



Original Article - Year 2021 - Volume 36 - Issue 2
Epidemiological profile of burned patients at the Clinical Hospital of the Federal University of Uberlândia in Brazil
Perfil epidemiológico dos pacientes queimados no Hospital de Clínicas da Universidade Federal de Uberlândia
Douglas Ravel Neto Diniz Ribeiro1,* ; Sinval Soares Cruvinel1; Phelipe Augusto Costa1; Hiléia Carolina de Oliveira Valente1; Tauã Richel Belchior da Costa1
; Sinval Soares Cruvinel1; Phelipe Augusto Costa1; Hiléia Carolina de Oliveira Valente1; Tauã Richel Belchior da Costa1
ABSTRACT
Introduction: Burns are lesions caused by agents external to organic tissues, in which there is the destruction of the epithelial lining and/or mucous membranes in varying depth and extension. This study aims to analyze the epidemiological profile of burned patients admitted to the Clinical Hospital of the Federal University of Uberlândia, Minas Gerais, Brazil.
Methods: Data were obtained by collecting medical records of patients admitted to the emergency room and burn Unit of the Hospital de Clínicas, from January 1, 2015, to December 31, 2019.
Results: Of the 305 patients analyzed, 59.2% were male, the age group from 0 to 9 years was the most representative (24.03%) and brown ethnicity with the highest number of episodes (42.53%). Regarding hospitalization length, 57% of the cases were hospitalized less than ten days and the mean total hospitalization time was 26.61 days. It was found that the most frequent incident was exposure to explosive agents or combustion of flammable substances (43.51%) and that liquid alcohol was the most common etiological agent (30.51%).
Conclusion: The relevance of the epidemiological profile is observed since it identifies the main risk groups. According to the references used, the importance of prevention and surveillance is highlighted, focusing on reducing morbidity and mortality.
Keywords: Burns; Epidemiology; Plastic surgery; Research on health services; Burn units.
RESUMO
Introdução: Queimaduras são lesões causadas por agentes externos aos tecidos orgânicos, nas quais há destruição do revestimento epitelial e/ou mucosas em profundidade e extensão variáveis. Objetiva-se neste estudo analisar o perfil epidemiológico de pacientes queimados, admitidos no Hospital de Clínicas da Universidade Federal de Uberlândia, Minas Gerais, Brasil.
Métodos: A obtenção dos dados ocorreu por meio do levantamento de prontuários de pacientes admitidos no pronto socorro e unidade de queimados do Hospital de Clínicas, no período de 01 de janeiro de 2015 a 31 de dezembro de 2019.
Resultados: Dos 305 pacientes analisados, 59,2% foram do sexo masculino, a faixa etária de 0 a 9 anos foi a de maior representatividade (24,03%) e a etnia parda a de maior número de episódios (42,53%). Quanto ao tempo de internação, 57% dos casos ficaram internados menos de 10 dias e a média do tempo de internação total foi de 26,61 dias. Constatou-se que o incidente de maior frequência foi a exposição a agentes explosivos ou à combustão de substâncias inflamáveis (43,51%) e que o álcool líquido foi o agente etiológico mais comum (30,51%).
Conclusão: Observa-se a relevância do perfil epidemiológico, já que esse identifica os principais grupos de risco. De acordo com as referências utilizadas, fica em evidencia a importância da prevenção e da fiscalização com foco na redução da morbidade e mortalidade.
Palavras-chave: Queimaduras; Epidemiologia; Cirurgia plástica; Pesquisa sobre serviços de saúde; Unidades de queimados
INTRODUCTION
Burns are traumatic injuries to the skin caused by chemical, thermal, electrical and radioactive agents. Besides, these injuries can affect adjacent organs, with the highest prevalence of burns in residential kitchens. These injuries can occur in simple or severe forms and are classified based on aspects such as depth, extent and location1.
According to the World Health Organization, an estimated 180,000 deaths per year are caused by burns, most of which occur in low- and middle-income countries2. In this context, according to the Ministry of Health, it is estimated that approximately 1 million burn accidents occur in Brazil per year, regardless of any characteristics such as sex, age, origin or social class. Of these victims, around 100,000 seek hospital care, and around 2,500 die from their injuries3. The prognosis of burns depends, mainly, on the initial approach and appropriate treatments, which can reduce mortality, complications, scar sequelae, and possible reconstruction needs in future surgeries. The best prognosis is associated with the emergence of specialized centers, improvement in resuscitation protocols, individualization in intensive care, earlier coverage of wounds and progress in treating infections, inhalation injuries and hypermetabolism. These advances4 impacted the morbidity and mortality of burn victim patients.
The percentage of burned body surface (BBS) and the presence of inhalation injury are associated with a worse prognosis and greater severity. Recent studies show that the extension of BBS in adults is linked to an increased risk of mortality, especially when the BBS is greater than 60% and no more than 40%, as established in past studies4.
In Brazil, among the main external causes of death recorded, burns are second only to other violent causes, such as transport accidents and homicides. Burn is considered an aggressive injury in human beings’ lives; in addition to the high incidence and mortality, it has a great capacity to leave functional, aesthetic and psychological sequelae5.
Accidents that cause burns in our country become a major health problem, affecting different age groups and sexes. Besides leaving sequelae, such accidents may require several days of hospitalization and require therapeutic monitoring, including psychological monitoring, after hospital discharge. Epidemiology and the study of statistical data on these injuries are still insufficient6. The knowledge of these data is of great scientific relevance, given the need to provide information for public health planning or research to encourage actions that favor guidance and awareness, as important instruments for preventing this type of accident and for the promotion of population health.
OBJECTIVE
This study proposes to trace the epidemiological profile of burn cases treated at the Emergency Room and the Burn Unit at the Hospital de Clínicas of the Universidade Federal de Uberlândia (HC-UFU), Minas Gerais (MG), Brazil, over five years considered from 2015 to 2019.
METHODS
This study is a quantitative analysis with a retrospective and descriptive approach. After authorization from the institution and agreement by the Ethics and Research Council (CEP-UFU) for the use of its documents, in the CAAE opinion number: 33395220.3.0000.5152, the medical records of patients admitted with burns were analyzed, regardless of the extension and depth, at HC-UFU Emergency Room and Burn Unit from January 1, 2015, to December 31, 2019. This Unit is characterized as a regional reference hospital for medium and high complexity care.
Based on hospital discharge reports from the HC-UFU statistics sector, a database was created with a sample of 305 patients admitted to the hospital in 308 burn events. To avoid the risks of identifying the participants, systematization was carried out by replacing the reference number of the medical records with random five-digit numbers.
The following nominal scales were analyzed: time of hospitalization, etiological agent, gender, ethnicity, age, percentage of the burned body surface, burn depth and affected sites. It is important to point out that not all medical records had the nominal scales completely filled out, but the information contained was fully considered.
RESULTS
The study had the participation of 305 patients admitted with burn complaints, regardless of the extent and depth, in the emergency room and in the burn unit of HC-UFU; of the total number of people in the study, 183 (59.02%) are males and 124 (40.66%) females.
Of the patients, 74 (24.03%) were between 0 and 9 years old, and 47 (15.26%) were between 40 and 49 years old (Table 1), a portion that represents the majority of patients admitted to the hospital. Among the patients from 0 to 9 years old, 35 (11.36% of the total hospitalized) were between 0 and 2 years old.
| Age Group | Burns per year | Total Burns | Total % | ||||
|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | |||
| 0 to 9 years | 13 | 5 | 17 | 18 | 21 | 74 | 24.03 |
| 10 to 19 years | 4 | 2 | 7 | 7 | 7 | 27 | 8.77 |
| 20 to 29 years | 6 | 5 | 7 | 11 | 9 | 38 | 12.34 |
| 30 to 39 years | 8 | 9 | 14 | 14 | 16 | 61 | 19.81 |
| 40 to 49 years | 5 | 6 | 6 | 20 | 10 | 47 | 15.26 |
| 50 to 59 years | 6 | 5 | 7 | 8 | 10 | 36 | 11.69 |
| 60 to 69 years | 2 | 1 | 2 | 6 | 8 | 19 | 6.17 |
| Over 70 years | 1 | 0 | 1 | 2 | 2 | 6 | 1.95 |

Regarding the ethnicity of the patients, 149 (48.38%) declared as brown, 131 (42.53%) whites, 22 (7.14%) blacks, 2 (0.65%) and 4 patients (1.30%) manifested to be of another unspecified ethnicity.
Regarding the hospitalization period, 127 (41%) burns remained hospitalized in the Unit from 0 to 10 days, the interval from 11 to 21 days had a frequency of 26% (79 patients), 29 (9%) remained hospitalized between 22 to 31 days, and 73 (24%) remained for a period greater than 32 days. The average total hospital stay was 26.61 days (Table 2).
| Burns per year | Total cases | % | ||||||
|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | ||||
| Length of stay | 0 to 10 days | 12 | 12 | 27 | 40 | 36 | 127 | 41.23 |
| 11 to 21 days | 17 | 8 | 16 | 20 | 18 | 79 | 25.65 | |
| 22 to 31 days | 4 | 1 | 7 | 9 | 8 | 29 | 9.42 | |
| 32 or more days | 12 | 12 | 12 | 17 | 20 | 73 | 23.70 | |
| Total events | 45 | 33 | 62 | 86 | 82 | 308 | 100.00 | |
| Total days hospitalized | 1476 | 1207 | 1195 | 1700 | 2021 | 7599 | - | |
| Average days hospitalized | 32.80 | 36.58 | 19.27 | 19.77 | 24.65 | 26.61 | - | |

Considering the etiological agent of burns, only 264 out of 308 had information in the medical records about the agent who injured the hospitalized. It was found that the highest incidence was with explosive agents or the combustion of flammable substances, which affected 134 (43.51%) patients together. Of these, 94 (30.51%) were associated with liquid alcohol, the most frequent etiological agent. Then, 84 (27.27%) patients burned by overheated liquids, such as boiling water, fat and cooking oil. Soon after, 21 (6.82%) were burned by electricity and electric current, while 16 (5.19%) were burned in contact with a direct fire flame and 5 (1.62%) in contact with materials such as overheated household appliances, engines, machines and tools.
In this study, there were 88 pediatric patients, representing 28.57% of 308 cases. Of these 88 children, we had 56 (63.64%) burns from overheated liquids and contact with hot materials, 52 and 4 events, respectively. Electricity, direct flame and flammable substances, added, were the etiology of 23 (26.14%) burns in children.
Of the 308 events, 11 (3.57%) were from people who attempted self-extermination. In these 11 patients, the etiologic agent was the direct flame. All had second-degree burns, and only 2 had third-degree burns. The percentage of body surface burned in these records ranged between 10% and 60%. The average length of hospital stay between this group was 50.43 days, and the average age was 35.91 years, given that the patients were aged between 19 and 50 years. All had second-degree burns, and only 2 had third-degree burns. The percentage of the burned body surface in these records ranged from 10% to 60%. The mean length of hospital stay between this group was 50.43 days, and the mean age was 35.91 years, given that the patients were between 19 and 50 years old.
Regarding the percentage of body surface burned, only 285 events presented such records in the medical records. In 108 (35.06%) of them, patients had burns that affected between 10% and 20% of the body surface. At the same time, 78 (25.32%) were affected by burns on less than 10% of their body surface. 99 (32.14%) records recorded burns that exceeded 20% of the burned surface.
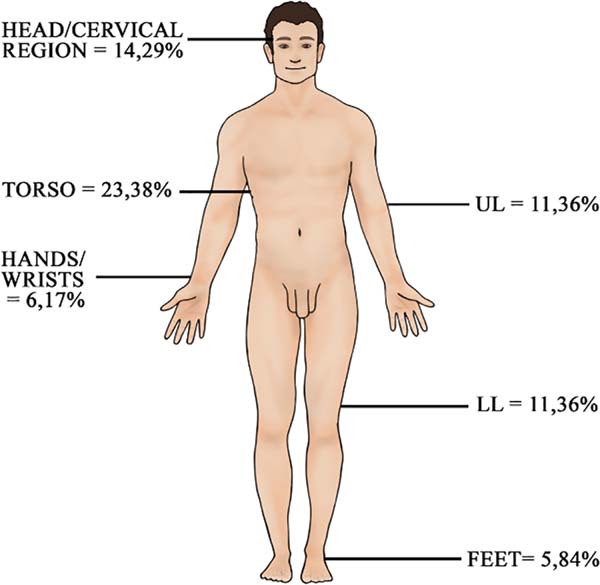
As for the burned body region, of the 308 events, 223 had information about this data. The most affected site was the trunk, with 72 (23.38%) patients burned at that location (Figure 1). Soon after, we have 44 (14.29%) injured in the head and neck. Then, we had 35 (11.36%) patients burned in shoulders and upper limbs without considering the wrist and hand. It was also found 35 (11.36%) patients burned in the hip and lower limb, without considering ankle and foot. There were 19 (6.17%) patients with burns on the wrist and hand, and those injured on the ankle and foot totaled 18 (5.84%). This information about the region was absent in 84 (27.27%) records.

DISCUSSION
Burns can produce physical and psychological sequelae, so the approach and management of this trauma can improve the patient’s quality of life7. In this sense, we must consider how severe the damage caused by burns is to the physical and psychosocial health of the person affected. Knowledge of epidemiology is important to guide burn patients’ management and carry out more effective prevention activities.
The prevalence of burns in males (59.02%), evidenced in this study, is according to the results cited by Bessa et al., In 20098, with 63.8% burned patients belonging to the male gender the Hospital Regional de Campina Grande (Paraíba-Brazil). Similar results were also found by Leão et al., In 20119, with 62.5% of hospitalizations due to burns belonging to the male gender. Macedo et al., In 201210, found 66% in their studies.
This study brings 74 patients (24.03%) under 9 years of age as the most affected age group, followed by those aged between 30 and 39 years, representing 61 (19.81%) events. Cruvinel et al., in 200511, in a similar study carried out in the city of Uberlândia/MG and in the same hospital in this study, also reached similar numbers. In his article, 29.85% of individuals were under 16 years old, followed by 24.46% adults between 31 and 40 years old. This showed that, despite the time difference, the most affected populations remain the same. Furthermore, Bessa et al. (2009) 8 remained in agreement with the majority of children and young adults, despite a greater number for children, 61.4% patients aged between 0 and 20 years and 23.9% for those between 20 and 40 years old. Leão et al. (2011) 9, in turn, obtained 37.6% for patients between 31 and 60 years old, the study’s main age group.
This study’s predominant ethnicity is brown since 48.38% of the patients declared themselves to be brown. In contrast, the data collected by Correa, in 199812, in the burn sector of the Hospital das Clínicas of the Faculty of Medicine of the University of São Paulo, burns prevailed in white individuals (71.74%) 12.
Regarding the period of hospitalization of the patients in this article, most of the burn patients (41%) remained hospitalized in the Unit for a period of 0 to 10 days, and the average total hospital stay was 26.61 days. Leão et al. (2011) 9 observed in their studies, at Hospital João XXIII, in Belo Horizonte/MG, an average hospital stays of 23.5 days. This data is close to the number found at HC-UFU.
Regarding the etiological agent, the results of this study are in accordance with the literature. The two agents with the highest incidence were alcohol (30.51%) and overheated liquids (27.27%). Leão et al. (2011) 9 obtained 34.4% and 28.1% for alcohol and overheated liquids, respectively. Bessa et al. (2009) 8 also presented close numbers, with 38% for alcohol and 32.5% for superheated liquids. Despite slightly larger data, Macedo et al. (2012) 10, also demonstrated burns by alcohol and overheated liquids, as the main causative agents, with 42% and 40% of patients, respectively. Still, Cruvinel et al. (2005) 11, in this same context, presented in their studies, 25.54% for alcohol and 21.22% for overheated liquids. This corroborates that the main etiologies remained in the two research periods at the same hospital.
Burned patients who attempted self-extermination are a complex problem, since they involve social and psychological aspects of these people¹³. In the present study, 11 (3.57%) events were attempts at self-extermination. Of these, 5 patients were males and 6 females. Leão et al. (2011) 9 obtained different data, presented 12% of hospitalized patients due to attempted suicide, 33% male and 66% female. Gimenes et al., in 200913, in their studies, found a rate of 7.5% of attempts at self-extermination of the total number of cases hospitalized with burns. In addition, both in this work and in that of Gimenes et al. (2009) 13, this condition’s etiology was the contact with the direct flame. The fact that this study was not carried out through the evaluation of physical records but, based on hospital discharge reports released by the HC-UFU statistics sector, may possibly justify the data discrepancies, especially in the disease of attempts at self-extermination concerning the other bibliographies analyzed.
Also, concerning patients who attempted suicide, a percentage of total body surface burning was observed, ranging from 10 to 60%. The 11 patients had second-degree burns and, even two of them also had third-degree injuries. The average age of affected people is 35.91 years. There was only one death.
Also, regarding attempts at self-extermination, Leão et al. (2011) 9 obtained an average of 40% of total body surface burned, the average age of 39 years and 51% of deaths. In the study by Calixto Filho and Zerbini, in 20167, on the epidemiology of suicides in Brazil, the data obtained corroborated with the findings in the present study and with those presented by Leão et al. (2011) 9. The highest incidence was in the age groups between 20 and 59 years of age7.
In the age group from 0 to 18 years old, 59.09% of the events had burns from overheated liquids, and this coincides with data from the literature, which consider these etiological agents as the most frequent in children and adolescents. Bessa et al. (2009) 8 observed scalding in 46.4% of patients younger than 20 years. The same agents were observed to be the most frequent by Leão et al. (2011) 9.
In this context, according to Rivera, in 200114, most burns in this age group occurred mainly at home with overheated liquids during food preparation or when serving them. Among the predisposing factors to appear burns in children, we can mention, for example, a child with a glass of overheated liquid that drops it in his arms while serving, the use of iron, environmental heaters, the shedding of the contents of pots in stoves for the cooking of food, and remembers, also, that children can burn the palm of hands by placing them on the lid of overheated ovens. Parents often have no idea that stove utensils can eventually be handled by a small child when they have no fixation or counterweight system. Prevention should focus especially on these mechanisms¹4.
As for the percentage of the total burned body surface, this study’s results were different from others. In this study, it was observed that 35.06% patients presented lesions with an extension between 10% and 20% of the body (medium extension), 25.32% below 10% (small extension) and 32.14% above 20% (large extension) extension) of the body surface. Bessa et al. (2009) 8 found for medium, large and small extent burned 63.2%, 18.4% and 18.4%, respectively. Macedo et al. (2012) 10 noted 45% of patients for medium burned extension, 31% for small burned extension and 24% for large burned extension. Gimenes et al. (2009) 13 in turn, reported 57%, 22% and 21% of patients with small, medium and large total body surface burned, exactly in that order.
Regarding the anatomical regions most affected, this study noted, firstly, the trunk injuries that affected 23.38% of the patients, and, secondly, the head and neck, present in 14.29% of the hospitalized. There was a considerable discrepancy with the references, namely that Cruvinel et al. (2005) 11 obtained, for the same hospital in this study, a preponderance for upper limbs with 19.7% and 17.82% for head and neck. In turn, Leão et al. (2011) 9 found a higher incidence in the anterior aspect of the chest in 60.2% of the patients, upper limbs in 53.8% and head in 51%. Bessa et al. (2009) 8, in their study, observed that burns mainly affected the upper limbs, followed by the chest. In the study by Gimenes et al. (2009) 13, found a higher incidence in the trunk with 62.7% and upper limbs in 60.4% of the patients analyzed.
CONCLUSION
It was found that accidents associated with the combustion of flammable substances affected 43.51% of the patients and, of these events, 94 were associated with liquid alcohol as the most frequent etiological agent of burns. According to Resolution No. 46 of the National Health Surveillance Agency (Anvisa), in February 2002, the manufacture and sale of ethyl alcohol in liquid form became prohibited15. In this context, it is necessary to promote preventive actions and inspect the trade in flammable products to reduce morbidity and mortality.
Besides, in the studies carried out at HC-UFU cited, more than 25% of the total number of burned patients treated, in the periods from 2000 to 2001 and from 2015 to 2019, belonged to the pediatric age group up to 18 years. Thus, it is possible to say that there is a tendency for pediatric patients to present themselves as the main victims of burns. Of the 88 children considered in this study, 63.64% had burns from scalding and contact with hot materials. Therefore, the importance of disseminating this information on pediatric traumas and continuously carrying out socio-educational campaigns prevents such accidents, thus reducing hospitalizations and mortality.
REFERENCES
1. Mélega JM, Viterbo F, Mendes FH. Cirurgia plástica: os princípios e a atualidade. Rio de Janeiro: Guanabara Koogan Ltda.; 2011.
2. World Health Organization (WHO). Burns [Internet]. Geneva: WHO; 2018; [acesso em 2020 Jun 23]. Disponível em: https://www.who.int/news-room/fact-sheets/detail/burns
3. Ministério da Saúde (BR). Queimados [Internet]. Brasília (DF): Ministério da Saúde; 2012; [acesso em 2020 Jun 23]. Disponível em: https://www.saude.gov.br/component/content/article/842-queimados/40990-queimados
4. Barcellos LG, Silva APP, Piva JP, Rech L, Brondani TG. Characteristics and outcome of burned children admitted to a pediatric intensive care unit. Rev Bras Ter Intensiva. 2018 Jul/Set;30(3):333-7.
5. Aragão JA, Aragão MECS, Filgueira DM, Teixeira RMP, Reis FP. Estudo epidemiológico de crianças vítimas de queimaduras internadas na Unidade de Tratamento de Queimados do Hospital de Urgência de Sergipe. Rev Bras Cir Plást. 2012;27(3):379-82.
6. Lei n° 8.069, de 13 de julho de 1990 (BR). Dispõe sobre o Estatuto da Criança e do Adolescente. Diário Oficial da União, Brasília (DF), 1990 jul 13: Seção 1.
7. Calixto Filho M, Zerbini T. Epidemiologia do suicídio no Brasil entre os anos de 2000 e 2010. Saúde Ética Justiça [Internet]. 2016 Dez; [citado 2020 Jun 28]; 21(2):45-51. Disponível em: http://www.periodicos.usp.br/sej/article/view/134006
8. Bessa D, Ribeiro A, Barros S, Mendonça M, Alves I, Alves M, et al. Perfil epidemiológico dos pacientes queimados no Hospital Regional de Urgência e Emergência de Campina Grande - Paraíba - Brasil. Rev Bras Ciênc Saúde [Internet]. 2009 Jul; 10(1):73-80. Disponível em: https://periodicos.ufpb.br/index.php/rbcs/article/view/3432
9. Leão CEG, Andrade ES, Fabrini DS, Oliveira RA, Machado GLB, Gontijo LC. Epidemiologia das queimaduras no estado de Minas Gerais. Rev Bras Cir Plást. 2011;26(4):573-7.
10. Macedo AC, Proto RS, Moreira SS, Gonella HA. Estudo epidemiológico dos pacientes internados na Unidade de Tratamento de Queimados do Conjunto Hospitalar de Sorocaba entre 2001 a 2008. Rev Bras Queimaduras. 2012;11(1):23-5.
11. Cruvinel SS, Queiroz DM, Recife FED. Epidemiologia de pacientes queimados atendidos no Hospital de Clinicas da Universidade Federal de Uberlândia no período 2000-2001. Biosci J. 2005 Mai;21(1):9-13.
12. Correa NA. Clínica cirúrgica. 4ª ed. São Paulo: Sarvier; 1998. v. 1.
13. Gimenes GA, Alferes FC, Dorsa PP, Barros ACP, Gonella HA. Estudo epidemiológico de pacientes internados no Centro de Tratamento de Queimados do Conjunto Hospitalar de Sorocaba. Rev Bras Queimaduras. 2009;8(1):14-7.
14. Rivera MG. Estudio anual prospectivo de las quemaduras infantiles em un área de la Región Metropolitana. Pediatria. 2001;17(5):349-53.
15. Ministério da Saúde (BR). Agência Nacional de Vigilância Sanitária (ANVISA). Resolução-RDC nº 46, de 20 de fevereiro de 2002. Brasília (DF): Ministério da Saúde/ANVISA; 2002.
1. Universidade Federal de Uberlândia, Faculty of Medicine, Uberlândia, MG, Brazil.
Corresponding author: Douglas Ravel Neto Diniz Ribeiro, Avenida João Pinheiro, 4604, Apt. 12, Umuarama, Uberlândia, MG, Brazil. Zip Code: 38405-307 E-mail: douglasdinizribeiro@hotmail.com
Article received: August 25, 2020.
Article accepted: January 10, 2021.
Conflicts of interest: none
COLLABORATIONS
DRNDR Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Project Administration, Software, Supervision, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing
SSC Supervision, Writing - Review & Editing
PAC Analysis and/or data interpretation, Conception and design study, Formal Analysis, Investigation, Methodology, Realization of operations and/or trials, Software, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing
HCOV Conception and design study, Conceptualization, Investigation, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing
TRBC Writing - Original Draft Preparation
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket