



Review Article - Year 2021 - Volume 36 -
Importance of plastic surgery for women with mastectomies and the role of Brazilian Unified Health System: integrative review
Importância da cirurgia plástica para mulheres mastectomizadas e o papel do Sistema Único de Saúde: revisão integrativa
Brenda Lopes Brandão1 ; Ariel Caríssimo Barbosa Silva1; Ítalo Nacif Francisquini1; Mariana Machado Gouvêa1; Lúcia Meirelles Lobão1,*
; Ariel Caríssimo Barbosa Silva1; Ítalo Nacif Francisquini1; Mariana Machado Gouvêa1; Lúcia Meirelles Lobão1,*
ABSTRACT
Introduction: The benefits of performing breast reconstruction in mastectomized patients go far beyond aesthetics, contributing to a woman’s emotional health, selfesteem and sex life. Thus, this study aimed to address the relevance of performing plastic surgery in women with mastectomies in Brazil and highlight women’s rights within the Brazilian Unified Health System during the process.
Methods: For this, an integrative qualitative review was carried out through data collection on the SciELO, PubMed and LILACS platforms, in addition to a complementary search on Google Scholar. The articles included in the study were analyzed using the content method.
Results: In total, 21 articles were included, in which it was observed that women with mastectomies reported feelings of fear, shame, suffering, reduced sexuality and dissatisfaction. It was also observed that these feelings decreased after performing the cosmetic procedure.
Conclusion: Because the breasts represent a symbol of sensuality and female pride, it is extremely important that the Brazilian Unified Health System, as well as health professionals, are trained to welcome and resolve the patients’ doubts, ensuring that there is no negligence in the care and providing a decent treatment.
Keywords: Quality of life; Breast; Mammaplasty; Mastectomy; Sexuality.
RESUMO
Introdução: Os benefícios da realização de reconstrução mamária em pacientes mastectomizadas vão muito além da estética, contribuindo para a saúde emocional, autoestima e vida sexual da mulher. Dessa forma, o presente estudo teve como objetivo abordar a relevância da realização da cirurgia plástica em mulheres mastectomizadas no Brasil, bem como evidenciar os direitos da mulher, dentro do Sistema Único de Saúde, durante o processo.
Métodos: Para isso, foi realizada uma revisão integrativa de caráter qualitativo através da coleta de dados nas plataformas SciELO, PubMed e LILACS, além de uma pesquisa complementar no Google Acadêmico. Os artigos incluídos no estudo foram analisados pelo método de conteúdo.
Resultados: No total foram incluídos 21 artigos, nos quais observou-se que as mulheres mastectomizadas relatavam sentimentos de medo, vergonha, sofrimento, redução da sexualidade e insatisfação. Também foi observado que esses sentimentos diminuíram após a realização do procedimento estético.
Conclusão: Pelo fato de as mamas representarem um símbolo de sensualidade e orgulho feminino, é de extrema importância que o Sistema Único de Saúde, assim como os profissionais da saúde estejam capacitados para acolher e sanar as dúvidas das pacientes, garantindo que não haja negligência no cuidado e proporcionando um tratamento digno.
Palavras-chave: Qualidade de Vida; Mama; Mamoplastia; Mastectomia; Sexualidade.
INTRODUCTION
Breast cancer is the leading cause of death in women and the most incident globally, with a rate of 2.1 million new cases in 2018 and a percentage of 6.6% of total deaths from all types of diseases1. Considering the Brazilian incidence, after non-melanoma skin tumors, breast cancer is also the most common among women and the leading cause of death from cancer in the population, representing 16.5% of all deaths in 2014- 20202. In addition, 66,280 new cases were estimated for 2020, indicating an incidence of 43.74 cases per 100,000 women3.
Mastectomy, which removes one or two breasts through a surgical procedure, is performed when other treatments such as chemotherapy and radiotherapy are not effective, either because of the advanced stage of the tumor or its location. It is a milestone for women who need to undergo it due to the consequences in these women’s lives4, affecting their femininity and self-image, as the breast symbolizes the feminine sphere. These impacts affect the patient’s entire social life, from romantic relationships to professionals, as many women become ashamed of their own bodies. The surgery impacts not only aesthetic and physical, but also emotional, self-esteem, and sex life4.
Due to the large recurrence of late breast cancer diagnosis and the delay in accessing appointments, exams, biopsy and treatment, approximately 70% of diagnosed patients will need to have their breast removed5. According to Law 11,664/2008, the Brazilian Unified Health System (SUS - Sistema Único de Saúde - in portuguese) should ensure that all women, from 40 years of age, undergo mammography as a way of preventing and detecting neoplasia in its initial form since the incidence and mortality of this pathology tends to grow progressively in this age group6. However, it is observed that such examination is performed in the SUS, only in ages between 50 and 69, under the guidance of the Ministry of Health7. It is important to note that under the age of 40, there are fewer than 10 deaths per 100,000 women, while in the age group over 60 years, the risk is 10 times greater, thus showing the importance of early diagnosis3.
With the progression of cancer or even cancer treatment, some women may suffer some mutilations in the breast. As a way of restoring the esthetic standard, they are assured of immediate reconstructive plastic surgery8. The purpose of reconstructive plastic surgery is to reestablish the region’s regular anatomy and restore the self-esteem lost by some women during surgical treatment9. However, some problems can be observed in this process, such as cases of breast seroma, hematomas, necrosis, dehiscence, asymmetry and late venous thrombosis, which in some cases can lead to the patient’s death10. Other problems are intrinsically related to SUS support for patients, such as the lack of trained doctors and the structure to carry out the necessary procedures11.
SUS neglected the right to surgery reparatory until 1999 when it became their right. Despite this achievement, it was only in 2013 that the surgery had a deadline to be performed, which should occur soon after the mastectomy or as soon as the woman presents conditions for it8. Furthermore, in 2018, the right to surgery on both breasts was approved to ensure symmetry10. Thus, this article seeks to answer the major impacts caused by mastectomy in women in Brazil. Therefore, the study’s objective was to highlight the importance of performing plastic surgery for women with mastectomies and to elucidate the rights of these patients guaranteed by SUS in Brazil during the process.
METHODS
This study has a qualitative approach, with a descriptive and exploratory purpose, having used the bibliographic review of the integrative type as a data collection technique.
The Scientific Electronic Library Online (SciELO), PubMed and Latin American and Caribbean Health Sciences Literature (LILACS) platforms were used for data collection. Google Scholar platform was used for further research. The search was performed using the Boolean descriptors and operators: “plastic surgery” OR “reconstructive surgery” AND “neoplasm” OR “breast carcinoma in situ” OR “unilateral breast cancer” OR “mastectomy” AND “unique health system” OR “legislation.” In addition, the resolutions of the Legislation Portal (http://www4.planalto.gov.br/legislacao/)x addressed women’s rights concerning breast reconstruction surgery in the SUS were consulted.
As exclusion criteria, articles before 2010 that addressed non-mammary neoplasms, dissertations on surgical techniques and the diagnosis of tumors, as well as studies carried out in patients in countries other than Brazil, were disregarded. Studies that described the benefits reported by patients, or by the literature itself, of performing post-mastectomy breast reconstruction, in addition to articles that addressed the role of the SUS in reconstructive surgery in terms of management and epidemiology. There was no language restriction.
The results of the articles were evaluated through thematic content analysis. The themes most discussed by the patients were counted when reporting their perception during the mastectomy process and after reconstructive surgery. This type of analysis allows for quantifying the frequency of the most discussed topics, whose results were processed using Excel 2010 software.
RESULTS
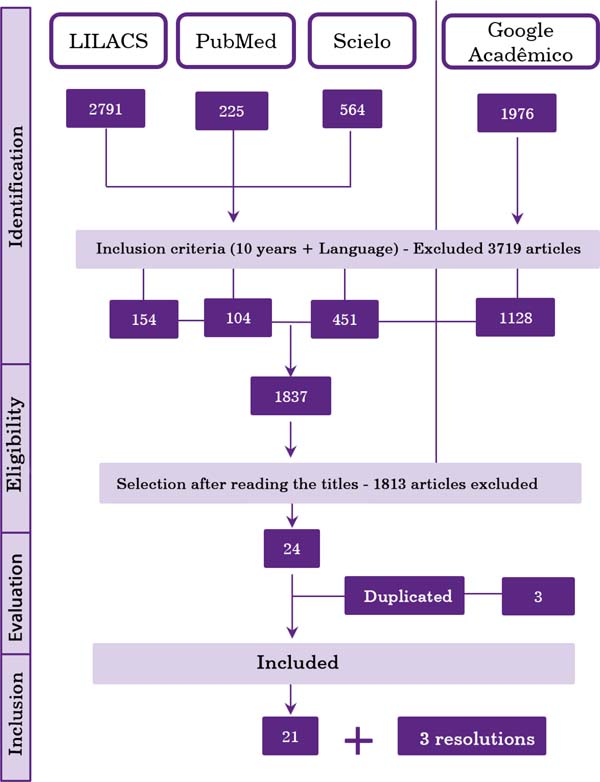
Five thousand five hundred fifty-six articles were found. After applying the filters (articles with full text on the platform, published in the last ten years) and an initial reading of the titles and abstracts, it resulted in 21 studies discussing the results. In addition, three resolutions were included, found on the Legislation Portal, as shown in Figure 1.
Of the selected articles, 16 addressed mainly the relationship between the performance of breast reconstructive surgery and the improvement of the woman’s quality of life, 2 about the feeling of post-mastectomy women, 1 addressed the comparison of the emotions of women who underwent or not breast reconstruction, and 2 discussed the role of SUS and public health about cosmetic surgery. In addition, the years of publication with the most selected studies were 2013, 2017 and 2019, with 4, 3 and 4 works, respectively. However, two articles from 2010, 2012, 2016 and 2020 were still selected; and one from 2015 and 2018, as shown in Chart 1.
From the resolutions found on women’s rights regarding breast reconstruction after mastectomy performed by SUS, Laws n° 9797, n° 12802 and n° 13.770 were selected, published respectively on May 6, 1999, April 24, 2013, and December 19, 2018.
Profile of women with mastectomies
The analysis of 19 articles about women with mastectomies showed that, in general, they have a profile between 41 and 60 years of age. In addition, most articles show a predominance of white participants with complete elementary education and Catholics (Chart 2).
Relationship between performing reconstructive surgery and the woman’s perception of her body
Among the 16 studies analyzed, which mostly addressed the relationship between performing breast repair surgery and improving the quality of life of women, 42.1% said that women felt anxiety, followed by feelings such as fear, depression and sadness (Table 1). In addition, some of the patients had decreased sexual desire, avoiding any intimate contact.
Among the included studies, an analysis of satisfaction with the breast, psychological and sexual well-being was presented by comparing 79 patients who underwent augmentation mammoplasty and 64 who did not. Of these, it was observed that patients undergoing reconstruction improved their self-image and feeling of overcoming cancer12. In addition, comparing before and after the reconstruction surgery, an increase in the patients’ physical and mental well-being was observed13. Therefore, it is generally possible to see that patients’ quality of life after breast reconstruction with breast implants is superior concerning the period before the procedure.
In the study by Carneiro et al. (2020)14, the assessment of these women’s feelings was also quite significant, with feelings of fear, shame, suffering, depression, loss, dissatisfaction being reported before the aesthetic procedure, which seem to decrease, or even disappear, after the surgery, as you can see in the patients’ statements:
“[...] I was very satisfied with the plastic surgery for breast reconstruction, it was as if I had been reborn, it’s another condition of life! I came back to life!” (p. 47746)
“[...] Knowing Ora of joy, right! Because I imagined that I would have that defect there, that we would look at, and see that thing without... right! Small right, but it is always defective, right. There was that emptiness, ugly thing there that I needed to do, so I resigned myself, but always nervous. It’s a lot of suffering. After the surgery to redo the breast, I dared to leave.” (p. 47746)
Chart 3 presents the main feelings brought by the articles of the patients after reconstructive surgery. In general, surgery is an option to reduce the negative emotions that are caused by the disease and the treatment, to improve self-esteem by replacing the “empty space” with a breast, facilitating clothing and seeing oneself body, changing the feeling of mutilation to a sense of renewed femininity and sensuality10. When comparing factors such as the age of the patients, it is possible to highlight that in physical aspects, younger women had better results, which indicates that it is associated with a lower presence of comorbidities in this age group, as well as in mental aspects, young women demonstrate a greater impact on self-esteem, which is expressed by the greater attachment to the body and following the standards of beauty imposed by society4.
The role of the SUS in the quality of life of women with mastectomies
According to Law No. 9,797, it was decreed as mandatory to carry out breast reconstructive plastic surgery by the network of units part of the SUS in mutilation cases after cancer treatment15. Some changes arose in Article 2nd when a new law was enacted, Law No. 12,802, adding two paragraphs. The 1st is to ensure that the reconstruction will be carried out when technical conditions exist at the same surgical time. The 2nd addresses the case impossibility of immediate reconstruction. The patient has the right to be referred for follow-up and will be guaranteed to undergo surgery immediately after reaching the necessary clinical conditions8.

| Author | Date | Title | Magazine | Type | Subject |
|---|---|---|---|---|---|
| Loyal et al.12 | 2010 | The body, cosmetic surgery and collective health: a case study. | Journal of Science and Public Health | Case study | Relationship of cosmetic surgery with collective health and health promotion. |
| Moura et al.13 | 2010 | The feelings of post-mastectomized women. | Anna Nery School of Nursing Magazine | Descriptive Qualitative Study | How women feel after mastectomy. |
| Cesnik and Santos14 | 2012 | Mastectomy and sexuality: an integrative review. | Psychology Journal: Reflection and Criticism | Integrative review | Impact of cancer and mastectomy on women's sexuality. |
| Majewski et al.15 | 2012 | Quality of life in women who underwent mastectomy compared to those who underwent conservative surgery: a literature review. | Journal of Science and Public Health | Literature review | Comparison between women who underwent a mastectomy and those who underwent conservative treatment. |
| Cosac et al.16 | 2013 | Breast reconstructions: a 10-year retrospective study. | Revista Brasileira de Cirurgia Plástica | Case study | Analysis of post-mastectomy breast reconstruction cases for breast cancer. |
| Colombo17 | 2013 | Assessment of the degree of satisfaction of patients undergoing breast reconstruction. | Revista Brasileira de Cirurgia Plástica | Retrospective study | Patient satisfaction after breast reconstruction. |
| Furlan et al.4 | 2013 | Quality of life and self-esteem of mastectomized patients undergoing or not breast reconstruction. | Revista Brasileira de Cirurgia Plástica | exploratory qualitative study | Quality of life of mastectomized patients undergoing or not breast reconstruction. |
| Gomes and Silva18 | 2013 | Self-esteem assessment of women undergoing breast cancer surgery. | Text and Context Nursing | Cross-sectional observational study | Self-esteem of women after cancer surgery. |
| Guimarães et al.19 | 2015 | Sexuality after augmentation mammoplasty. | Revista Brasileira de Cirurgia Plástica | Case study | Assess sexuality after augmentation mammoplasty. |
| Braga et al.9 | 2016 | Breast reconstruction process in mastectomized women. | Interdisciplinary Magazine | Literature review | Process involved from mastectomy to breast reconstruction. |
| Thais Rodrigues Guedes20 | 2016 | Body image of women undergoing treatment for breast cancer. | Masters dissertation | Self-esteem of cancer patients | |
| Alves, VL et al.21 | 2017 | Early assessment of the quality of life and self-esteem of mastectomized patients undergoing or not breast reconstruction. | Revista Brasileira de Cirurgia Plástica | Cross-sectional, comparative and analytical observational study | Make a comparison about the self-esteem of mastectomized patients undergoing reconstruction and those who did not undergo plastic surgery. |
| Martins, et al.22 | 2017 | Immediate breast reconstruction versus no post-mastectomy reconstruction: a study on quality of life, pain and functionality. | Physiotherapy and Research Journal | Cross-sectional descriptive study | Comparison between immediate breast reconstruction versus no post-mastectomy reconstruction. |
| Villar et al.23 | 2017 | Quality of life and anxiety in women with breast cancer before and after treatment. | Latin American Journal of Nursing | Prospective observational study | Before x after women being treated for breast cancer. |
| Casassola et al.24 | 2018 | Satisfaction with breast cancer surgery: Comparison between mastectomized patients with and without breast reconstruction. | International Exhibition of Teaching, Research and Extension | Qualitative study | Comparison between women with mastectomies who underwent plastic surgery and those who did not. |
| Archangel et al.25 | 2019 | Sexuality, depression and body image after breast reconstruction. | Clinics | Case study | Quality of life after breast reconstruction. |
| Cammarota et al.10 | 2019 | Quality of life and aesthetic result after mastectomy and breast reconstruction. | Revista Brasileira de Cirurgia Plástica | Case study | Quality of life of women undergoing breast reconstruction after cancer treatment. |
| Cosac et al.26 | 2019 | Breast reconstructions: a 16-year retrospective study. | Revista Brasileira de Cirurgia Plástica | Case study | Analysis of post-mastectomy breast reconstruction cases for breast cancer. |
| Volkmer et al.27 | 2019 | Breast reconstruction from the perspective of women undergoing mastectomy: a meta-ethnography. | Text and Context Nursing | Literature review | What do women undergoing mastectomy think about breast reconstruction? |
| Carneiro et al.28 | 2020 | Psychological repercussions of plastic surgery in mastectomized women. | Brazilian Journal of Development | Literature review | Quality of life of women who underwent mastectomies after plastic surgery. |
| Mollinar et al.11 | 2020 | Oncoplastic and reconstructive surgery of the breast: analysis of the patient's rights within the scope of the SUS. | Brazilian Journal of Development | Literature review | Rights of SUS patients for mastectomy and breast reconstruction. |

On December 19, 2018, Law No. 13.770 was created, in which three paragraphs were added to Article 1st, with the 1st paragraph to ensure that the breast reconstruction will be carried out during the surgical time of the mutilation when technical conditions exist, the paragraph 2nd in the event of the impossibility of immediate reconstruction, the patient will be referred for follow-up and will have the right to undergo surgery immediately after having the necessary clinical conditions, and paragraph 3rd guarantees that the procedures will symmetrize the contralateral breast and reconstruct the nipple-areola complex integrate reconstructive plastic surgery16.
DISCUSSION
The age group in the literature for mastectomized patients was a little lower than the Ministry of Health recommended starting performing breast cancer screening (50 to 69 years). It is possibly due to excessive exam requests resulting in unnecessary treatments and earlier exposure to ionizing radiation in women, implying more risks than benefits with advancing age17.
The most prevalent age can be explained by the epidemiology of the disease, being more common in women at the end of their childbearing lives. Menopause is the main risk factor for the disease, even more determinant than lifestyle habits and genetics11. As for family income, it is common for screening and the search for the health system to happen early in women who are part of a socioeconomic population with higher income, as this population has easier access to the private health system, health insurance, as well as greater access to information about the pathology and its clinical course18. In addition to the lower search for disease tracking, women with lower income, less education, and housewives are more likely to affect mental health, developing pathologies such as anxiety and eating disorders, making them even more prone to worse psychic progression after mastectomy.19
Breast cancer has a high prevalence and causes a great impact on women’s lives, affecting both their physical and psychological aspects20. Since the diagnosis is confirmed, the female identity starts to be questioned by the patient; after all, the breasts are considered a symbol of femininity and body beauty21. Therefore, breast reconstruction surgery has caused great satisfaction in post-mastectomized patients, as it is a good alternative to improve their self-esteem.
| Variables | Observed profile |
|---|---|
| Age group | More than 60% of women aged 41-60 years. |
| Color | It depends on the study's region, but it has a greater predominance in white women. |
| Education | More than 60% of women have education (in years) from 1 to 9 years, corresponding to complete primary education. |
| Family income | Family income is around 1 to 3 minimum wages. |
| Religion | It follows the regional pattern, tending to follow the national average, with more than half Catholic. |

| Feelings | % of articles |
|---|---|
| Anxiety | 42.1 |
| Fear | 31.5 |
| Depression | 21.0 |
| Sadness | 15.7 |
| Fault | 10.5 |
| Anguish | 10.5 |
| Insecurity | 10.5 |
| Conformism | 5.2 |
| Defensive posture | 5.2 |
| Shame | 5.2 |
| Worry | 5.2 |
| Inferiority | 5.2 |
| Feeling of worthlessness | 5.2 |

Thus, mastectomy can cause emotional and psychological distress, with significant improvements after breast reconstruction22. Still, it is important to emphasize that women have a higher rate of depression than men, which may highlight some biopsychosocial factors, such as educational and historical issues, and face losses as possible explanations for this indicator23.
The changes suffered in the body generate difficulty for women undergoing treatment for breast cancer, mainly due to prejudice and stigma associated with this disease21. This is related to the side effects of the treatment, the main ones being menopause and alteration in the production of sex hormones9. These hormonal changes can also cause problems such as vaginal dryness, dyspareunia, even vaginal atrophy, which brings another psychological shock to the woman, making healthy sexual intercourse a challenge24.
| Main changes after breast lift | |
|---|---|
| Sexuality | Sexuality increased significantly, in addition to the improvement in sexual satisfaction, showing no significant difference between patients who were or were not in a stable relationship. |
| Self-esteem | The improvement in self-esteem appears to be directly related to the patient's age, and the younger she is, the greater the result in her emotional function. |
| Psychosocial well-being | Patients are more self-confident, more accepting of their own bodies, strengthened in social environments and emotionally healthy. |
| Physical well-being | Few or almost no complaints of unbearable pain in the area of the breasts after surgery were observed, with only the increased sensitivity in the area standing out. |

A study carried out with 47 patients resulted in a great improvement in the sexuality of women undergoing mammoplasty surgery, showing an improvement in sexual satisfaction and arousal25. In addition to this, other studies have shown that there is a great benefit in performing breast reconstruction for post-mastectomized patients, reporting that patients who have not undergone this procedure have greater emotional fragility4.
Faced with so many negative impacts on the lives of women undergoing treatment for breast cancer, there is still certain negligence on the part of professionals about feminine emotionality, which is unacceptable since body and mind are in common26. Therefore, health professionals must support these patients, clarifying possible doubts, providing emotional support and managing the case in the best possible way to have the least likely impact on the woman’s life27.
Based on the review of the articles, it is possible to observe the importance of aesthetic procedures in the physical and psychological recovery of women who underwent a procedure as aggressive as mastectomy10. Surgical intervention through mastectomy can be performed with conservative methods such as quadrantectomy and nodulectomy or more radical methods that consist of total ablation of the breast and muscles. It is known that the emotionality of these women undergoing these procedures is affected throughout the treatment stage. However, it is mainly at the end of the treatment that difficulties in adaptation, restrictions and even negative repercussions in their sexual life arise20.
The complications of cosmetic surgery for breast repair and reconstruction are difficult to resolve, as they are inherent in any medical procedure, whether it is of low or high complexity. However, the surgeon must pay attention to risk factors such as obesity and smoking, as these contribute to complications and are essential to carry out a good preoperative period and strict follow-up after surgery28. The risk of performing this cosmetic surgery, being minimal, is offset by so many benefits provided to women, the main ones being an improvement in self-esteem and a feeling of greater femininity29.
Concerning the cost of surgery problems and others mentioned above, such as possible complications, it is difficult to propose solutions to establish a more beneficial scenario for both the system and the individual. A possible solution would be to improve the active screening of the target population since, in the early diagnosis, the number of procedures, mortality, and the cost of operations decreases significantly compared to the spontaneous search for patients11.
Thus, the right that women won, in 1999, to perform the procedure through the SUS, associated with the fact that this procedure is performed soon after the mastectomy, were important milestones in the fight for a better quality of life for women victims of breast cancer11. Despite this achievement, it was only in 2018 that it was possible to win the right to carry out bilateral repairs to maintain the symmetry of the breasts through an update to the 1999 law, ensuring a better aesthetic result and with good impacts on their quality of life11,30.
CONCLUSION
The present study showed that performing plastic surgery in women with mastectomies greatly impacts several psychological, sexual, affective, and social pillars of their lives. Despite having won several rights that address mastectomy and its consequences, there are still adversities that could be overcome with greater investment in secondary prevention, with more effective active screening.
This measure would be important to reduce treatment costs since the early stages of cancer require fewer interventions and less costly and less invasive procedures.
As for the psychological impacts of the consequences of the surgery and treatment, the preparation of professionals is essential to answer this patient’s doubts and welcome her concerns and concerns. Therefore, the naturalization of the suffering of these patients cannot occur, as it often leads to negligence in care. And, an important part of this care, humanization and dignification of women already takes place in the reconstruction surgery, which aims to return a physical symbol of female sensuality and pride.
REFERENCES
1. World Health Organization (WHO). Global Cancer Observatory (GCO). Estimated age-standardized mortality rates (world) in 2018, worldwide, female, all ages [Internet]. Lyon: Cancer Today/WHO; 2018; [acesso em 2020 Nov 29]. Disponível em: https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900&key=asr&sex=0&
2. Instituto Nacional de Câncer (INCA). Mortalidade proporcional não ajustada por todas as neoplasias, mulheres, Brasil, entre 2014 e 2018 [Internet]. Rio de Janeiro: INCA; 2018; [acesso em 2020 Nov 29]. Disponível em: https://mortalidade.inca.gov.br/MortalidadeWeb/pages/Modelo01/consultar.xhtml#panelResultado
3. Instituto Nacional de Câncer (INCA). Estimativa 2020: incidência de câncer no Brasil [Internet]. Rio de Janeiro: INCA; 2020; [acesso em 2020 Nov 29]. Disponível em: https://www.inca.gov.br/publicacoes/livros/estimativa-2020-incidencia-de-cancer-no-brasil
4. Furlan VLA, Neto MS, Abla LEF, Oliveira CJR, Lima AC, Ruiz BFO, et al. Qualidade de vida e autoestima de pacientes mastectomizadas submetidas ou não a reconstrução de mama. Rev Bras Cir Plást. 2013 Jun;28(2): 264-9.
5. Correio Brasiliense (BR). Demora no diagnóstico de câncer leva à mastectomia em 70% dos casos [Internet]. Brasília (DF): Correio Brasiliense; 2018; [acesso em 2020 Nov 29]. Disponível em: https://www.correiobraziliense.com.br/app/noticia/ciencia-e-saude/2018/05/06/interna_ciencia_saude,678759/demora-no-diagnostico-de-cancer-leva-a-mastectomia-em-70-dos-casos.shtml
6. Lei no 11.664, de 29 de abril de 2008 (BR). Dispõe sobre a efetivação de ações de saúde que assegurem a prevenção, a detecção, o tratamento e o seguimento dos cânceres do colo uterino e de mama, no âmbito do Sistema Único de Saúde - SUS. Diário Oficial da União, Brasília (DF), 29 abr 2008; Seção 1: 1.
7. Federação Brasileira de Instituições Filantrópicas de Apoio à Saúde da Mama (FEMAMA). O câncer de mama em números [Internet]. Porto Alegre: FEMAMA; 2019; [acesso em 2020 Nov 29]. Disponível em: https://www.femama.org.br/site/br/noticia/o-cancer-de-mama-em-numeros
8. Lei no 12.802, de 24 de abril de 2013 (BR). Altera a Lei nº 9.797, de 6 de maio de 1999, que “dispõe sobre a obrigatoriedade da cirurgia plástica reparadora da mama pela rede de unidades integrantes do Sistema Único de Saúde - SUS nos casos de mutilação decorrentes de tratamento de câncer”, para dispor sobre o momento da reconstrução mamária. Diário Oficial da União, Brasília (DF), 24 abr 2013.
9. Braga AKG, Santos TLC, Magalhães MAV. Processo de reconstrução mamária em mulheres mastectomizadas. Rev Interd. 2016;9(1):216-23.
10. Cammarota MC, Campos AC, Faria CADC, Santos GC, Barcelos LDP, Dias RCS, et al. Qualidade de vida e resultado estético após mastectomia e reconstrução mamária. Rev Bras Cir Plást. 2019;34(1):45-57.
11. Mollinar ABP, Pereira IPC, Araújo JSF, Smith JSR, Guerra MCA, Real Junior MMF, et al. Cirurgia oncoplástica e reconstrutiva da mama: análise acerca dos direitos do paciente no âmbito do SUS. Braz J Develop. 2020;6(8):54485-503.
12. Leal VCLV, Catrib AMF, Amorim RF, Montagner MA . O corpo, a cirurgia estética e a Saúde Coletiva: um estudo de caso. Ciência & Saúde Coletiva. 2010; 15 (1): 77-86.
13. Moura FMJSP, Silva MG, Oliveira SC, Moura LJSP. Os sentimentos das mulheres pós-mastectomizadas. Esc Anna Nery. 2010; 14(3): 477-84.
14. Cesnik VM, Santos MA. Mastectomia e sexualidade: uma revisão integrativa. Psicologia: Reflexões e Crítica. 2012; 25(2): 339-49.
15. Majewski JM, Lopes ADF, Davoglio T, Leite JCDC. Qualidade de vida em mulheres submetidas à mastectomia comparada com aquelas que se submeteram à cirurgia conservadora: uma revisão de literatura. Ciência & Saúde Coletiva. 2012; 17(3): 707-16.
16. Cosac OM, Filho JPPC, Barros APGSH, Borgatto MS, Esteves BP, Curado DMC, et al. Reconstruções mamárias: estudo retrospectivo de 10 anos. Rev Bras Cir Plást. 2013;28(1):59-64.
17. Colombo FG. Avaliação do grau de satisfação de pacientes submetidas a reconstrução mamária. Rev Bras Cir Plast. 2013; 28(3): 355-60.
18. Gomes NS, Silva SR. Avaliação da autoestima de mulheres submetidas à cirurgia oncológica mamária. Texto Contexto Enferm. 2013; 22(2): 509-16.
19. Guimarães PAMP, Neto MS, Abla LEF, Veiga DF, Lage FC, Ferreira LM. Sexualidade após mamoplastia de aumento. Rev Bras Cir Plast. 2015; 30(4): 552-559.
20. Guedes TSR. Imagem Corporal de Mulheres Submetidas Ao Tratamento Do Câncer De Mama. Natal. Tese [Mestrado em Saúde Coletiva] - Universidade Federal do Rio Grande do Norte; 2016
21. Alves VL, Sabino Neto M, Abla LEF, Oliveira CJR, Ferreira LM. Avaliação precoce da qualidade de vida e autoestima de pacientes mastectomizadas submetidas ou não à reconstrução mamária. Revista Brasileira de Cirurgia Plástica. 2017;32(2):208-17
22. Martins TNDO, Santos LFD, Petter GDN, Ethur JNDS, Braz MM, Pivetta HMF. Reconstrução mamária imediata versus não reconstrução pós-mastectomia: estudo sobre qualidade de vida, dor e funcionalidade. Fisioter. Pesqui. 2017; 24(4): 412-19.
23. Villar RR, Fernandez SP, Garea CC, Pillado MTS, Barreiro VB, Martin CG. Qualidade de vida e ansiedade em mulheres com câncer de mama antes e depois do tratamento. Rev Latino-Am Emfermagem. 2017; 25: e2958.
24. Casassola GM, Stallbaum JH, Pivetta HMF. Satisfação com cirurgia oncológica da mama: Comparação entre pacientes mastectomizadas com e sem reconstrução mamária. SIEPE [Internet]. 14º de fevereiro de 2020 [citado 20º de novembro de 2020];10(3). Disponível em: https://periodicos.unipampa.edu.br/index.php/SIEPE/article/view/87256
25. Archangelo SDCV, Neto MS, Veiga DF, Garcia EB, Ferreira LM. Sexuality, depression and body image after breast reconstruction. Clinics. 2019; 74:e883.
26. Cosac OM, Campos AC, Dias RCS, Costa RSC, Da-Silva SV, Damasio AA, et al. Reconstrução mamária: estudo retrospectivo de 16 anos. Rev Bras Cir Plast. 2019; 34(2): 210-7.
27. Volkmer C, Santos EKA, Erdmann AL Sperandio FR, Backes MTS, Honório GTS. Reconstrução mamária sob a ótica de mulheres submetidas à mastectomia: uma metaetnografia. Texto & Contexto Enfermagem. 2019; 28: e20160442.
28. Carneiro MSF, Pinheiro CPO, Feitosa FVV, Soares MN, Rabelo IV, Lebre P, et al. Repercussões psicológicas da cirurgia plástica em mulheres mastectomizadas. Braz J of Develop. 2020; 6(7): 47743-51.
29. Ng SK, Hare RM, Kuang RJ, Smith KM, Brown BJ, Hunter-Smith DJ. Breast Reconstruction Post Mastectomy: Patient Satisfaction and Decision Making. Ann Plast Surg. 2016; 76(6): 640-4.
30. Zhong T, Temple-Oberle C, Hofer S, Beber B, Semple J, Brown M, et al.; MCCAT Study Group. The Multi Centre Canadian Acellular Dermal Matrix Trial (MCCAT): study protocol for a randomized controlled trial in implant-based breast reconstruction. Trials 2013, 14: 356.
31. Brasil. Lei n. 9.797, de 06 de maio de 1999. Dispõe sobre a obrigatoriedade da cirurgia plástica reparadora da mama pela rede de unidades integrantes do Sistema Único de Saúde - SUS nos casos de mutilação decorrentes de tratamento de câncer. Diário Oficial da União. 06 mai 1999.
32. Brasil. Lei n. 13.770, de 19 de dezembro de 2018. Altera as Leis n º 9.656, de 3 de junho de 1998, e 9.797, de 6 de maio de 1999, para dispor sobre a cirurgia plástica reconstrutiva da mama em casos de mutilação decorrente de tratamento de câncer. Diário Oficial da União. 19 dez 2018.
33. Instituto Nacional de Câncer (INCA). Câncer de mama: vamos falar sobre isso?[site]. Rio de Janeiro: INCA; 2019 [acesso em 29 nov 2020]. Disponível em: https://www.inca.gov.br/campanhas/outubro-rosa/2015/cancer-de-mama-vamos-falar-sobre-isso
34. Crippa CG, Hallal ALC, Dellagiustina AR, Traebert EE, Gondin G, Pereira C. Perfil clínico e epidemiológico do câncer de mama em mulheres jovens. Arquivos Catarinenses de Medicina. 2003; 32(3): 50-8.
35. Santos LS, Diniz, GRS. Saúde mental de mulheres donas de casa: um olhar feminista-fenomenológico-existencial. Psicologia Clínica, 2018, 30(1): 37-59.
36. Correia KML, Borloti E. Mulher e Depressão: Uma Análise Comportamental-Contextual. Acta comport., 2011; 19(3): 359-73.
37. Oliveira JO, Peruch MH, Gonçalves S, Haas P. Padrão hormonal feminino: menopausa e terapia de reposição. Revista Brasileira de Análises Clínicas, 2016; 48(3): 198-210.
38. Brasil. Parecer técnico Nº 23/GEAS/GGRAS/DIPRO/2018. Cobertura: procedimentos diversos - mama e sistema linfático (mastectomia/ mastoplastia). Agência Nacional de Saúde Suplementar. 2018.
1. Dynamic College of Vale Do Piranga, Ponte Nova,
MG, Brazil.
BLB Analysis and/or data interpretation, Conceptualization, Data Curation, Investigation, Writing - Original Draft Preparation, Writing - Review & Editing.
ACBS Analysis and/or data interpretation, Conceptualization, Data Curation, Investigation, Writing - Original Draft Preparation, Writing - Review & Editing.
INF Analysis and/or data interpretation, Conceptualization, Data Curation, Investigation, Writing - Original Draft Preparation, Writing - Review & Editing.
MMG Analysis and/or data interpretation, Conceptualization, Data Curation, Investigation, Writing - Original Draft Preparation, Writing - Review & Editing.
LML Analysis and/or data interpretation, Conception and design study, Final manuscript approval, Supervision, Writing - Review & Editing.
Corresponding author: Lúcia Meirelles Lobão, Rua G, nº 205, Paraíso, Ponte Nova, MG, Brasil, Zip Code 35430-302, E-mail: lucia.fadip@gmail.com
Article received: April 09, 2021.
Article accepted: July 14, 2021.
Conflicts of interest: none.
Institution: Dynamic Faculty of Vale do Piranga, Ponte Nova, MG, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket