



Case Report - Year 2020 - Volume 35 -
Reduction cheiloplasty in bikini: case report
Queiloplastia redutora em biquíni: relato de caso
GIAN KARLO ALBERTO VIGO CASTRO1,* ; CESAR ANDRÉS BASTOS PLAZA1; FERNANDO SÉRGIO MENDES CARNEIRO1; GISELA HOBSON PONTES1; RONALDO PONTES1
; CESAR ANDRÉS BASTOS PLAZA1; FERNANDO SÉRGIO MENDES CARNEIRO1; GISELA HOBSON PONTES1; RONALDO PONTES1
ABSTRACT
Introduction: The lips are the central characteristic in the
lower third of the face, being essential for mimicry and facial
expression, speech, and swallowing, without forgetting the
aesthetic component. The presence of excessive large lips
(macroqueilia) represents an occasional but significant
challenge in plastic surgery. The technique called "bikini
reduction cheiloplasty," described in 2007, unlike the
techniques previously described, is focused on reducing lips
and restoring their anatomy, providing a more harmonious lip
contour.
Case Report: Male patient, 18 years old, black race
with a complaint of excessively large lips for whom surgical
treatment using the bikini technique was proposed, with
a good aesthetic result.
Conclusion: Based on the correct
indication and execution, we can conclude that the technique
of reducing cheiloplasty in bikini is a safe alternative, easy
to perform, and that provides a satisfactory aesthetic result.
Keywords: Face; Ambulatory surgical procedures; Case reports; Mouth; Lip.
RESUMO
Introdução: Os lábios são a característica central no terço inferior da face, sendo fundamentais para mímica e expressão facial, fala e deglutição, sem se esquecer do componente estético. A presença de lábios excessivamente grandes (macroqueilia) representa um desafio ocasional, mas significativo na cirurgia plástica. A técnica denominada "queiloplastia redutora em biquíni", descrita em 2007, à diferença das técnicas anteriormente descritas, não está focada apenas na redução de lábios, mas também na restauração da sua anatomia, proporcionando um contorno labial mais harmônico.
Relato de Caso: Paciente do sexo masculino, 18 anos, raça negra com queixa de lábios excessivamente grandes para o qual foi proposto tratamento cirúrgico usando a técnica do biquíni tendo um bom resultado estético.
Conclusão: Baseados na correta indicação e execução, podemos concluir que a técnica de queiloplastia redutora em biquíni é uma alternativa segura, de fácil execução e que proporciona um resultado estético satisfatório.
Palavras-chave: Face; Procedimentos cirúrgicos ambulatórios; Relatos de casos; Boca; Lábio
INTRODUCTION
The lips are the central characteristic in the lower third of the face1. It is one of the most significant facial features; they play a fundamental role in forming facial expressions. In the past, excessively large lips were an aesthetic issue among certain ethnic groups. Although full lips are a desirable characteristic sought by many people, the current world of fashion emphasizes balance and the significant correspondence of features, encouraging people to seek refinement through cosmetic surgery2.
The presence of excessively large lips (macroqueilia) represents an occasional but significant challenge in plastic surgery. It can interfere with oral function, with an inadequate seal between the upper and lower lips. It is more prevalent in certain ethnic groups, has multiple etiologies, and can affect one or both lips3.
The technique called “bikini reduction cheiloplasty,” described in 20074, differs from those previously described. We report a case with detailed preoperative planning and intraoperative surgical steps, not only focusing on the reduction of the lips but also on the restoration of their anatomy, providing a more harmonious lip contour.
OBJECTIVE
Disclose the technique of reduction cheiloplasty “in bikini” in a patient with excessively large lips.
CASE REPORT
18-year-old male patient, black, with complaints of excessively large lips. He denied associated comorbidities, smoking, and/or allergies.
Surgical technique
The patient’s marking is performed during the preoperative hospitalization as follows: with the lips closed at rest and after determining the midline, the upper lip’s contact point with the lower lip is marked, called points A - A ‘. With the lips slightly parted, the surgeon with the fingers pinches the upper lip 1 cm laterally to the “pillars of the filter,” gently rotating it inward to establish a more appropriate position4. Keeping the upper lip in this position, the same maneuver is now repeated on the lower lip to make them appear smaller in about 30% for the upper lip and 70% for the lower lip5. The new point of contact between the lips on the midline is marked, called points B - B ‘(Figure 1A). The design for the “bikini reduction cheiloplasty” technique can be established by determining these points. On the upper lip, the bikini top consists of a medial design of two parallel lines approximately 1 cm long through points A and B, which corresponds to the central band of the bikini. This band now diverges to form two oval domes. The apex of these domes’ anteroposterior dimension, called points C and D, must be twice the dimension A - B. The end of the marking must stop a few millimeters from the lip commissure.
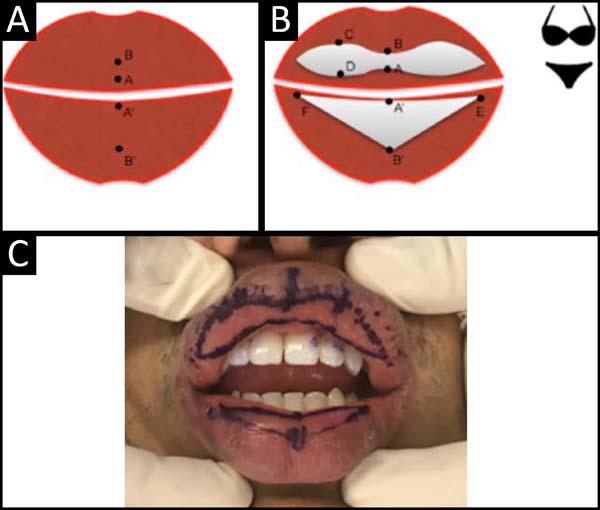

On the lower lip, the bottom of the bikini consists of the design of a triangle E - B ‘- F, where points E and F follow the same level as point A’ and must stop a few millimeters from the commissures (Figures 1B and 1C )5.
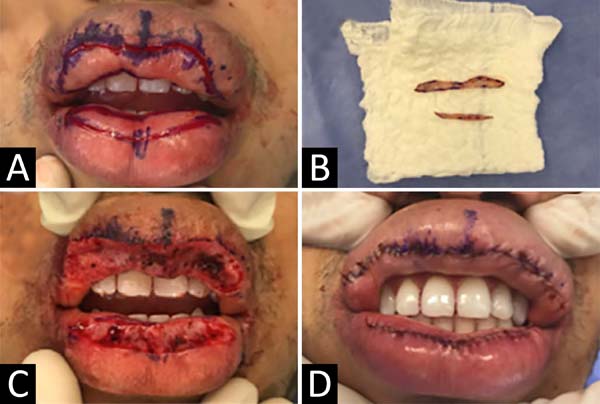
Surgery is started with the patient under sedation, with local infiltration of an anesthetic solution containing 60ml of 0.9% saline, 20ml of 2% lidocaine, 20ml of 7.5% ropivacaine, and 1ml of adrenaline 1: 1,000, resulting in a 1: 100,000 adrenaline concentration solution. The lip is pulled with the fingers in a two-finger maneuver to limit bleeding; the incision is then made according to the pre-established mark. The depth of tissue resection involves only the mucosa. The incision of the lower lip is performed similarly. Hemostasis must be meticulous, with the aid of electrocautery (Figures 2 A, 2B, and 2C). The main points (A - B, C - D, and A ‘- B’) will be approximated with simple 5-0 chrome catgut points; then the rest is performed by distributing the incision with continuous suture (running suture) with chrome catgut. 5- 0 (Figure 2D).

In the postoperative period, the use of PerioGard® as antibiotic prophylaxis for one week was indicated. Lip swelling was managed with cold compresses in the first two weeks, and Cicaplast Baume® was used in the second week to aid healing.
RESULTS
The patient presented marked lip edema for two weeks in the immediate postoperative period, being treated with cold compresses.
In the following 3-6 months, there was a significant improvement in volume and lip contour without altering the lip dynamics. The scar aspect was barely noticeable because it was on the inside of the lips. It was emphasized during the preoperative consultations that the final result could be observed after one year (Figure 3).


DISCUSSION
The main etiologies of macroqueilia are racial characteristics and biological inheritance. Other causes can be inflammatory diseases6, congenital malformations7, and iatrogenic procedures8. The use of the macroqueilia approach is described by Zanini et al. (2005)3 in the Melkersson-Rosenthal Syndrome, Hauben (1988)7 in the lip hemangiomas, Botti (2002)8 for correction of injection of alloplastic products and Niamtu (2010)9 in the various macroqueilias. It only consisted of excising a horizontal or vertical soft tissue wedge in the upper and lower lip to decrease their size, without paying attention to the contour, volume, and/or proportion between the upper and lower lips.
We propose that the “bikini” technique for approaching excessively large lips is considered more appropriate because addressing the lips’ volume also corrects the lip disproportion by giving aesthetic harmony.
CONCLUSION
Therefore, based on the correct indication and execution, we can conclude that the technique of reducing cheiloplasty in bikini is a safe alternative, easy to perform, and that provides a satisfactory aesthetic result.
REFERENCES
1. Maloney BP. Cosmetic surgery of the lips. Facial Plast Surg. 1996 Jul;12(3):265-78.
2. Sforza M, Andjelkov K, Zaccheddu R, Jovanovic M, Colic M. The "Brazilian" bikini-shaped lip-reduction technique: new developments in cheiloplasty. Aesthetic Plast Surg. 2012 Ago;36(4):827-83.
3. Zanini M, Martinez MAR, Machado Filho CDS. Síndrome de Melkersson- Rosenthal: relato de dois casos e revisão da literatura. Med Cutan Iber Lat Am. 2005;33(3):113-7.
4. Fanous N, Brousseau VJ, Yoskovitch A. The 'bikini lip reduction': A detailed approach to hypertrophic lips. Can J Plast Surg. 2007;15(4):205-10.
5. Maricevich P, Campolina AC, Sinder R, Mazzarone F, Pitanguy I. Sequela de injeção de silicone em lábio inferior: correção cirúrgica pela técnica do biquíni modificada. Rev Bras Cir Plást. 2014;29(1):172-5.
6. Popenko NA, Tripathi PB, Devcic Z, Karimi K, Osann K, Wong BJF. A quantitative approach to determining the ideal female lip aesthetic and its effect on facial attractiveness. JAMA Facial Plast Surg. 2017 Jul;19(4):261-7. DOI: https://doi.org/10.1001/jamafacial.2016.2049
7. Hauben DJ. Reduction cheiloplasty for upper lip hemangioma. Plast Reconstr Surg. 1988 Oct;82(4):694-7.
8. Botti G, Botti C, Cella A. A simple surgical remedy for iatrogenic excessively thick lips. Plast Reconstr Surg. 2002 Out;110(5):1329-34.
9. Niamtu J. Lip reduction surgery (reduction cheiloplasty). Facial Plast Surg Clin North Am. 2010 Feb;18(1):79-97. DOI: https://doi.org/10.1016/j.fsc.2009.11.007
1. Niterói D’Or Hospital, Plastic Surgery Service Prof. Ronaldo Pontes, Niterói, RJ,
Brazil.
Corresponding author: Gian Karlo Alberto Vigo Castro, Calle Contralmirante Villar, 619, Miraflores, Lima, Lima, Perú Zip Code: 15074. E-mail: gvc_1505@hotmail.com
Article received: December 02, 2018.
Article accepted: July 15, 2020.
Conflicts of interest: none
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket