



Original Article - Year 2021 - Volume 36 -
Masculinizing mastectomy for male transsexual's gender reassignment
Mastectomia masculinizadora para redesignação de gênero de transexuais masculinos
Bruno Pires Do Amaral Marques1,*
ABSTRACT
Introduction: Masculinizing mastectomy is generally the first, most important and often the only surgical procedure for gender reassignment in male transsexuals. The objective is to describe and systematize the steps of the technique used by the author of the double-incision mastectomy associated with a free graft from the nipple-areola complex.
Methods: Retrospective review of 26 patients who underwent masculinizing mastectomies (total of 52 breasts), performed using the technique used by the author, between November 2013 and January 2018.
Results: 84.6% of patients had surgery with a final horizontal scar in the inframammary fold, and 15.4% evolved with a final inverted “T” scar. The rate of major complications was 3.8%. There was one reoperation (3.8%) in the follow-up period. Mean breast weight was 1,136 grams, mean age was 27 years and nine months, mean body mass index was 26.6 kg/m2, and 73% of patients received male hormone therapy before surgery.
Conclusion: Mastectomy is a safe procedure, with good reproducibility and brings satisfactory aesthetic results.
Keywords: Mammoplasty; Transsexualism; Sex reassignment surgery; Subcutaneous mastectomy; Gynecomastia.
RESUMO
Introdução: A mastectomia masculinizadora é geralmente o primeiro, o mais importante e muitas vezes o único procedimento cirúrgico na readequação de gênero em transexuais masculinos. O objetivo é descrever e sistematizar os passos da técnica utilizada pelo autor da mastectomia com dupla incisão associado ao enxerto livre de complexo areolopapilar.
Métodos: Revisão retrospectiva de 26 pacientes submetidos a mastectomias masculinizadoras (total de 52 mamas), realizadas pela técnica utilizada pelo autor, entre novembro de 2013 e janeiro de 2018.
Resultados: 84,6% dos pacientes sofreram a cirurgia com cicatriz final horizontal no sulco inframamário e 15,4% evoluíram com cicatriz final em “T” invertido. A taxa de complicações maiores foi de 3,8%. Houve uma reoperação (3,8%) no período de acompanhamento. O peso médio das mamas foi de 1.136 gramas, a idade média de 27 anos e 9 meses, índice de massa corporal médio de 26,6kg/m2 e 73% dos pacientes receberam terapia com hormônio masculino previamente à cirurgia.
Conclusão: A mastectomia masculinizadora é um procedimento seguro, com boa reprodutibilidade e traz resultados estéticos satisfatórios.
Palavras-chave: Mamoplastia; Transexualismo; Cirurgia de readequação sexual; Mastectomia subcutânea; Ginecomastia.
INTRODUCTION
The breasts are probably the greatest symbol of femininity in the human race and cause great discomfort to the social life of male transsexuals, who were born in the female gender and identify themselves as the opposite gender, which we conventionally diagnose as dysphoria1,2. The incidence of transsexualism varies greatly depending on the sources, most ranging between 0.5% and 1.5%1,3.
With the dissemination of information among the patients themselves through the internet and social media, there has been greater awareness of the topic, as well as the demand for psychotherapy, hormone therapy and surgical treatments, carried out by various professionals for social and psychological guidance, masculinization of the characteristics primary and secondary sexual: plastic surgeons, dermatologists, endocrinologists, gynecologists, urologists, breast cancer specialists, psychologists, social workers, among others1.
The objectives of this surgical procedure are: to remove breast tissue and excess skin, reduce and correctly reposition the CAP, try to minimize loss of sensation, flatten the inframammary fold, minimize scars on the chest wall and create an aesthetically pleasing male chest contour, preferably in a single surgical time2,3.
OBJECTIVES
This paper presents the author’s experience with a technique of masculinizing mastectomy (MM) performed in male transsexual patients (female to male), called double incision associated with a free graft of papillary areolar complex (DIEL-CAP).
METHODS
Casuistry
Between November 2013 and January 2018, 26 patients from his private clinic in Sorocaba/SP. were submitted to masculinizing mastectomies (a total of 52 breasts), performed by the technique proposed by the author.
Six months was the minimum follow-up time to be included in this work.
Surgical procedure
The maximum hospital stay was thirty hours. All masculinizing mastectomies were performed under general anesthesia.
1. Preoperative markings are performed with the patient’s trunk around sixty degrees of inclination, starting with an inferior horizontal line along the inframammary fold (Figure 1) and the midclavicular line;
2. Next, the upper horizontal incision line is drawn on the skin above the areola, evaluated using the pinch test. When the breast does not have enough skin leftover for the complete descent of the upper flap, the marking of this upper line is performed during the surgical procedure, which may eventually evolve with a final inverted “T” scar, in smaller breasts and with less flaccidity;


3. The surgical procedure is performed with the patient in horizontal dorsal decubitus with open arms;
4. The operation begins with the collection of a full-thickness NAC graft with a diameter of 2.5 cm, from the central region of the breast areola, with a scalpel blade (Figure 2);


5. The incision begins in the inframammary fold and, later, in the upper line, forming a final elliptical incision, whose surgical piece will be removed in monobloc (Figure 3). When there is no skin leftover for the descent of the superior flap, the detachment of the mammary gland is preceded by the superior incision of the ellipse in monobloc;
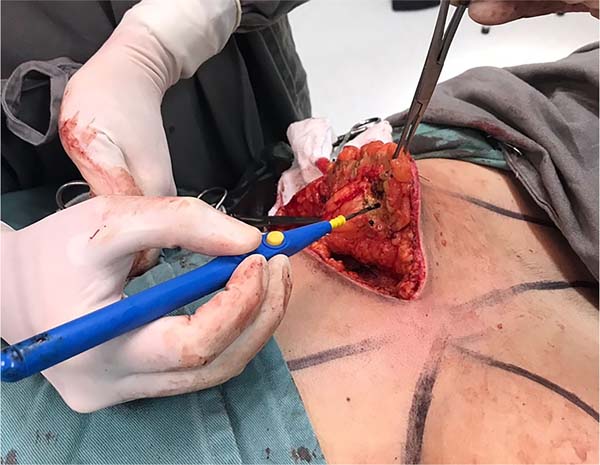
6. Afterwards, a detachment above the muscular plane is complemented in the cranial direction. When the breast tissues are released (Figure 4), the transition between the subcutaneous and glandular cell tissues is superficially incised, maintaining the final skin thickness around 1.5 to 2.5 cm (Figure 5), depending on the thickness of the adipose panicle. It is extremely important to preserve the adequate thickness of the subcutaneous fat during the entire detachment and resection of the glandular tissue (Figure 6). A tubular vacuum drain is introduced on each side of the hemithorax;







7. The superior and inferior flaps are sutured in three planes (Figure 7);
8. The new position of the NAC is preferably marked 1.0 to 2.0 cm lateral to the intersection of the midclavicular line and the original inframammary fold. The vertical height is marked approximately 2.5 cm above the inframammary suture line. Decortication is performed in the graft recipient area;
9. The NAC is thinned with scissors, and the suture is made with twelve simple mononylon stitches, like the hours of a clock, being interspersed with longer threads to fix Brown’s dressing (Figure 8);
10. Medium compression dressing with a cotton swab and microporous tape covers the entire chest. Compressive mesh or vest is not recommended to prevent skin flap ischemia.




Post-operative care
Outpatient return is performed between three and seven days after the surgical procedure to remove the drains, assess the scar and redress. A second return visit takes place one week after the first and the third one around twenty-one days after surgery to remove the graft stitches from the NAC. At this point, the usual activities such as housework and driving are released. After three months, intense physical activities are allowed.
RESULTS
The mean age of patients was 27 years and nine months (age range between 18 and 47 years). The weights of the patients were between 48 and 133kg (mean 73kg), height varied between 1.59m and 1.80m (mean 1.66m), and the mean body mass index (BMI) was 26.9 (between 17.8 and 39.1). Nineteen patients (73%) had a history of receiving testosterone hormone therapy before the operation. This hormone was discontinued three weeks before the surgical intervention and resumed three weeks later, according to Lo Russo and Innocenti (2017)2. In addition, every patient underwent a psychological evaluation that allowed the diagnosis of “female to male” (FTM) transsexualism and was documented through a psychological report, as well as an evaluation with an endocrinologist and social worker for a minimum period of 2 years, which was the legal requirement in effect at the time of this work.
Liposuction was not associated with these surgical procedures. The rate of major complications was 3.8%, and one patient had small suture dehiscence of 0.5x3.0cm, which healed by the second intention. Minor complications were: seroma (19.2%) and hematoma (7.7%), punctured and emptied in the office without needing a new surgical approach. Scarring disorders were found as follows: keloid in 15.4%, hypertrophic scar in 3.8% and scarring in 3.8%. This patient with scarring was the only one who underwent a new surgical approach (3.8%), where fat grafting was performed in the inframammary fold scar.
Other local complications were not found, such as large dehiscence, skin necrosis, total loss of the NAC graft, infection or evident asymmetries, and systemic: deep vein thrombosis, pulmonary thromboembolism, fat embolism or death. Small dyschromia in NACs was seen in some cases, common in this surgical procedure2, but there was no desire for a new surgical approach or tattoo for dermal pigmentation for them.
The total weight of the breasts ranged between 284 and 3,155 grams (average of 1,136), with the weight of the right breasts ranging between 140 and 1,585 grams (average of 557) and of the left ones between 144 and 1,570 grams (average of 578). All breasts were sent for anatomopathological diagnosis, which showed the absence of malignancy in all surgical specimens.
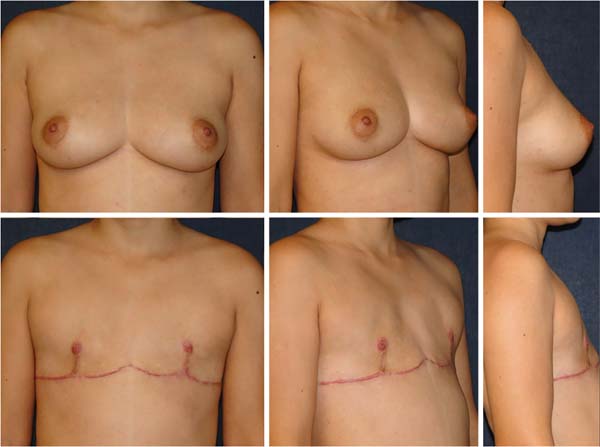
The final scar evolved in an inverted “T” in four cases (15.4%) in breasts of moderate volume and flaccidity. All surgical procedures were performed separately, without association with other combined surgeries. No breast had been previously operated on for reduction mammaplasty or mastopexy. None of the patients in the sample had undergone transgenitalization before MM, as well as oophoretomy (Figure 9-10).
DISCUSSION
Male transsexualism (or female to male, “female to male” - FTM) is a gender identity disorder (dysphoria). These individuals believe that they were raised in the body of the wrong gender, suffer from persistent psychological discomfort related to their anatomical gender and wish to live and be permanently accepted in the social role of the male gender1,2.



The treatment of gender dysphoria consists of a combination of different approaches such as hormonal therapy, surgical therapy and psychotherapy1,2. Due to the desire to change their anatomical sexual characteristics to those of the opposite sex, MM is generally the first, the most important and often the only surgical procedure in gender readjustment in male transsexuals, especially those with large breasts2,4 .5.
Regarding the current legal bases for transsexual surgeries, Resolution No. 2265, of September 20, 2019, of the Federal Council of Medicine, corroborated by publication in the Federal Official Gazette on 01/09/2020 (edition 6, section 1, page 96), defines the minimum age of 18 years for sexual reassignment breast surgeries, such as simple bilateral mastectomy (masculinizing) and 16 years for hormone therapy, as well as one year of minimum psychiatric follow-up. During this work, the legal basis was the CFM Resolution 1955/2010, which required 2 years of prior follow-up with an endocrinologist, psychologist and social worker, in addition to releasing hormone therapy at 18 and surgical procedures at 21 years of age. The four patients in this study aged 18 and 21 were operated on with court orders before surgery.
An ultrasound examination of the breasts was performed to assess the presence of glandular tissue and exclude any pathological tumors in all cases. Patients with an indication (over 40 years old with no family history and 35 years old with a positive family history of breast cancer) underwent mammography as a preoperative diagnostic complement.
Gynecomastia6,7 or mastectomy techniques for breast disease are commonly used in female patients. Still, subcutaneous mastectomy in FTM transsexuals is more difficult than the two procedures because these individuals have considerably larger breast volume, a greater degree of flaccidity and lower skin elasticity8. Continuous breast compression with elastic bands makes the quality of the skin and breast parenchyma worse4,6,8.
The first surgical techniques for MM had unsightly scars along the chest9,10. Currently, some authors such as Lo Russo and Innocenti (2017)2, Agarwal et al. (2017)5 and Knox et al. (2017)11 indicate to guide the position of the horizontal scar based on the lower edge of the pectoralis major muscle, especially on its lateral portion, in an ascending curve and not exactly on the original inframammary fold, so that it becomes more imperceptible.
The DIEL-CAP MM is used for most cases, in breasts of moderate to large volume and moderate to large ptosis, by most authors in the literature2-6,8,12.
Small breasts with little skin flaccidity were not part of this study. The periareolar technique is indicated, as described by Davidson (1979)7, Colic and Colic (2000)13, McEvenue et al. (2017)3 in one surgical time or Takayagi and Nakagawa (2006)14 in two surgical times, to minimize the resulting scar in the NAC, or transareolar according to Hage and Bloem (1995)15.
The advantages of the surgical technique described in this author’s work (DIEL-CAP) are the creation of a good field of view for dissection, exeresis of the breast parenchyma and hemostasis, allowing an adequate reduction of the NAC and skin excess, in addition to the absence of possible bulging due to excess volume with an inferior pedicle areolate. The disadvantages of the technique are a long inframammary scar and deformities in the projection, and decreased sensitivity of the breast papillae2.
The upper and lower flaps are adjusted so that the edges are as comfortable as possible, given that the length of the upper flap tends to be longer than the lower one. In cases where the breasts have large volumes, the right and left suture lines can be connected in the median region, forming a “W”-shaped scar, but this should be avoided when possible due to the possibility of keloid formation in the presternal region.
Wolter et al. (2015)8 describe other surgical techniques for treatment, depending on breast volume, summarizing the previous classification by Monstrey et al. (2008)4:
1) Small breasts, with good elasticity and without ptosis: semicircular periareolar subcutaneous mastectomy associated with liposuction;
2) Small breasts, moderate elasticity and grade I ptosis: periareolar concentric mastopexy associated with liposuction;
3) Medium breasts, moderate to poor elasticity and grade II ptosis: mammoplasty with an inferior pedicle areolate;
4) Large breasts, poor elasticity and grade III ptosis: MM DIEL-CAP.
The technique in group 3 above causes lower patient satisfaction and a higher rate of irregularities and reoperations8.
Another surgical option for Wolter classification 3 cases is described by Conte et al. (2019)7, with a NAC island skin flap, but tends to leave the breast with potential excess parenchyma.
McEvenue et al. (2017)3 published the study with the largest series of this surgical procedure in the literature (679 patients over 15 years). They simplified the surgical approach based on the classification into two single groups:
1) Subcutaneous mastectomy with a semicircular periareolar incision associated with liposuction in a patient with grade 0 or 1 ptosis with good skin elasticity (called “keyhole” technique);
2) Double-incision mastectomy associated with NAC-free graft in all other breasts.
Resende (2007)17 describes a technique to treat gynecomastia usually applied to male transsexuals. Still, the scar tends to be noticeable and placed outside the inframammary fold, where the lower chest contour tends to have less horizontal tension. Monstrey et al. (2008)4 also use this technique in some cases.
An important detail refers to the free NAC graft, similar to Thorek’s technique (1946)18. The graft donor area can be: 1 - areola margin; 2 - the center of the areola with the papilla; or 3 - the combination of both, with the central papilla around 0.5 to 1.0 cm in diameter and areolar diameter of 2.5 cm19. The author’s preference is for option 2, with satisfactory results. To improve the contour, tattooing is indicated for dermal pigmentation after six months. Still, no patient did it, as they were satisfied with the result, based on the author’s subjective experience, according to their reports in subsequent visits to the office. However, no questionnaire on satisfaction has been filled in by the patient, such as those performed by Wolter et al. (2015)8 or Nelson et al. (2009)12, or evaluation of the quality of the result evaluated by a surgeon and patient, such as Antoszewski et al. (2012)21.
A crucial point of this surgical procedure is the final horizontal position of the NAC graft in the chest. Normally, its position tends to be more pleasant when it is located around one to two centimeters lateral to the intersection between the original midclavicular line and the final horizontal scar in the inframammary fold. Thus, the author of this work simplifies other marking techniques based on the lateral border of the pectoralis major muscle, on the junction of body lines or a table concerning the chest circumference, which are more difficult to reproduce2,3,5,9. The author recommended the vertical distance between the NAC and the final scar of the inframammary fold to be 2.5 cm, close to what Monstrey et al. (2008)4 orient (half clavicular line and 2-3 cm above the horizontal scar).
When collected in a circular shape, the NAC graft is common to be elliptical with a longer vertical axis over time due to the tension forces in this direction of the chest. To avoid this complication, Agarwal et al. (2017)5 advise removing the elliptical graft measuring 1.5 by 2.5 centimeters and fixing it vertically with the smallest diameter. Over time it tends to have a rounded shape.
This work was based on the author’s casuistry in that period and presented to the examining board for Ascension to Full Member of the Brazilian Society of Plastic Surgery (SBCP - Sociedade Brasileira de Cirurgia Plástica) at the 55th Brazilian Congress, in Recife, in 2018. After the publication of this work, the author will publish future papers with the subsequent experience in this technique described, as well as two others used for smaller breasts: 1) periareolar for patients classified as grades 1 and 2 by Wolter or grade 1 by McEvenue; 2) double incision with a NAC mobilization flap for Wolter grade 3 and McEvenue grade 2 without great flaccidity and ptosis.
CONCLUSION
Mastectomy is a safe procedure with good reproducibility, and that brings satisfactory aesthetic results.
REFERENCES
1. Hage JJ, Karim RB. Ought GIDNOS get nought? Treatment options for nontranssexual gender dysphoria. Plast Reconstr Sur. 2000 Mar;105(3):1222-7.
2. Lo Russo G, Innocenti M. Masculine chest-wall contouring in FtM transgender: a personal approach. Aesthetic Plast Surg. 2017 Abr;41(2):369-74.
3. McEvenue G, Xu FZ, Cai R, McLean H. Female-to-male gender affirming top surgery: a single surgeon’s 15-year retrospective review and treatment algorithm. Aesthet Surg J. 2017 Dez;38(1):49-57.
4. Monstrey S, Selvaggi G, Ceulemans P, Van Landuyt K, Bowman C, Blondeel P, et al. Chest-wall contouring surgery in female-to-male transsexuals: a new algorithm. Plast Reconstr Surg. 2008 Mar;121(3):849-59.
5. Agarwal CA, Wall VT, Mehta ST, Donato DP, Walzer NK. Creation of an aesthetic male nipple areolar complex in female-to-male transgender chest reconstruction. Aesth Plast Surg. 2017 Dez;41(6):1305-10.
6. Top H, Balta S. Transsexual mastectomy: selection of appropriate technique according to breast characteristics. Balkan Med J. 2017 Mar;34(2):147-55.
7. Davidson BA. Concentric circle operation for massive gynecomastia to excise the redundant skin. Plast Reconstr Surg. 1979 Mar;63(3):350-4.
8. Wolter A, Diedrichson J, Scholz T, Arens-Landwehr A, Liebau J. Sexual reassignment surgery in female-to-male transsexuals: an algorithm for subcutaneous mastectomy. J Plast Reconstr Aesthet Surg. 2015 Fev;68(2):184-91.
9. Hage JJ, Van Kesteren PJ. Chest-wall contouring in female-to-male transsexuals: basic considerations and review of the literature. Plast Reconstr Surg. 1995 Ago;96(2):386-91.
10. Lindsay WR. Creation of a male chest in female transsexuals. Ann Plast Surg. 1979;3(1):39-46.
11. Knox ADC, Ho AL, Leung L, Hynes S, Tashakkor AY, Park YS, et al. A review of 101 consecutive subcutaneous mastectomies and male chest contouring using the concentric circular and free nipple graft techniques in female-to-male transgender patients. Plast Reconstr Surg. 2017 Jun;139(6):1260e-72e.
12. Nelson L, Whallett EJ, McGregor JC. Transgender patient satisfaction following reduction mammaplasty. J Plast Reconstr Aesthet Surg. 2009 Mar;62(3):331-4.
13. Colic MM, Colic MM. Circumareolar mastectomy in female-to-male transexuals and large gynecomastias: a personal approach. Aesthetic Plast Surg. 2000 Nov/Dez;24(6):450-4.
14. Takayagi S, Nakagawa C. Chest wall contouring for female-to-male transexuals. Aesthetic Plast Surg. 2006 Mar/Abr;30(2):206-213.
15. Hage JJ, Bloem JJ. Chest wall contouring for female-to-male transsexuals: Amsterdam experience. Ann Plast Surg. 1995 Jan;34(1):59-66.
16. Conte CHR, Correa JPT, Pinto EBS, Rocha PAC, Puhl RC, Daher JAC. Técnica de mastectomia masculinizadora (FTM) - interpretação pessoal. Rev Bras Cir Plást. 2019;34:45-7.
17. Resende JHC. Técnica para correção de ptose mamária masculina pós-grandes emagrecimentos. Rev Bras Cir Plást. 2007;22(1):1-9.
18. Thorek M. Plastic reconstruction of the breast and free transplantation of the nipple. J Int Coll Surg. 1946 Mar/Abr;9:194-224.
19. Tanini S, Lo Russo G. Shape, position and dimension of the nipple areola complex in the ideal male chest: a quick and simple operating room technique. Aesth Plast Surg. 2018 Ago;42(4):951-7.
20. Antoszewski B, Bratos R, Sitek A, Fijalkowska M. Long-term results of breast reduction in female-to-male transsexuals. Pol Przegl Chir. 2012 Mar;84(3):144-51.
1. Hospital Santa Lucinda, Sorocaba, SP,
Brazil.
2. Private Clinic of Plastic Surgery, Dr. Bruno
Marques, Sorocaba, SP, Brazil.
BPAM Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Resources, Software, Supervision, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing.
Corresponding author: Bruno Pires do Amaral Marques, Rua Av Antônio Carlos Comitre, nº 1296 Parque Campolim, Sorocaba, SP, Brazil, Zip code: 18047-620, E-mail: brunopamarques@gmail.com
Article received: February 17, 2019.
Article accepted: July 12, 2021.
Conflicts of interest: none.
Institution: Private Clinic of Plastic Surgery, Dr. Bruno Marques, Sorocaba, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket