



Case Reports - Year 2020 - Volume 35 -
Piezoelectric preservative rhinoplasty: an alternative approach for treating bifid nose in Tessier No. 0 facial cleft
Rinoplastia preservadora piezoelétrica: uma abordagem alternativa para tratamento de nariz bífido em fissura facial nº 0 de Tessier
Luiz Carlos Ishida1 ; Rodolfo Costa Lobato1,*; Bruno Ferreira Luitgards1; Marcelo José Monteiro Carvas1; Juan Felippe Guimarães Urcioli Mosquera de Rodriguez1; Rolf Gemperli1
; Rodolfo Costa Lobato1,*; Bruno Ferreira Luitgards1; Marcelo José Monteiro Carvas1; Juan Felippe Guimarães Urcioli Mosquera de Rodriguez1; Rolf Gemperli1
ABSTRACT
The bifid nose management in Tessier nº 0 facial cleft is controversial due to its characteristics, such as a wide bone vault, low dorsal height, excessive skin, soft tissues volume, and distant upper and lower lateral cartilages. Conservative rhinoplasty techniques, using piezoelectric instruments, can be a good option for the bifid nose treatment, as they preserve the roof and upper lateral cartilages and perform a more accurate osteotomy. We report the treatment of bifid nose in a 13-year-old boy with facial cleft No. 0, to whom was performed conservative rhinoplasty with the aid of piezoelectric material. Given the excess of skin and soft tissues, a completely external transcutaneous approach was chosen. For osteotomies, lateral fractures under direct piezo-assisted vision were performed to have better control of the bone vault narrowing. The upper lateral cartilages and the internal nasal valves were preserved and brought back to the midline with horizontal "U" sutures to obtain a projection of the cartilaginous vault. A large segment of skin and soft tissue was excised after narrowing the nasal vault. A year of follow-up shows a narrow bone pyramid, better projection, and tip definition, but persisting with a vertically short nose. Conservative rhinoplasty techniques, assisted by piezoelectrics, may be an option for bifid nose treatment, requiring long-term follow-up and a study with more cases.
Keywords: Nose; Nasal diseases; Rhinoplasty; Piezosurgery; Plastic surgery.
RESUMO
O manejo do nariz bífido na fissura facial de Tessier nº 0 é controverso devido às suas características, como uma ampla abóbada óssea, baixa altura dorsal, excesso de pele, volume de partes moles e cartilagens laterais superiores e inferiores distantes. Técnicas conservadoras de rinoplastia, utilizando instrumentos piezelétricos, podem ser uma boa opção para o tratamento do nariz bífido, pois preservam o teto e as cartilagens laterais superiores e realizam uma osteotomia mais precisa. Relatamos o tratamento de nariz bífido em um menino de 13 anos com fissura facial nº 0, no qual foi realizada a rinoplastia conservadora com auxílio de material piezoelétrico. Dado o excesso de pele e tecidos moles, optou-se por uma abordagem transcutânea completamente externa. Para osteotomias, fraturas laterais sob visão direta assistida por piezo foram realizadas para ter um melhor controle do estreitamento da abóbada óssea. As cartilagens laterais superiores e as válvulas nasais internas foram preservadas e reaproximadas à linha média com suturas em "U" horizontais, a fim de obter projeção da abóbada cartilaginosa. Um grande segmento de pele e tecidos moles foi extirpado após estreitamento da abóbada nasal. Um ano de acompanhamento mostra uma pirâmide óssea estreita, melhor projeção e definição de ponta, mas persistindo com um nariz verticalmente curto. Técnicas conservadoras de rinoplastia, assistidas por piezoelétricas, podem ser uma opção para o tratamento do nariz bífido, exigindo um acompanhamento a longo prazo e um estudo com mais casos.
Palavras-chave: Nariz; Doenças nasais; Rinoplastia; Piezocirurgia; Cirurgia plástica
INTRODUCTION
Facial cleft 0, described by Tessier, in 19761, can present with several alterations, including bifid nose, characterized by a wide and low nasal dorsum and bifid tip, which occur due to anatomical changes such as nasal bones and lateralized maxillary processes, horizontal upper lateral cartilages (ULC) and flat and hypoplastic wing cartilages, with malformed and asymmetric nostrils2.
Surgical correction of the bifid nose is usually performed with chisel osteotomies and structured rhinoplasty, using cartilaginous septal grafts to correct cartilaginous anomalies3,4.
Recent studies have shown that piezoelectric devices provide greater control in nasal osteotomies5,6. Some studies also emphasize the advantages of preservative rhinoplasty, such as avoiding an open roof, middle third collapse, and internal valve insufficiency 7,8.
This article reports the treatment of bifid nose in a patient with Tessier No. 0 facial cleft by preservative and piezo-assisted rhinoplasty.
CASE REPORT
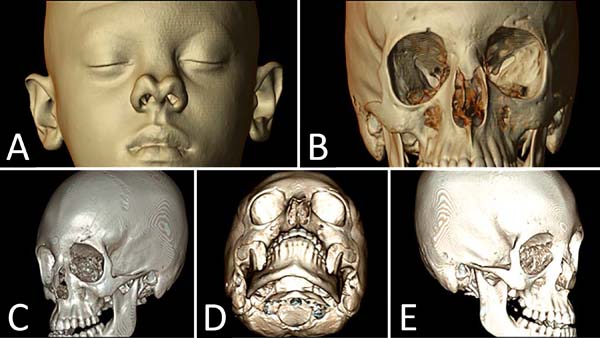
A thirteen-year-old boy with a bifid nose was referred to the plastic surgery department of our institution complaining about the dorsum and the nasal tip. In addition to the aesthetic complaint, the patient had psychological disorders due to social isolation and school bullying (Figure 1).


After computed tomography, he showed a bifid nasal tip, alar and ULC lateralized, and distant nasal bones, defining the diagnosis of facial cleft No. 0, with no frontal dysplasia findings (Figure 2).

He underwent surgical correction with access through a diamond-shaped incision on the nasal dorsum, removing the non-elastic skin from the same area and extending the incision to the columella. An excess of abnormal soft tissues was identified in the middle third of the nose, occupying an area above the septum (bifid) and between the ULC, making them horizontal and distant. Although the alar cartilages were lateralized, their domes were normoplastic and well defined (Figure 3).
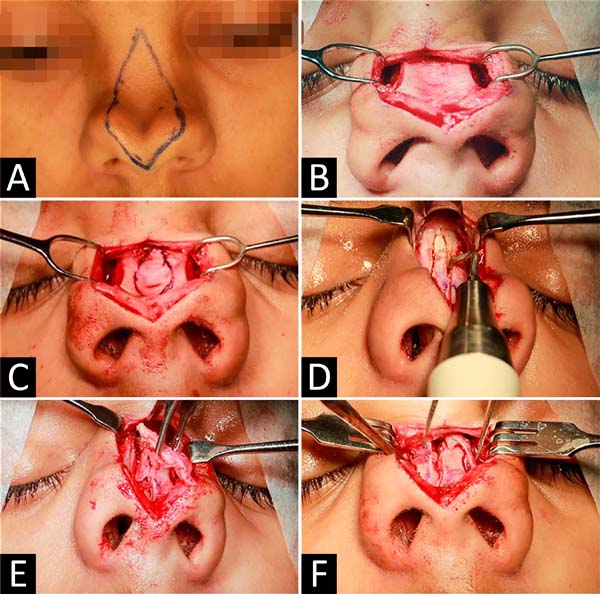

Despite being bifid, the nasal bones had a central spike that continued with the anomalous soft parts of the middle third. Both structures were resected: soft parts with a blade and bone part with piezoelectric, providing adequate exposure of the nasal bones and upper lateral cartilages.
The nasal bones were medialized through lateral and medial osteotomies, performed with a piezoelectric osteotome, to minimize damage to the structures.
The septal cartilage and ULC were preserved, without opening the cartilaginous roof, preserving the individual units of the internal nasal valve described by Saban, in 20187 and Ishida et al., In 19998. After detachment of zone K (separating the bone pyramid from cartilaginous), horizontal “U” sutures were performed, approaching the ULC that was horizontal and apart, narrowing the nose and raising the height of the nasal dorsum (Figure 4).
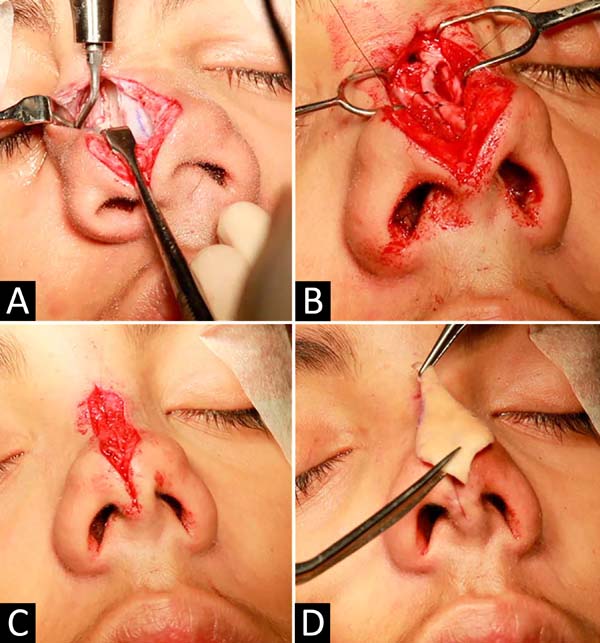

The treatment of the nasal tip was performed with interdomal points and between the medial crosses, and the primary closure of the surgical wound was performed in two planes, bringing together the soft parts preserved during the opening.
Standard postoperative care was performed, and the result after one year was satisfactory for the patient (Figure 5).


DISCUSSION
The bifid nose is part of the spectrum of midline facial malformations (Tessier No. 0-14) and may occur in isolation or associated with deformities of the lips, palate, and forehead9.
In this case, we present a 13-year-old patient with Tessier No. 0 facial cleft who had an isolated bifid nose, whose treatment initially proposed was orthognathic surgery and later rhinoplasty, but this was not accepted by the patient and family, who only wanted rhinoplasty.
It was tactically opted for external access through a diamond-shaped incision in the nasal dorsum, allowing broad access, dissection and visualization of redundant structures, resection of bone, and anomalous soft parts in the midline, as well as the use of piezoelectric instrumentation for osteotomies controlled.
The literature varies concerning the appropriate age and access to treat isolated bifid noses. According to Saied and El-Sherbiny, in 20114, access in these cases varies according to the degree of the deformity; in cases with a small separation of the domus, transcolumellar marginal access may be sufficient for adequate correction10. On the other hand, cases with greater separation of the tip and cartilaginous back require better visualization and resection of excess skin and soft tissues, with the incision on the nasal dorsum being the access of choice2,3,4,9.
We opted for access through the back as the patient had excess skin and, in our view, would not contract sufficiently after surgery if it were not resected. Despite the unpredictability of healing, especially in patients with black skin, other studies have shown similar maneuvers with good evolution2,3.
Regarding the tip, the alar cartilages were not fragile or hypoplastic, allowing treatment with interdomal sutures. On the other hand, the ULC was released from the K zone and medialized, without opening the cartilaginous roof, avoiding the violation of the elements of the internal nasal valve7,8.
In 20187 and Ishida et al., in 19998, Saban point out the advantages of preservative rhinoplasty, such as preservation of ULC and prevention of open roof and collapse of the middle third, which could occur in bifid noses after classical rhinoplasty3,4,9.
Regarding bone treatment, Ortiz-Monasterio et al., in 198710, demonstrated that osteotomies should be routine in cases of bifid nose, regardless of age. In this case, piezoelectric instrumentation was used for more controlled osteotomies and resection of the bony dorsum to tune the upper nasal third. This technique allows osteotomies with less ecchymosis and postoperative morbidity and more precise control of the height of the osteotomy with less bone comminution5,6.
A limitation of the case is the persistence of nasal shortening. In order to lengthen this type of nose, in our opinion, it would be necessary to use extended spacer grafts attached to a columellar strut, in addition to dorsal grafts, but we chose not to violate the septal cartilage to collect them at this time. This could be done in a surgical review, but the patient is satisfied with the height of the back achieved and does not admit further interventions.
Conservative and piezoelectric-assisted rhinoplasty is an alternative approach for treating the bifid nose and has not yet been described in the literature. Long-term follow-up and more cases are needed to prove its efficiency in treating bifid nose.
* All photos were authorized by the minor’s father, who signed the Free and Informed Consent Term and the photos’ publication term.
REFERENCES
1. Tessier P. Anatomical classification of facial, crânio-facial and látero-facial clefts. J Maxillofac Surg. 1976 Jun;4(2):69-92.
2. Kolker AR, Sailon AM, Meara JG, Holmes AD. Midline cleft lip and bifid nose deformity: description, classification, and treatment. J Craniofac Surg. 2015 Nov;26(8):2304-8.
3. Ozturk S, Zor F, Isik S. Surgical correction of severe bifid nose. J Cleft Lip Palate Craniofac Anomal. 2014;1(2):115-8.
4. Saied S, El-Sherbiny A. Algorithm for aesthetic reconstruction of the bifid nose in tessier number 0 cleft. J Plast Reconstr Surg. 2011 Jul;35(2):187-90.
5. Gerbault O, Daniel RK, Kosins AM. The role of piezoelectric instrumentation in rhinoplasty surgery. Aesthet Surg J. 2016 Jan;36(1):21-34.
6. Ilhan AE, Cengiz B, Eser BC. Double-blind comparison of ultrasonic and conventional osteotomy in terms of early postoperative edema and study design and patient selection. Aesthet Surg J. 2016 Abr;36(4):390-401.
7. Saban Y, Daniel RK, Polselli R, Trapasso M, Palhazi P. Dorsal preservation: the push down technique reassessed. Aesthet Surg J. 2018 Feb;38(2):117-31.
8. Ishida J, Ishida LC, Ishida LH, Vieira JC, Ferreira MC. Treatment of the nasal hump with preservation of the cartilaginous framework. Plast Reconstr Surg. 1999 Mai;103(6):1729-33;discussion:1734-5.
9. Miller PJ, Grinberg D, Wang TD. Midline cleft: treatment of bifid nose. Arch Facial Plast Surg. 1999 Jul/Set;1(3):200-3.
10. Ortiz-Monasterio F, Fuente del Campo A, Dimopulos A. Nasal clefts. Ann Plast Surg. 1987 Mai;18(5):377-97.
1. Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo,
São Paulo, SP, Brazil.
Institution: Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo, São Paulo, SP, Brazil.
LCI Analysis and/or data interpretation, Conception and design study, Final manuscript approval, Writing - Original Draft Preparation
RCL Conceptualization, Investigation, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing
BFL Data Curation, Final manuscript approval, Investigation, Realization of operations and/or trials, Writing - Review & Editing
MJMC Conceptualization, Realization of operations and/or trials, Supervision, Writing - Review & Editing
JFGUMR Conceptualization, Final manuscript approval, Investigation, Methodology, Writing - Original Draft Preparation
RG Conception and design study, Conceptualization, Supervision, Visualization, Writing - Review & Editing
Corresponding author: Rodolfo Costa Lobato, Rua Doutor Melo Alves, 55, Cj 23, Cerqueira Cesar, São Paulo, SP, Brazil. Zip Code: 01417-010. E-mail: rodolfolobato49@yahoo.com.br
Article received: May 13, 2019.
Article accepted: June 22, 2019.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket