



Articles - Year 1998 - Volume 13 -
Use of the Pectoralis Musculocutaneous Flap with Exposed Pedicle for Face and Neck Reconstruction
Uso de Retalho Miocutâneo do Músculo Peitoral com Pedículo Exposto para Reconstrução de Face e Pescoço
ABSTRACT
The pectoralis major musculocutaneous flap is very important in face and neck reconstruction. First described with the use of a subcutaneous tunne1 lending to the defect through the neck, it's variation with use of an external pedicle is not widely reported. This study represents the number of patients that underwent surgery with pectoralis major musculocutaneous flap with external pedicle, in the Hospital de Clínicas de Porto Alegre from February 1991 to January, 1994. The data compared the advantages and complications with the literature wherein the internal pedicle technique is applied.
Keywords:
RESUMO
O RMC do músculo peitoral maior foi, e continua sendo, de grande importância na reconstrução de face e região cervical. Classicamente descrito com a realização de um túnel subcutâneo na região cervical, o uso deste retalho com a exteriorização de pedículo muscular é pouco difundido. Foram revisados os casos submetidos à reconstrução de face e região cervical no Serviço de Cirurgia Plástica do Hospital de Clínicas de Porto Alegre, no período de janeiro de 1991 a fevereiro de 1994 em que foram utilizados RMC com pedículo externo. São analisadas as vantagens e complicações do uso deste retalho comparando os dados obtidos com os de literatura, em que foi utilizado o pedículo interno.
Palavras-chave:
The pectoralis major musculocutaneous flap (MCF), primarily described by ARIYAN(1), is one of the main alternatives for face and neck reconstruction. This is basical1y due to its constant anatomy and for being a flap of easy execution(3).
Several studies have analyzed the use of this flap, describing the complications occurring in the type of reconstruction(1, 2, 10, 11).
A few variables must be analyzed when intending to study such complications, among these the flap aims, the lesion extension, and the long term patient's functional state (4, 5).
In the pectoralis muscle MCF, classically described(3), a subcutaneous tunnel is used, through which the musculocutaneous component is taken up to the defect to be corrected. Revisions about the pectoralis muscle MCF using exposed pedicle were nor found.
This paper dcscribes the experience in the use of this type of flap, showing the history cases, complications, and advantages of the pectoralis muscle MCF with exposed pedicle.
METHOD
All the cases of patients subjected to face and cervical reconstruction with musculocutaneous flaps of pectoralis muscle with exposed pedicle in the Plastic Surgery Service, CranioMaxillo-Facial Surgery Unit of the Hospital de C1inicas of Porto Alegre (HCPA) in the period of January, 1991 through January 1994, were revised.
The patients were analyzed as to the following characteristics: sex, age, number of performed flaps, reconstruction purpose, presence of concomitant bone defect, use of aloplastic material, surgical time, interval for the flap release, reconstruction moment, internation time, dressing type in the exposed pedicle, and complications of the procedure.
RESULTS
Of the 15 patients subjected to rotation of musculocutaneous flap of pectoralis muscle with exposed pedicle, 13 were operated by the resident surgeons of the Plastic Surgery Service, Cranio-Maxil1o-Facial Surgery Unit of the Hospital de C1inicas of Porto Alegre. The other two cases were operated by one of the service instructors.
The total amount of patients which took part in the sample was 15 individuals, 13 were male and 2 were female, with an average age of 62 years. A total of I7 flaps were prepared.
The musculocutaneou, flap was used to reconstruct a facial defect caused by neoplasia (case 1) in 13 patients.
One patient was subjected to surgery due to sequelae of paracoccidiodomycosis, and one patient presented high output arteriovenous malformation (case 2). Of these patients, 3 underwent the lower jaw reconstruction with plate: due to neoplasia, 2 presented detect due to parotidectomy, 2 underwent reconstruction of the mouth floor, one patient was operated because he presented exposed area of the common carotid artery, secondary to the neoplasic infiltration, and 7 patients for facial defects reconstruction.
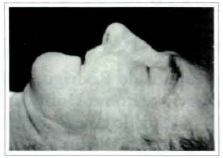
Fig. 1 - Patient with maxilar basocellular neoplasia.
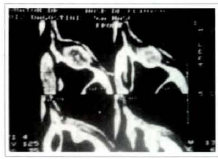
Fig. 2 - CT showing invasion of maxilar sinus.

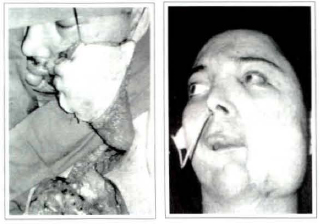
Fig. 3 - Post-ressection defect showing the maxilar sinus.

Fig. 4 - Correction after MCF rotation.
Case 2

Fig. 5 - Post-ressection defect in a high output arteriovenous fistula.
Figs. 6 & 7 - Result after MCF rotation.
Out of the 15 patients subjected to this procedure, in 2 flaps were used bilaterally, one for the mouth floor reconstruction due to paracoccidiodomycosis, and another for lower jaw reconstruction after total necrosis of the flap prepared two weeks earlier, at the same time of the tumor excision.
The revision of the cases showed that the necessary period for the flap preparation and for its accommodation in the defect to be corrected was of 2½ hours (+ 30 min.), the time necessary for the primary pathology excision being not included. Of the 17 prepared flaps, 15 occurred in the same anesthetic period for the basic sickness surgery and the other 2 flaps were prepared in another period, the first after total nectosis of the previous flap and the second after stabilization of high output arteriovenous malformation of the face. The medium period of hospital internation of these patients was of 33,3 days (5-150 days) and the average time in which the exposed pedicle releases were performed was of 28 days.
Among the complications found, a patient presented total necrosis of the flap used for the reconstruction of the mouth floor, 4 days after the procedure. Two weeks after the debridement, he was subjected to a new rotation of pectoralis muscle MCF, which presented total necrosis on the 5th postoperative day, so that the defect had been corrected by the use of a deltopectoral flap.
Other complications were partial necrosis in two patients, fistulae in three cases, infection in 4 patients.
Besides, a patient presented seroma and there was late exposition of the plate used for lower jaw reconstruction in another patient.
Of the 17 procedures in which the pectoralis muscle MCF with exposed pedicle was used, 5 received partial skin graft for the pedicle covering on the same surgical time of the reconstruction.
DISCUSSION
Several authors have reported their satisfaction with the short and long term results of the musculocutaneous flap of major pectoralis muscle(2). Many studies tried to identify factors which could forecast the flap viability. Factors such as tabaccoism(8),the inadequate flap handling, and the use of reconstruction plates(9), appeared prejudicial to the flap survival.
Other factors as sex, laboratory values, and other clinical variables have no statistically significative influence(8) for the flap viability.
There are also factors which are controversial, such as the patient's nutritional state, the previous irrad.iation(7, 8), and the size of the detect to be reconstructed(8).
The literature subdivides the complications with the MCF in larger and smaller. The smaller ones include limited process of infection, small dehiscence, partial necrosis of the flap and limited fistulae. The larger complications are represented by the total necrosis and/or permanent fistulae, imposing a new procedure.
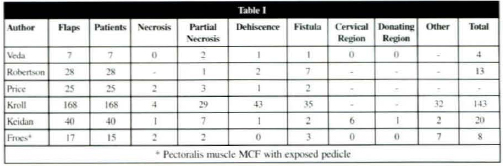
The literature revision shows that the complication indexes vary from 35 to 65 percent and the incidence of partial or total necrosis varies from 2 to 33 percent(6, 12), in case of rcconstruction with exposed pedicle. The results found in this study are comparable with the literature (Table 1). And it is more significant if we consider that most patients (13 out of 5) were operated by training surgeons (resident doctors).
The facial and cervical region defects reconstruction with the use of MCF of major pectoralis muscle with exposed pedicle has a few characteristics that must be put in relief. When analyzing the surgical time, we have observed that such procedure reduces considerably the operating time, since the time of the tunnel confection and of the accommodation of the flap are suppressed. Another important point is that a few complications of the tunnel confection, the hematoma, and the flap compression, for example, are discarded, reducing the risk as to the flap viability.
In the long term, the MCF with exposed pedicle presents a few advantages regarding the internal pedicle.
The muscular pedicle, being sectioned around 28 days(6) after the initial reconstruction, avoids an increase of volume in the preclavicular region.
Another factor observed in patients with MCF of major pectoralis muscle with internal pedicle is the retraction caused by the muscular atrophy. When the muscle begins the scarring process and atrophies itself, it starts to cause a cicatricial retraction in the tunnel region, which in a few cases forces the surgeon to reintervene, attacking the cervical region to release the fibrotic band. The muscular flap contraction was studied by SHINDO et al.(12), who noticed a conrraction in the muscular area of 41 to 45 percent of the tissue in all the patients.
The evidences showing the advantages of the use of the MCF of the pectoralis muscle with exposed pedicle are confronted with a few disadvantages. The procedure must count on the patients cooperation, especially with reference to the care with the head moving.
The muscular pedicle may be grafted or kept open with daily dressings up to its release. The patient must participate of the option, being informed of the advantages of grafting, since within 5 to 7 days the pedicle will be healed; he also must be aware of the disadvantages, since such procedure will require another dressing in the graft donor area and will involve an evenmal sequel. We must remind the patient that the grafting will not reduce his period of hospitalization, since his permanence in the hospital has the objective of observing eventual complicarions of the musculocutaneous component of the flap, which more commonly occur around the 5th to the 7th day Another important point to be observed, mainly in the first week, is the formation of "elbow" in the pedicle. This may cause a reduction in the blood flow and put the flap viability at risk. For this, in the first 5 to 7 davs, not only the patient, but also all the nursing team, are emphatically oriented as to the pedicle care.
The patient must also be informed that he shall be subjected to a new procedure after the flap integration.
This procedure will provide the pedicle section and give the final touch to the pedicle.
The case history of the patients operated in the Plastic Surgery Service of the HCPA, during the studies period, is small, but even so the pectoralis muscle with exposed pedicle flap may be an interesting alternative, especially in patients who need a long surgical time for the base pathology excision.
Randomized prospective studies, analyzing also the procedure cost, must be performed in order to compare the advantages of one or another technique to be employed.
REFERENCES
1. ARYIAN S. The Pectoralis Major Musculocutaneous Flap. Plast. Reconstr. Surg. 1979; 63: 7381
2. BAEK SM, LAWSON W, BILLER HF An Analsys of 133 Pectoralis Major Myocutaneous Flaps. Plast. Reconstr. Surg. 1982;69:460-467
3. BILLER HF, BAEK SM, LAWSON W, KRESPI YP, BLAUGRUND SM. Pectoralis Major Musculocutaneous Island Flap in Head and Neck Surgery. Arch. Otolaryngol. 1981;107:23-26
4. BRUSATI R, COLLINI M, BOZZETTI A, CHIAPASCO M, GALIOTO S. The Pectoralis Major Musculocutaneous Flap. J. Craniomaxilofac. Surg. 1988; 16:35-39
5. HUANG RD, SILVER SM, HUSSAIN A, PARNES SM, WING PD. Pectoralis Major Musculocutaneous Flap: Analysis of Complications in a VA Population. Head & Neck. 1992;14:102-106
6. IAN JACKSON. Por comunicação pessoal.
7. KEIDAN RD, KUSIAK JF Complications Following Reconstruction With The Pectoralis Major Myocuyaneous Flap: The Effect of Pior Radiation Therapy. Laryngoscope. 1992: 102
8. KROLL SS, REECE GP, MILLER MJ, SCHUSTERMAN MA. Comparison of the Rectus Abdominis Free Flap with the Pectoralis Major Musculocutaneous Flap for Reconstrctions of the Head and Neck. Am. j. Surg. 1992;164:615 618
9. MEHRHOF Al, ROSENSTOCK A, NEIFELD JP, MERRITT WH, THEOGARAJ SW, COHEN IK. The Pectoralis Major Musculocutaneous Flap in Head and Neck. Am. J. Surg. 1983;43:482
10. MAISEL RH, LISTON SL, ADAMS GL. Complications of Pectoralis Musculocutaneous Flaps. 1983;93:928-930
11. OSSOF RH et al. Complications After Pectoralis Major Musculocutaneous Flap Reconstruction of Head and Neck Defects. Arch. Otolaryngol. 1983;109:812-814
12. SHINDO ML, COSTANTINO PD, FRIEDMAN CD, PELZER HJ, SISSON GA, BRESSLER FJ. The Pectoralis Major Flap for Intraoral and Pharingeal Reconstruction. Arch Otolaryngol. Head Neck Surg. 1992;118:707-711
I - Resident Doctor from the Plastic Surgery Service of Hospital de Clinicas de Porto Alegre, Brazil.
II - Assistant Professor of the Surgery Department of Faculdade de Medicina da UFRGS, Brazil. Plastic Surgeon from the Plastic Surgery Service of Hospital de CHnicas de Porro Alegre, Brazil.
III - Plastic Surgeon from the Plastic Surgery Department of the Cranio-maxillo-facial Division of Hospital de Clinicas de Porto Alegre, Brazil.
Address for Correspondence:
R. Ramiro Barcelos, 2350 Porto Alegre - RS - Brazil
Phone: (55 31) 331.6699
Plastic Surgery Department, Cranio-maxillo-facial division of Hospital de Clinicas de Porto Alegre.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket