEBSTER RC, DAVIDSON TM, SMITH R C: Curved lateral osteotomy for airway protection in rhinoplasty. Arch Otolaryngol 103: 454-8, 1977.
35. WRIGHT WK & DRIDEL RWH: External septorhinoplasty: a tool for teaching. Laryngoscope 91 :945, 1981.
I - Reconstructive Microsurgery and Plastic Surgery Service Santa Coso de Misericordia - Porto Alegre - RS - Brasil
ADDRESS FOR CORRESPONDENCE
24 de Outubro, 1681/606
CEP: 90510-003 Porto Alegre - RS - Brasil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket