



Case Report - Year 2021 - Volume 36 -
Multicystic epithelioid mesothelioma infiltrating abdominal wall and thigh: case report
Mesotelioma epitelioide multicístico infiltrando parede abdominal e coxa: relato de caso
Danilo Rafael da Silva Fontinele1,* ; Gilvander Cesar Martins1; Iran Batista de Brito2; Sabas Carlos Vieira3; Edimar Duarte Val2; Caio Alcobaça Marcondes2
; Gilvander Cesar Martins1; Iran Batista de Brito2; Sabas Carlos Vieira3; Edimar Duarte Val2; Caio Alcobaça Marcondes2
ABSTRACT
Multicystic epithelioid mesothelioma is a rare benign tumor that arises from changes in peritoneal mesothelial cells. We report a large multicystic epithelioid mesothelioma case in a female patient with infiltration into the abdominal wall and thigh. Extensive tumor resection and reconstruction were performed with multiple fasciocutaneous flaps randomized in the abdominal region, flanks, right and left thigh flaps and vulva flap. It has been in full healing for nine months without recurrence and complaints.
Keywords: Mesothelioma; Abdomen; Thigh; Cystic mesothelioma; Neoplasms.
RESUMO
O mesotelioma epitelioide multicístico é um tumor benigno raro que surge a partir de modificações nas células mesoteliais peritoneais. Relatamos um caso de um grande mesotelioma epitelioide multicístico em paciente do sexo feminino com infiltração em parede abdominal e coxa. Foi realizada a ressecção ampla do tumor e reconstrução com múltiplos retalhos fasciocutâneos randomizados em região do abdome, flancos, retalhos de coxa direita e esquerda e retalho de vulva. Segue há 9 meses com cicatrização completa sem recidiva e sem queixas.
Palavras-chave: Mesotelioma; Abdome; Coxa da perna; Mesotelioma cístico; Neoplasias.
introduction
Multicystic epithelioid mesothelioma is an unusual benign tumor that arises from changes in peritoneal mesothelial cells and accounts for 3 to 5% of peritoneal mesotheliomas, with an estimated size incidence of 2 per 1,000,000 per year1-3. The first report was described in 1979 in a young woman with omental, peritoneal, and pelvic involvement3,4.
The pathology is more prevalent in young women1,2,5, and its etiopathogenesis is still controversial6. Although there are other theories, inflammatory processes in the peritoneum have been the main associated etiopathogenic mechanism2.
Thus, we report a case of multicystic epithelioid mesothelioma in a female patient with infiltration into the abdominal wall and thigh.
CASE REPORT
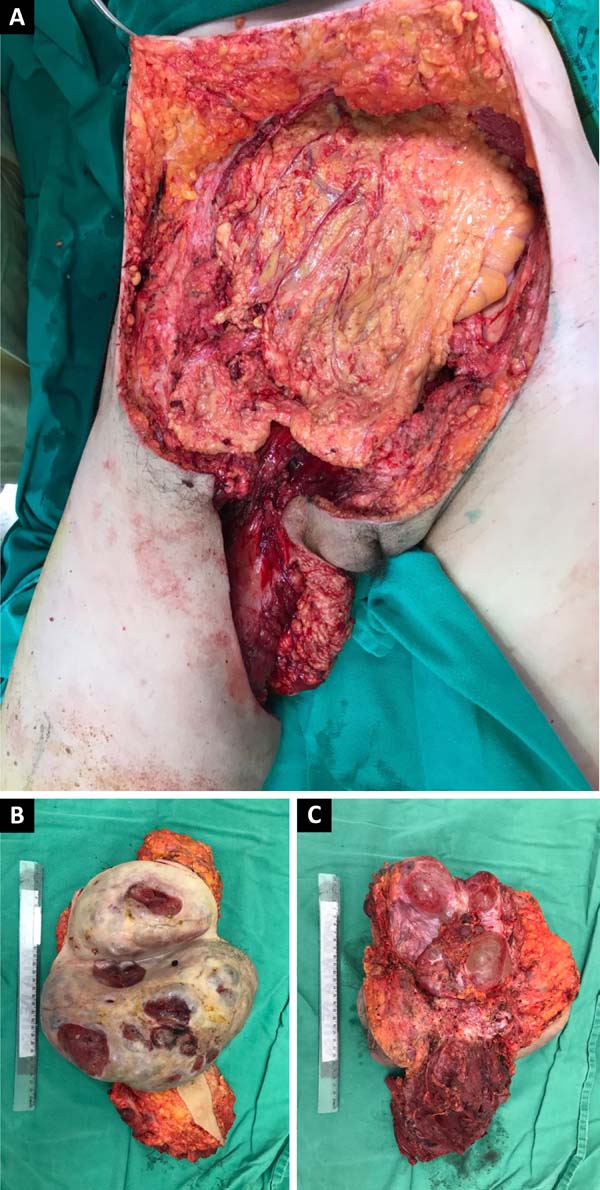
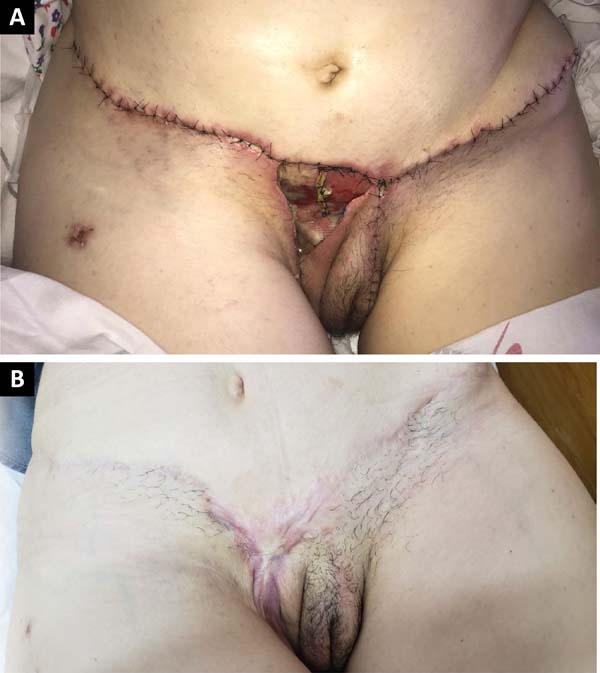
Female patient, 49 years old. Five years ago, she presented a large tumor of soft parts in the pelvic wall at the level of the pubic region, fixed to the deep planes. Magnetic resonance imaging revealed an extensive multiloculated solid-cystic lesion affecting the anterior wall of the lower abdomen, compromising the subcutaneous tissue, the muscle planes and, in close relationship with the posterior aponeurosis, measuring 13.8x12.8x10.3cm, wide resection of the tumor was performed. Histopathological revealed a multicystic epithelioid neoplasm, and immunohistochemistry confirmed multicystic peritoneal mesothelioma. After two years, she presented solid nodules in the pelvic abdominal wall with neoplastic characteristics and umbilical hernia, and a biopsy was indicated. After another two years, and without performing a biopsy of the lesion, she had a large, recurrent soft tissue tumor in the pelvic wall and pubic region (Figure 1). Tomography of the pelvis with multiple cystic lesions, grouped and clustered in the anterior abdominal region measuring 20x9 cm predominantly to the left, extending to the inguinal region and right thigh measuring 19x20 cm. The patient underwent extensive tumor resection with reconstruction with multiple fasciocutaneous flaps randomized in the abdomen, flanks, right and left thigh flaps and vulva flap (Figure 2). The resection product weighed 4,832g, with the following dimensions 32.0x21.0x14.0cm (Figure 2). Histopathological confirmed multicystic epithelioid mesothelioma infiltrating abdominal wall and thigh. She evolved with partial necrosis of the vulva flap on the 12th postoperative day. Conservative treatment was performed with 0.6U/g collagenase ointment (Figure 3). It has been with complete healing for nine months (Figure 4), with no recurrence and complaints. Publication approved by the ethics and research committee with the opinion of no. 4,311,835.






discussion
Multicystic epithelioid mesothelioma is a rare syndrome of recurrent peritoneal mesothelial cysts4. There are fewer than 200 reported cases worldwide if we consider the reports made during 20176,7. Due to its rarity, its natural history and pathogenesis are still little explored1,5. Most of the studies in the literature are from retrospective series or case reports7.
It affects more females than males, having a higher incidence during reproductive age1,5, the mean age of occurrence is 36 years6, which differentiates from the case in question. It is an extremely rare disease in men, prevalent in individuals aged in the sixth decade of life6.
The literature shows that the lesion is diffusely distributed in the abdomen and pelvis, with the peritoneum of the pelvic organs being the most common site 4. It is considered that its appearance is associated with previous surgery, endometriosis or abdominal inflammation5,6. There are theories based on hormonal hypothesis, in which the development and progression of the disease would be linked to their sensitivity to sexual hormones6,8. Symptoms of multicystic mesothelioma are usually absent and occur mainly due to the mass effect on other organs6. Abdominal discomfort, abdominal distension, and the presence of an abdominal mass on physical examination are observed7,8.
Magnetic resonance imaging has been used as the method of choice. However, studies have shown little value as an accurate diagnosis of multicystic mesothelioma since, mainly due to the lack of clinical and imaging presentation, the preoperative diagnosis is challenging1,5,8. It may be a situation diagnosed incidentally during other abdominal surgeries6,9. Its final diagnosis requires histological evaluation of a surgical sample8.
There are no guidelines available for the conduct of cases. However, the central management is complete surgical resection7, which presents a recurrence rate between 40 and 50%. A study with 19 cases used a combination of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC). It concluded that such a combination offers a low recurrence rate (21%), good relapse-free survival, and acceptable morbidity10. However, there is a lack of comparative data on recurrence and complications of the association of this treatment7.
Malignant transformation is rare2,4. In a follow-up study with 75 cases, malignant transformation was diagnosed in only one case9. The prognosis is very good, with only one reported death attributed to the disease6.
conclusion
The neoplasm in question is rare, especially in the dimensions presented in this case. Diagnosis and treatment must not be delayed. The oncology surgeon and the plastic surgeon should discuss and plan these cases. In addition, attention should be paid to relapses.
REFERENCES
1. Noiret B, Renaud F, Piessen G, Eveno C. Multicystic peritoneal mesothelioma: a systematic review of the literature. Pleura Peritoneum. 2019 Set;4(3):20190024.
2. Canu GL, Medas F, Columbano G, Gordini L, Saba L, Erdas E, et al. Benign multicystic peritoneal mesothelioma in a male patient with previous Wilms’ tumor: a case report and review of the literature. Case Rep Surg. 2018;2018:4324986.
3. Jouvin I, Dohan A, Gergi P, Pocard M. Intra-abdominal benign multicystic peritoneal mesothelioma. J Visc Surg. 2014 Abr;151(2):155-7.
4. Lang A, Chaudhri P. Benign multicystic mesothelioma arising from the tunica vaginalis. J Surg Case Rep. 2019 Jan;2019(1):rjy361.
5. Zhang CH, Yu JW, Luo M. Multicystic peritoneal mesothelioma: a short review. Curr Probl Cancer. 2017 Set/Out;41(5):340-8.
6. Khurram MS, Shaikh H, Khan U, Edens J, Ibrar W, Hamza A, et al. Benign multicystic peritoneal mesothelioma: a rare condition in an uncommon gender. Case Rep Pathol. 2017; :20179752908.
7. Gussago S, Spina P, Guerra A. Benign multicystic peritoneal mesothelioma (BMPM) as a rare cause of abdominal pain in a young male: case report and review of the literature. J Surg Case Rep. 2019 Mar; 2019 (3):rjz057.
8. Wang TB, Dai WG, Liu DW, Shi HP, Dong WG. Diagnosis and treatment of benign multicystic peritoneal mesothelioma. World J Gastroenterol. 2013 Out;19(39):6689-92.
9. Sun M, Zhao L, Weng LI, Yu L, Wang J. Well-differentiated papillary mesothelioma: a 17-year single institution experience with a series of 75 cases. Ann Diagn Pathol. 2019 Fev;38:43-50.
10. Nizri E, Baratti D, Guaglio M, Sinukumar S, Cabras A, Kusamura S, et al. Multicystic mesothelioma: operative and long-term outcomes with cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. Eur J Surg Oncol. 2018 Jul;44(7):1100-4.
1. State University of Piauí, Teresina, PI, Brazil.
2. São Marcos Hospital, Teresina, PI, Brazil.
3. Oncocentro, Teresina, PI, Brazil.
DRSF Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Funding Acquisition, Methodology, Realization of operations and/or trials, Resources, Software, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing.
GCM Analysis and/or data interpretation, Final manuscript approval, Resources, Software, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing.
IBB Analysis and/or data interpretation, Conceptualization, Data Curation, Final manuscript approval, Methodology, Realization of operations and/or trials, Resources, Software, Validation, Visualization, Writing - Original Draft Preparation.
SCV Analysis and/or data interpretation, Conceptualization, Data Curation, Final manuscript approval, Funding Acquisition, Investigation, Methodology, Realization of operations and/or trials, Software, Supervision, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing.
EDV Analysis and/or data interpretation, Data Curation, Final manuscript approval, Formal Analysis, Investigation, Realization of operations and/or trials, Supervision, Validation, Writing - Original Draft Preparation.
CAM Analysis and/or data interpretation, Data Curation, Final manuscript approval, Formal Analysis, Investigation, Realization of operations and/or trials, Resources, Validation, Visualization, Writing - Review & Editing.
Corresponding author: Danilo Rafael da Silva Fontinele Rua Olavo Bilac, nº 2335 - Centro (Sul), Teresina, PI, Brazil Zip Code 64001-280 E-mail: drsilvafontinele@gmail.com
Article received: May 19, 2020.
Article accepted: April 23, 2021.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket