



Special Article - Year 2021 - Volume 36 -
The role of magnetic resonance in the evaluation of gluteoplasty: habitual aspects and complications
O papel da ressonância magnética na avaliação da gluteoplastia: aspectos habituais e complicações
Flavio Donaire Cônsolo1,* ; Marcelo Garcia1; Bruno Cerreti Carneiro1; Julio Brandão Guimaraes1; Marcelo Astolfi Nico1; Milena Rocha Souza1; Alipio Gomes Ormond1
; Marcelo Garcia1; Bruno Cerreti Carneiro1; Julio Brandão Guimaraes1; Marcelo Astolfi Nico1; Milena Rocha Souza1; Alipio Gomes Ormond1
ABSTRACT
Introduction: Aesthetic procedures in the gluteal region are increasingly in evidence in recent decades with the augment in demand and the emergence of new techniques. This fact, coupled with the development and easier access to imaging methods and the increasing judicialization of medicine, makes imaging exams more frequent in patients undergoing gluteoplasty, with an emphasis currently on magnetic resonance imaging in this region. Thus, the image increasingly enters the plastic surgeon's daily clinical practice, requiring knowledge of basic concepts regarding the request and interpretation of the exams. In this article, we reviewed aspects of magnetic resonance imaging of aesthetic procedures in the gluteal region and their complications. The objective is to, through magnetic resonance studies, the usual findings in gluteoplasty procedures, as well as some of their complications, in addition to proposing an examination protocol for magnetic resonance imaging in the region. Illustrative cases of patients who underwent gluteoplasty procedures, whether approved, off-label or even illicit, were selected, in which we conducted a magnetic resonance study in our service. A bibliographic review was also done on the topic.
Keywords: Plastic Surgery; Magnetic resonance imaging; Radiology; Silicone elastomers; Silicone Oils.
RESUMO
Introdução: Os procedimentos estéticos na região glútea têm ganhado evidência nas últimas décadas, com aumento da procura e aparecimento de novas técnicas. Somado ao desenvolvimento e maior facilidade de acesso aos métodos de imagem, assim como a crescente judicialização da medicina, tornam-se cada vez mais frequentes os exames de imagem nos pacientes submetidos a gluteoplastia, com destaque atualmente para a avaliação por ressonância magnética desta região. Dessa forma, a imagem entra cada vez mais na prática clínica diária do cirurgião plástico, requerendo do mesmo conhecimentos sobre conceitos básicos em relação à solicitação e interpretação dos exames. Neste artigo, revisamos aspectos de imagem por ressonância magnética de procedimentos estéticos da região glútea, bem como suas complicações. O objetivo é ilustrar através de estudos de ressonância magnética os achados habituais nos procedimentos de gluteoplastia, bem como algumas de suas complicações, além de propor um protocolo de exame por ressonância magnética da região. Foram selecionados selecionados casos ilustrativos de pacientes que se submeteram a procedimentos de gluteoplastia, sejam eles aprovados, off-label ou mesmo ilícitos, e que fizeram estudo de ressonância magnética em nosso serviço. Foi realizada ainda revisão bibliográfica sobre o tema.
Palavras-chave: Cirurgia Plástica; Imagem por Ressonância Magnética; Radiologia; Elastômeros de Silicone; Óleos de Silicone
INTRODUCTION:
Aesthetic procedures in the gluteal region are increasingly in evidence in recent decades. In the United States of America, there was an increase of 86% from 2013 to 2014, reaching in 2014 the number of 21.446 gluteoplasty procedures1. According to data from the Sociedade Brasileira de Cirurgia Plástica, in Brazil from 2008 to 2011, there was a 20% increase in procedures number 2.
This increased demand for the procedure added to the development of new techniques and the greater ease of access to imaging methods, make imaging exams in patients undergoing gluteoplasty increasingly frequent, currently highlighting magnetic resonance imaging evaluation of this region. Thus, the image enters more and more into the plastic surgeon’s daily clinical practice, requiring knowledge about basic concepts regarding the exams’ request and interpretation.
This article reviews magnetic resonance imaging aspects of aesthetic procedures of the gluteal region and its complications.
OBJECTIVE
Illustrate through magnetic resonance studies the usual findings in gluteoplasty procedures and some of its complications. Also, propose a protocol of magnetic resonance sequences to be performed to evaluate the region better, considering the particularities of each suspect of the requesting physician and each procedure performed.
METHODS
Illustrative cases of patients who underwent gluteoplasty procedures were selected, whether approved, off-label, or even illicit3, in which we conducted magnetic resonance imaging in the laboratories of the Fleury group (Fleury brand, Amais and in the imaging service of the Hospital Alemão Oswaldo Cruz, located in the city of São Paulo) in the period between 2016 and 2019, not being the totality of the cases observed, but the most representative cases in relation to the imaging findings.
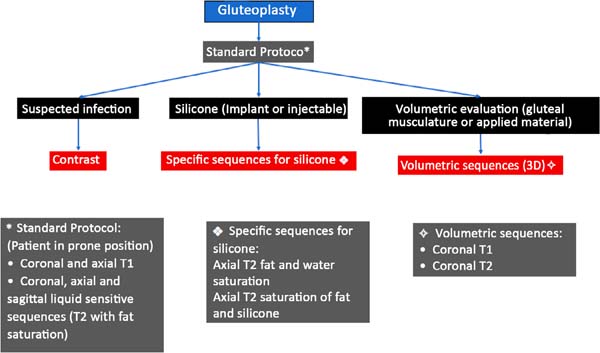
The patients underwent MRI scans on equipment from different manufacturers, all of which were 1.5 Tesla. The protocol for image acquisition was the one we proposed (Figure 1), comprising for each suspicion and type of implant, additions of sequences to the standard protocol usually performed for the cases. The type of procedure to which the patient was submitted was decided by completing a questionnaire directed before the examination and the medical request’s information. When it was necessary, contact was made with the requesting physician to complement the information.

The patients’ examinations were evaluated by at least two radiologists with a subspecialty in musculoskeletal radiology, with experience of 5 and 15 years and graduated from the Brazilian College of Radiology.
DISCUSSION
Silicone implant, lipografting and so-called local flaps are surgical methods recognized in the literature to increase the gluteal region’s projection. Minimally invasive methods with the use of filling materials, in turn, have been gaining space in recent years, being part of the clinical practice of many professionals. Unfortunately, the use of liquid silicone injectables applied by non-medical individuals, or even the application of filling materials by professionals without adequate specialization, is still a Brazilian reality, resulting in often serious complications4.
Regardless of the type of procedure performed, all are subject to complications, the most common being: seroma or hematoma formation, infection, material migration, inflammatory reaction/foreign body, compression of the vasculonervous bundle, among others. In the specific case of silicone implants, we may still have rupture, displacement and capsular contracture5.
For analysis by magnetic resonance (MRI) method, we basically have the sequences in the T1 weighting, in which the fat appears with a high sign (“white”) and demonstrates more conspicuously the anatomy, and the T2-weighted sequences with fat suppression, in which the fat appears with low signal (“dark”), and the areas containing liquid or edema shine (liquid-sensitive sequences). Other additional sequences are employed depending on each particular case: the specific sequences for silicone, post-contrast sequences, and volumetric sequences; for this more specific type of evaluation, we suggest following the protocol in Figure 1.
It is worth mentioning that this protocol consists only of a suggestion based on the practice of imaging diagnoses performed in our service, and no validation of said protocol was performed, which is a relevant limitation of the study.
Silicone implant:
Structurally, silicone implants are composed of a solid silicone elastomer enclosure containing a silicone gel inside6. In the United States, unlike Brazil and other countries, only solid silicone elastomer implantation is approved for gluteoplasties7, to the detriment of silicone gel and saline implant.
On computed tomography (CT) images, the implants are slightly hyperdense compared to muscle6,8, demonstrating intermediate signal intensity on T1 and T2 weighted MRI images9.
Magnetic resonance imaging is the most accurate imaging modality for noninvasive evaluation of implant integrity9.
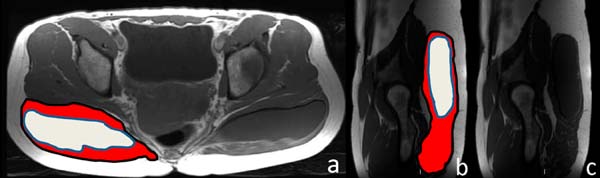
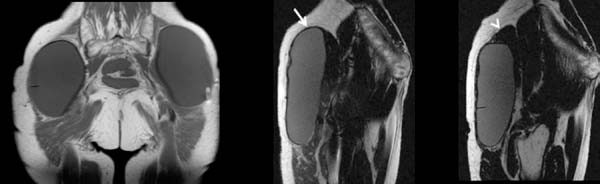
Figure 2 shows a scheme of the usual positioning seen in the axial magnetic resonance sections for the two most common types of the gluteal implants’ location, the intramuscular or subfascial spaces. In Figure 3, we have the usual presentation in the axial section of a patient with an intramuscular implant in T1-weighted and T2-weighted sequences.
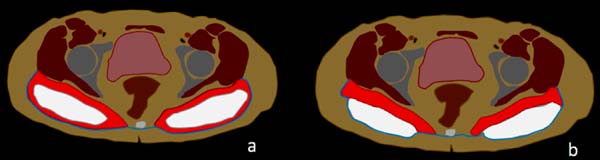

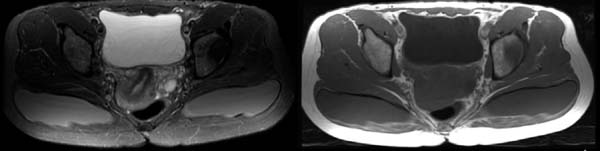
Figure 4 shows how intramuscular implants are seen in T1-weighted sequences, axial plane and also sagittal plane.

Magnetic resonance protocols for evaluating the gluteus implant include sequences similar to those used for breast implant evaluation, with sequences for both silicone signal suppression and accentuation of its signal6,9.
Selective silicone sequences include the suppression of the water and fat signal, which increases the contrast between silicone and surrounding tissues. Similarly, a sequence that suppresses the silicone signal provides a useful additional means to confirm, for example, whether extracapsular silicone is present9.
The depth of positioning of silicone implants varies by anatomical location and has implications concerning the types of complications observed after surgery. They can be inserted more commonly in intramuscular or subfascial spaces10,11 (figure 2).
In a plane created within the gluteus muscle fibers, the implant’s intramuscular placement is the most popular because it provides satisfactory aesthetic results and a lower prevalence of complications10,11.
A systematic review of the literature reported complication rates for different sites of prostheses placement: 55% for subfascial, 18% for intramuscular, 18% for submuscular methods and 13% for methods with intramuscular technique XYZ11.
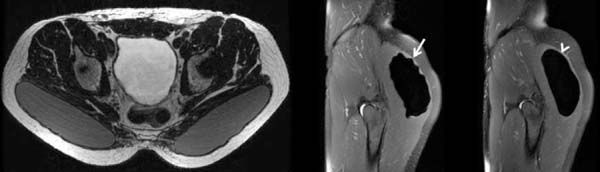
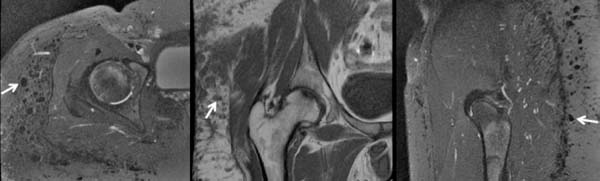
Oranges et al.10, in turn, reviewed the literature that showed an overall complication rate of 30.5% for cosmetic surgeries of gluteus implant, the most prevalent being: surgical wound dehiscence (8.1%), seroma (4.4%), infection (3.2%) (figure 5) and implant revision (3.1%). Other complications reported, however, less frequent, are rupture of the prosthesis (figure 6), displacement (figure 7) and contracture (figure 8).




The number of procedures has been falling in the last two years in the United States, possibly because it presents a percentage of complications still considered high, a more limiting postoperative period with absence from usual activities for longer than other techniques, in addition to large scars. This number decreased by 56% from 2016 to 2017 and by 28% from 2017 to 2018, with less than 1,000 procedures being performed this past year12.
Autologous lipografting:
Autologous lipografting is characterized by a procedure for collecting fat from the site where removal is aesthetically desired, such as the abdomen or thighs, and transfer to increase other areas in the same patient, commonly in the buttocks. In the American market, the method is known as”Brazilian buttock lift”13.
According to the American Society of Plastic Surgeons, procedures in the United States increased 10% from 2016 to 2017 and 19% from 2017 to 2018, with more than 24,000 being performed this past year.12.
Better aesthetic results are obtained by combining subcutaneous, subdermal and intramuscular injections for augmentation gluteoplasty14,15.
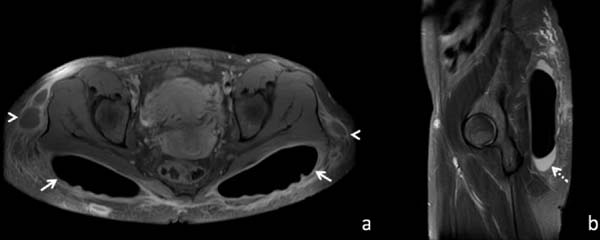
On CT or MRI images (figure 9), fat grafting on the subcutaneous is difficult to characterize due to similar characteristics with subcutaneous cellular tissue. On the contrary, the fat injected in the intramuscular region is easily identified by both methods, such as lobular foci of macroscopic fat, with low characteristic density on tomography (values of - 150 to -50 Hounsfield units), of permeate to muscle fibers, and with high signal in conventional sequences weighted in T1, on magnetic resonance imaging. The adipose nature is confirmed with the fat suppression sequences on MRI, presenting low signal, both in T1 and T2( weighting6.


Magnetic resonance imaging (MRI) can be used to document the integration of the fat graft and volumetric variations produced in the buttocks after lipografting10.
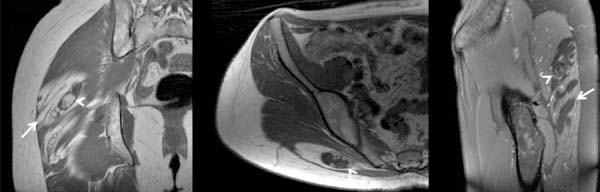
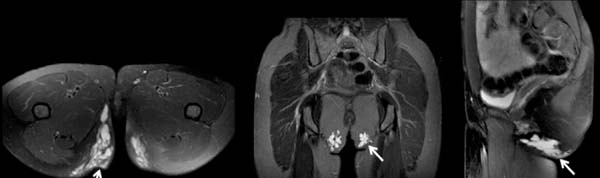
In the literature10, there is a global rate of complications in patients with autologous lipografting of 10.5%, and donor site seroma is the most common complication (3.1%). Other complications reported were: liponecrosis (0.7%) (figure 10), cellulitis (0.5%), asymmetry (0.4%), infection (0.3 %) and fatty embolism (0.2%).
Compared to silicone implants, lipografting has the advantages of being more targeted and allowing the concomitant conformation of the hip and waist regions, which affects the overall aesthetic appearance of the gluteus17 a more natural result. It also allows a higher degree of increase and less evident scars7. Moreover, the rate of complications is lower than for implants6.

Filling Materials:
The use of dermal filling materials has grown sharply in recent years, totaling more than 2.6 million procedures in 2018 in the United States, more than three times the number of procedures performed in 200012.
As the indications and the number of procedures performed increase, the number of complications is likely to increase18.
Concerning classification can be divided into absorbable/temporary (hyaluronic acid, collagen, polyacrylamide gel, poly-L-lactic acid, calcium hydroxyapatite) and non-absorbable/permanent acid (polymethylmethacrylate).
Although some studies report these materials’ imaging characteristics in magnetic resonance imaging6, the literature’s data are still scarce, so the signal pattern is still considered in general nonspecific. Thus, magnetic resonance imaging is more used to evaluate possible complications, besides determining the location, quantity and extent of the applied material.
Magnetic resonance imaging can detect amounts as small as 2 mm in diameter of filling materials, in addition to complications such as abscesses and granulomas that have not been clinically detected19.
The use in small amounts and specific regions, such as the face and back of the hands, is well established in plastic surgery. However, the use of larger volumes and other body sites, such as the gluteal region, is still a controversial issue.
Some European authors have published studies using hyaluronic acid applied to the subcutaneous region of the gluteal region20,21, with volumes of up to 400 ml per patient, with satisfactory results. They emphasize in their studies that traditional methods of gluteoplasty are all surgical procedures that usually require general anesthesia and/or produce scarring. Consequently, many people are looking for minimally invasive procedures. Hyaluronic acid is chosen because it is easy to use, biocompatible, non-toxic and easily removable, if necessary 20. Material degradation results in volume reduction over time, which can be evaluated by magnetic resonance imaging20. The overall rate of complications with the use of hyaluronic acid in these two studies was equal to 39.1%, and none of the complications evaluated was severe. Among the most frequent complications reported are swelling (7.2 %), pruritus (7.2 %), pain at the injection site (5.8 %), hematoma (5.8 %), displacement of the material (4.3 %)10.
Other authors 22,23 reported in their articles the use of poly-L-lactic acid (PLLA) for filling in the gluteal region, with the application of the material in the subcutaneous, using volumes of up to 48 ml per buttock per session. They did not report serious complications. Unlike other temporary filling materials that basically act occupying space, such as collagen and hyaluronic acid-based products, poly-L-lactic acid (PLLA) aims to gradually promote collagen deposition through a biostimulator response, with therapeutic effects that last approximately two years24.
A recent publication25 brings a consensus on recommendations regarding (PMMA) in Brazil for facial and body aesthetic procedures. According to the publication, deeper plans should be chosen whenever possible for body treatment with PMMA. Subcutaneous, intramuscular and submuscular planes can be used based on the needs of each patient. According to the experts’ recommendations, the volume applied in the gluteal region can reach 150 ml in a single application.
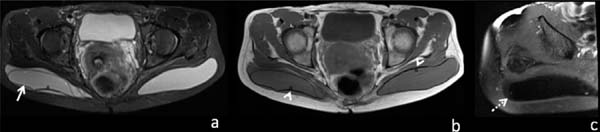
Figure 11 illustrates a case of polymethylmethacrylate gluteoplasty on magnetic resonance imaging in an asymptomatic patient, and Figure 12 illustrates a case of late complication with a local inflammatory process, but in this case, liquid silicone was associated.
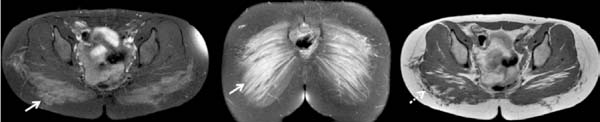


We have not found in the literature reports of polyacrylamide gel (PAAG) in the gluteal region. We have one case using this material in an asymptomatic patient (figure 13) and another with material migration (figure 14).



It is important to maintain a high rate of clinical suspicion of infection when filling agents are identified in imaging tests because abscesses can be difficult to differentiate from certain materials that have CT and MRI imaging characteristics close to those of water, such as hyaluronic acid5. However, abscesses tend to exhibit a higher degree of enhancement around by intravenous contrast26.
Silicone:
The Agência Nacional de Vigilância Sanitária (National Health Surveillance Agency) (Anvisa) prohibits industrial silicone for aesthetic procedures. The illegal application of industrial silicone in the human body is considered a crime against public health provided for in the Penal Code. Of course, cosmetic augmentation silicone injection is also not approved by the U.S. Food and Drug Administration (FDA).
Nevertheless, this practice is still present, possibly due to low costs compared to approved surgical procedures and the lack of information on the associated risks. The gluteal region is one of the most common sites of application of the material5.
Liquid silicone is as dense or slightly denser than soft parts on tomography. In MRI, it tends to demonstrate intermediate signal intensity or slightly higher than the water signal in T1-weighted images and variable intensity in T2-weighted images, possibly due to different viscosities, with high viscosity silicone generally more hypointense at T2 6,7,8,16,27,28.
In the specific sequence for silicone, with suppression of the water and fat signal, it has a high signal19.
Because silicone permanently resides in tissues, surgical removal may be the only way to treat chronic problems. However, surgical removal of silicone can be very difficult for the surgeon and disfiguring for the patient. Preoperative MRI with specific silicone sequences can help define and locate the material before any surgical attempt to locate the silicone and facilitate identification and removal by the surgeon8.
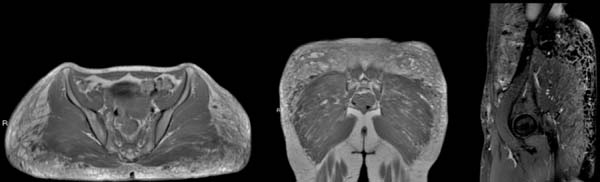
The host’s tissue response after silicone injection results in the formation of granulomas6 (figure 15). Granulomatous reactions can occur weeks to decades after injection7.

Minor complications include injection site reaction, erythema, edema, and scars12. Due to silicone impurities and the non-sterile conditions under which injections often occur, these procedures can be complicated by chronic cellulitis, abscesses, and myositis. Other local silicone injection complications include migration, hyperpigmentation and fibrosis of the skin, necrosis, ulceration, fistula, disfigurement6.
CONCLUSION
We present the common findings on magnetic resonance imaging of gluteoplasty procedures, together with the spectrum of images of some of its possible complications, in addition to an organization chart with suggested magnetic resonance protocol.
REFERENCES
1. https://doi.org/10.1093/asj/35.Supplement_2.1
2. Lima DA, Minakami DA, Pereira LC, Grando MC, Cruz RS, Braga AR, et al. Gluteoplasty augmentation: the importance of teaching of training residents to meet increasing demand. Rev Bras Cir Plást. 2011;26(1):127-33.
3. Nakamoto HA, Goldenberg D. We need to discuss gluteal fat grafting. Rev Bras Cir Plást. 2018;33(3):270-1.
4. Chasan PE. The history of injectable silicone fluids for soft-tissue augmentation. Plast Reconstr Surg. 2007 Dez;120(7):2034-40;discussion:2041-3.
5. http://dx.doi.org/10.1097/sap.0000000000001765
6. Lin DJ, Wong TT, Ciavarra GA, Kazam JK. Adventures and misadventures in plastic surgery and soft-tissue implants. Radiographics. 2017 Nov/Dez;37(7):2145-63.
7. Yahyavi-Firouz-Abadi N, Menias CO, Bhalla S, Siegel C, Gayer G, Katz DS. Imaging of cosmetic plastic procedures and implants in the body and their potential complications. AJR Am J Roentgenol. 2015 Abr;204(4):707-15.
8. Frank SJ, Flusberg M, Friedman S, Sternschein M, Wolf EL, Stein MW. Aesthetic surgery of the buttocks: imaging appearance. Skeletal Radiol. 2014 Fev;43(2):133-9.
9. Seiler SJ, Sharma PB, Hayes JC, Ganti R, Mootz AR, Eads ED, et al. Multimodality imaging-based evaluation of single-lumen silicone breast implants for rupture. Radiographics. 2017 Mar/Abr;37(2):366-82.
10. Oranges CM, Tremp M, Di Summa PG, Haug M, Kalbermatten DF, Harder Y, et al. Gluteal augmentation techniques: a comprehensive literature review. Aesthet Surg J. 2017 Mai;37(5):560-9.
11. Flores-Lima G, Eppley BL, Dimas JR, Navarro DE. Surgical pocket location for gluteal implants: a systematic review. Aesthetic Plast Surg. 2013 Jan;37(2):240-5.
12. American Society of Plastic Surgeons (ASPS). 2018 National Plastic Surgery Statistics: cosmetic and reconstructive procedure trends [Internet]. Arlington Heights: ASPS; 2018; [access in 2019 May 15]. Available from:
13. https://doi.org/10.1093/asj/sjx004
14. Toledo LS. Gluteal augmentation with fat grafting: the Brazilian buttock technique: 30 years' experience. Clin Plast Surg. 2015 Abr;42(2):253-61.
15. Condé-Green A, Kotamarti V, Nini KT, Wey PD, Ahuja NK, Granick MS, et al. Fat grafting for gluteal augmentation: a systematic review of the literature and meta-analysis. Plast Reconstr Surg. 2016 Set;138(3):437e-46e.
16. Wolf GA, Gallego S, Patrón AS, Ramírez F, Delgado JA, Echeverri A, et al. Magnetic resonance imaging assessment of gluteal fat grafts. Aesthetic Plast Surg. 2006 Jul/Ago;30(4):460-8.
17. Sinno S, Chang JB, Brownstone ND, Saadeh PB, Wall Junior S. Determining the safety and efficacy of gluteal augmentation: a systematic review of outcomes and complications. Plast Reconstr Surg. 2016 Abr;137(4):1151-6.
18. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013 Dez;6:295-316.
19. Mundada P, Kohler R, Boudabbous S, Trellu LT, Platon A, Becker M. Injectable facial fillers: imaging features, complications, and diagnostic pitfalls at MRI and PET CT. Insights Imaging. 2017 Dez;8(6):557-72.
20. Camenisch CC, Tengvar M, Hedén P. Macrolane for volume restoration and contouring of the buttocks: magnetic resonance imaging study on localization and degradation. Plast Reconstr Surg. 2013 Out;132(4):522e-9e.
21. De Meyere B, Mir-Mir S, Peñas J, Camenisch CC, Hedén P. Stabilized hyaluronic acid gel for volume restoration and contouring of the buttocks: 24-month efficacy and safety. Aesthetic Plast Surg. 2014 Abr;38(2):404-12.
22. Lorenc ZP. Techniques for the optimization of facial and nonfacial volumization with injectable poly-L-lactic acid. Aesthetic Plast Surg. 2012 Out;36(5):1222-9.
23. Mazzuco R, Sadick NS. The use of poly-L-lactic acid in the gluteal area. Dermatol Surg. 2016 Mar;42(3):441-3.
24. Jabbar A, Arruda S, Sadick N. Off face usage of poly-L-lactic acid for body rejuvenation. J Drugs Dermatol. 2017 Mai;16(5):489-94.
25. Souza TAB, Colomé LM, Bender EA, Lemperle G. Brazilian consensus recommendation on the use of polymethylmethacrylate filler in facial and corporal aesthetics. Aesthetic Plast Surg. 2018 Out;42(5):1244-51.
26. Ginat DT, Schatz CJ. Imaging features of midface injectable fillers and associated complications. AJNR Am J Neuroradiol. 2013 Ago;34(8):1488-95.
27. Cheung YC, Su MY, Ng SH, Lee KF, Chen SC, Lo YF. Lumpy silicone-injected breasts: enhanced MRI and microscopic correlation. Clin Imaging. 2002 Nov/Dez;26(6):397-404.
28. Mathews VP, Elster AD, Barker PB, Buff BL, Haller JA, Greven CM. Intraocular silicone oil: in vitro and in vivo MR and CT characteristics. AJNR Am J Neuroradiol. 1994 Fev;15(2):343-7.
1. Fleury, Radiologia, São Paulo, SP, Brazil.
FDC Análise e/ou interpretação dos dados, Análise estatística, Aprovação final do manuscrito, Aquisição de financiamento, Coleta de Dados, Conceitualização, Concepção e desenho do estudo, Gerenciamento do Projeto, Investigação, Metodologia, Realização das operações e/ ou experimentos, Redação - Preparação do original, Redação - Revisão e Edição, Supervisão, Validação
MG Análise e/ou interpretação dos dados, Análise estatística, Conceitualização, Concepção e desenho do estudo, Metodologia, Realização das operações e/ou experimentos, Redação - Revisão e Edição, Supervisão, Visualização
BCC Análise estatística, Conceitualização, Investigação, Metodologia
Corresponding author: Flavio Donaire Cônsolo Rua Pernambuco, Higienópolis, 210, Apart. 61B, São Paulo, SP, Brazil. Zip Code: 01240-020 E-mail: fconsolo@me.com
Article received: February 06, 2020.
Article accepted: January 10, 2021.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket